
Abstract
Background and Objective:
Ambulatory holmium laser enucleation of prostate (HoLEP) has shown low rates of readmission and postoperative complications. However, the patient’s experience has been undervalued. We aimed to measure the patient’s perceived fear and anxiety during ambulatory HoLEP.
Methods:
We performed a prospective study on patients scheduled for HoLEP at our institution. We excluded patients with cognitive or psychiatric disorders and those who had to be hospitalized. The week preceding the surgery, we administered the Surgical Fear Questionnaire (SFQ) and the Hospital Anxiety and Depression Scale (HADS) by phone. The day following the surgery, we readministered the HADS and asked the patients if they would undergo HoLEP in the same setting.
Key Findings and Limitations:
Overall, 70 patients completed the study (mean age 72.3, standard deviation [SD] 6.5 years). The mean SFQ score was 18.4/90 (SD 13.5); the two highest rated items were “I am afraid of pain after the operation” and “I am afraid of unpleasant side effects after the operation.” with a mean of 3.7/10 and 2.7/10, respectively. For the HADS, the mean preoperative score was 4.6/21 (SD 3.4), and the mean postoperative score was 3.9/21 (SD 3.0), with a mean difference of −0.7 (p = 0.059). The majority (90%) of patients reported they would undergo HoLEP in the same setting.
Conclusions and Clinical Implications:
Most patients described low levels of anxiety and fear, and would undergo ambulatory HoLEP again. Given the high satisfaction and low levels of anxiety, widespread adoption of ambulatory HoLEP should be considered.
Patient Summary:
Men with benign prostatic hyperplasia, or an enlarged prostate, often need surgery to improve urinary function. We studied the acceptability of same-day discharge surgery for this condition by assessing patients’ anxiety, fear, and willingness to repeat the procedure. Most patients described low levels of anxiety and fear, and would undergo ambulatory HoLEP again.
Introduction
Anatomical endoscopic enucleation of the prostate (AEEP) 1 has revolutionized the management of lower urinary tract symptoms due to benign prostatic hyperplasia (BPH). This minimally invasive procedure has shown to reduce bleeding, catheter time, and length of the hospital stay. 2 –4 Although the learning curve may be challenging, this size-independent technique 5 is now regularly performed in the ambulatory setting with low rates of readmission and postoperative complications, and exhibits excellent functional results. 6 –9 Patient satisfaction was found to be 90.5%–95.2% at 6 months after outpatient AEEP using a holmium laser. 10–11 However, the patient’s experience during AEEP has been undervalued.
Because of the stressful nature of undergoing a surgery and the apprehension that comes with a loss of consciousness due to anesthesia, having trust in one’s surgical team and being well informed is essential. More than one third of patients would desire anxiolytic medication prior to surgery. 12 A patient’s anxiety in the days leading up to surgery seems to influence the intensity of the pain they experience after the surgery. 13 For certain surgeries, excessive preoperative stress could increase postoperative morbidity and mortality. 14,15 Education and preparation of patients could increase satisfaction and reduce pain after the surgery, but not necessarily anxiety. 16 Regarding BPH surgeries, such as inpatient transurethral resection of the prostate (TURP), personalized preoperative education has been shown to significantly reduce postoperative anxiety and pain.
Nevertheless, there are limited data regarding the anxiety and fear patients feel when undergoing ambulatory urological surgery. Hence, there are numerous questions: what does a patient experience when undergoing AEEP? Does the ambulatory nature of the surgery increase fear and anxiety in the patient? To address these questions, our objective was to prospectively measure the patient’s perceived fear and anxiety during ambulatory holmium laser enucleation of prostate (HoLEP).
Methods
Study design and population
This prospective study involved patients requiring HoLEP at our teaching hospital from March 2021 to March 2024. Patients with psychiatric disorders, cognitive impairments affecting their ability to respond accurately to questionnaires, and/or failed ambulatory surgery—defined as readmission within 2 days postsurgery—were excluded from the study. The study protocol was approved by the institutional review board (databank 2022-4463).
Preoperative consultation
During the preoperative consultation, each patient received verbal information from the surgeon performing HoLEP and a document summarizing their prostate disease, the surgery, the anesthesia, and the possible aftereffects, such as the risks of sepsis, hematuria, incontinence, anejaculation, and urethra or bladder neck strictures. Postoperative pain was not routinely discussed and did not appear in the handout. Antiplatelet and anticoagulant medications were suspended before surgery, unless otherwise advised by the preoperative internal medicine team.
Data collection
During the week preceding the surgery, the Surgical Fear Questionnaire (SFQ) and the Hospital Anxiety and Depression Scale (HADS), anxiety subscale (Supplementary Data) were administered by phone to each patient. The day following the surgery, the HADS was readministered via phone call. Both phone calls were made by an independent member of the research team. Each patient was also asked whether they would undergo HoLEP in the same ambulatory setting. The response options included “not at all,” “yes, but with more information,” and “yes, in the same setting” (Supplementary Data). All data were collected prospectively. In addition, data related to the patient’s preoperative characteristics were collected—including a history of previous surgeries, the International Prostate Symptom Score (IPSS), quality of life (QoL) questionnaire score, uroflowmetry, and postvoiding residual volume (PVR).
Questionnaires
The SFQ is a validated survey comprising 10 items that assess the level of a patient’s fear regarding different aspects related with a surgical procedure. Item 8 (“I worry about my family”) was removed because it is not particularly relevant to ambulatory surgery. Each item is assessed using a Likert scale from 0 to 10, indicating the extent of fear experienced by the patient for each item. A rating of 0 signifies a complete absence of fear, while 10 indicates a significant level. Items 1–4 are associated with fear of the short-term consequences of surgery, while items 5–10 are associated with fear of the long-term consequences of surgery.
The HADS questionnaire, anxiety subscale, comprises seven questions that evaluate different manifestations of anxiety that patients could experience prior to surgery. Each item is rated on a Likert scale from 0 to 3, where 0 indicates no anxiety and 3 indicates anxiety most of the time. The total score ranges from 0 to 21 points, with a score of 8–10 considered to be borderline abnormal and a score greater than 11 considered to be abnormal.
Technique and postoperative care
All surgeries were performed by the same surgeon. The details regarding the “en bloc” HoLEP technique and the postoperative protocol have been described previously. 8 Each patient lived less than 1 hour away from any hospital and was asked to be accompanied the first night after surgery. At the time of discharge, patients were informed of (1) a number to call if they needed assistance during “business hours.” (2) a urology team was on call, and (3) they would be contacted by the local community care centers for catheter removal the next day.
Statistical analysis
Prior to performing the study, a power analysis was performed using G Power to determine the required sample size to detect a difference of 1 point between the preoperative and postoperative mean HADS score, with a standard deviation (SD) of 3. 17–18 With statistical power of 0.80 and an alpha level of 0.05, 70 participants would allow detecting this difference with a paired t-test and a small effect size (Cohen’s d = 0.30).
SPSS Statistics Version 28 (IBM Corp., Armonk, NY) was used for statistical analysis. A descriptive analysis of the HADS and SFQ scores, and the question regarding willingness to undergo HoLEP in the same ambulatory setting was performed. A paired t-test was used to compare the difference between the preoperative and postoperative HADS scores. Subsequently, subgroup analyses were performed for the SFQ and preoperative and postoperative HADS scores using independent-samples t-tests. The participants were divided into groups based on age (<70 or ≥70 years), preoperative retention (yes or no), longer duration of retention (≤10 or >10 months), 8 past surgeries (yes or no), and type of anesthesia (general or spinal) used during surgery. A p value <0.05 was considered to be statistically significant.
Results
A total of 82 patients underwent HoLEP, with 92.9% (76/82) of them having a successful ambulatory surgery. Hematuria was the only cause of ambulatory failure and no patient was hospitalized because of the anxiety of having to go home the same day. We excluded four patients before the intervention and an additional eight patients after the surgery, resulting in 70 patients meeting the eligibility criteria and included in our final analysis (Fig. 1).
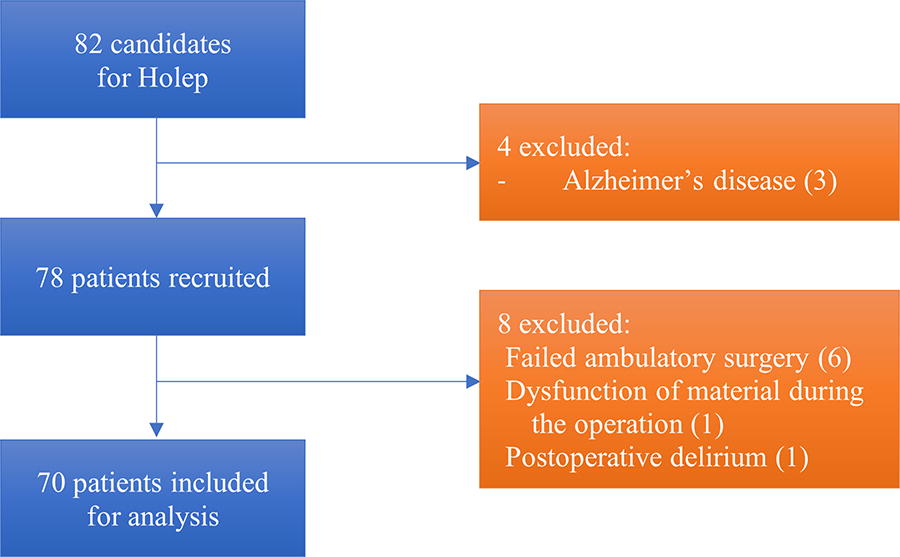
Study flow chart.
The median age was 72.3 (SD 6.5) years. The majority of the patients had urinary retention (68.6%, 48/70). Intermittent catheterization was slightly more prevalent than indwelling catheter use (54.2% [26/48] vs 45.8% [22/48]). The average prostatic volume was 109.7 (SD 42.3) g, with a mean Qmax of 8.35 (SD 6.5) mL/s and a mean PVR of 209.6 (SD 158.8) mL. The mean IPSS was 16.8 (SD 6.9) and the mean QoL score was 4.4 (SD 1.6). Table 1 presents the preoperative characteristics of the patients.
Preoperative Characteristics
IPSS = International prostate symptom score; IQR = interquartile range; SD = standard deviation.
As shown in Table 2, the mean preoperative SFQ score was 18.4/90 (SD 13.5). The two highest rated items were “I am afraid of pain after the operation” and “I am afraid of unpleasant side effects after the operation,” with a mean of 3.7/10 (SD 2.8) and 2.7/10 (SD 2.7), respectively. The mean preoperative HADS score was 4.6/21 (SD 3.4) and the mean postoperative HADS score was 3.9/21 (SD 3.0) points, with a mean difference of −0.7 (p = 0.059). Only 4.3% (3/70) of the patients had a clinically significant preoperative HADS score (>10 points) and 1.4% (1/70) postoperative. Figure 2 exhibits the distribution of the preoperative and postoperative HADS scores. Finally, 90.0% (63/70) of the patients indicated they would undergo HoLEP again in the same ambulatory setting, while 8.6% (6/70) would undergo HoLEP again, but under different conditions.
The Surgical Fear Questionnaire and Hospital Anxiety and Depression Scale, Anxiety Subscale Scores
The total Surgical Fear Questionnaire score is 90 points, and the total Hospital Anxiety and Depression Scale, anxiety subscale is 21 points. Patients with clinically significant anxiety had a Hospital Anxiety and Depression Scale, anxiety subscale score of >10 points.

Distribution of the
In the subgroup analysis, there were no significant differences in SFQ and preoperative and postoperative HADS scores (details are exhibited in Table 3).
Subgroup Analysis of the Surgical Fear Questionnaire and Hospital Anxiety and Depression Scale, Anxiety Subscale Scores
HADS = Hospital Anxiety and Depression Scale; SFQ = Surgical Fear Questionnaire.
At 3 months after HoLEP, 98.6% (69/70) of the patients were catheter free. The mean IPSS was 6.5 (SD 4.9), the mean QoL questionnaire score was 1.5 (SD 1.6), the mean maximum flow rate was 19.8 (SD 9.8), and the mean PVR was 67.1 (SD 809) mL.
Discussion
In our study, patients undergoing ambulatory HoLEP described low levels of fear or anxiety, both the week before and the day after the surgery. Moreover, only a very small percentage of the sample exhibited clinically significant anxiety based on the HADS score. Additionally, the two highest rated items were “I am afraid of pain after surgery” and “I am afraid of side effects after surgery.” Interestingly, considering that 68.6% of our patients were catheter dependent, the mean score of the item ‘I am afraid that the operation will fail’ was only 1.3/10.
It is essential to measure and identify ways to reduce preoperative anxiety because it could be associated with higher postoperative mortality after certain surgeries, 19 consumption of analgesics, postoperative pain, as well as prolonged recovery from anesthesia and hospital stay. 13,20,21 Anxiety could affect daily life or it could only occur when a stress factor is added. Preparing for surgery is stressful: based on data from 2001 to 2019, the global pooled prevalence of preoperative anxiety among surgical patients was 48%. 20 When using the Amsterdam Preoperative Anxiety and Information Score, the prevalence of anxiety ranged from 40.5% to 58.1%. 22,23
There are several anxiety questionnaires. We used the HADS, which has been shown to perform well to evaluate anxiety in the general population. 24 Many researchers have aimed to evaluate a patient’s anxiety before surgery or anesthesia; they have often considered different populations, questionnaires, and/or different surgeries, which makes a direct comparison among the studies inaccurate. Focusing on ambulatory surgeries, Jiwanmall et al. 23 found that 58% of patients had preoperative anxiety. To the best of our knowledge, our study is the first to evaluate the patient’s perioperative stress and anxiety regarding ambulatory HoLEP. In the preoperative questionnaire, item 8 (“I worry about my family”) in the SFQ was removed since we considered the procedure to be a minimally invasive endoscopic, with a low risk of mortality. In our experience, this concern did not emerge during preoperative discussions with patients. Therefore, we were cautious about including this item, as it could potentially bias the SFQ to a lower level of fear.
The patients showed high satisfaction with the procedure: 90% stated they would undergo the surgery in the same setting. Jeong et al. 10 and Lee et al. 11 have also reported a high willingness of patients to undergo HoLEP again (94%–98%). However, in their cohorts, the patients were hospitalized and the evaluation was performed 6 months after the surgery. Moreover, they focused on patient satisfaction regarding the functional results rather than the surgical setting.
A few studies have focused on anxiety in patients undergoing endoscopic prostate surgery; the authors found that overall, the patients were moderately stressed. 25,26 Nottingham et al. 26 retrospectively identified that 32% of patients had anxiety prior to HoLEP, among which only 7.5% had severe anxiety (based on a Generalized Anxiety Disorder-7 score ≥15). There was no change in patient-reported anxiety before and after HoLEP. However, the authors did not specify the duration between the preoperative visit and HoLEP, nor the surgical setting (inpatient or outpatient), and the postoperative questionnaire was completed 3 months after the surgery. Evaluating perioperative anxiety in context of TURP, Peng et al. 25 found a median HADS anxiety score of 9 (interquartile range 5–12) in the routine care group, which is slightly higher than our study but still under the significant anxiety score cut-off of 11 points. In their randomized study, they showed that by developing a supportive environment and involving the patient in decision-making, the anxiety level significantly decreased at 1 and 3 months after surgery compared with baseline.
According to Statistics Canada, in 2022, the 12-month prevalence of generalized anxiety disorder among Canadians older than 65 years was <2.5%. 27 Our cohort represents men with an average age of 72 years and from a medium-sized city in Canada. We can assume that the prevalence of generalized anxiety disorder in our population is fairly low. In addition, our patient education handout and the fact that the procedure was minimally invasive could explain why only 4.3% of the patients had clinically significant anxiety the week preceding HoLEP.
In the preoperative consultation with the surgeon, patients were informed about the ambulatory HoLEP procedure, the day’s course, the types of anesthesia, and possible complications such as sepsis, hematuria, incontinence, anejaculation, or urethral and bladder neck strictures. They were also informed that while a few patients may fail the postoperative catheter weaning test, most will be catheter-free at 3 months, which is definitely reassuring. Patients’ expectations were moderated for those at higher risk of weaning failure, particularly due to hypocontractile bladder and high volume of preoperative urinary retention (urodynamic evaluation is not routinely performed to all patients). In our facility, patients with a prostate volume greater than 80 g are systematically referred for HoLEP. Prostate embolization was the sole alternative that was discussed with the patients, since open simple prostatectomy is no longer performed in our institution and mini-invasive surgical procedures (MIST) were not available at the time of the study.
Similarly to our findings, studies have found that “pain after surgery” seems to be what worries patients the most, 16,28 while a meta-analysis showed that “fear of complication” was the main independent predictor of preoperative anxiety. 29 Preoperative specific preparations have not consistently demonstrated their effectiveness in reducing fear or worry, confirming that anxiety could be difficult to manage. Ortiz et al. 16 added handouts as part of the preparation for surgery, and Peng et al. 25 added specific information addressing fears before TURP without reported differences compared to the routine care group.
None of the patients in our cohort expressed a desire to remain hospitalized because of stress or anxiety at the time of discharge. The sole cause of ambulatory failure was hematuria and we excluded these patients. We designed our postoperative protocol to reduce anxiety and to provide the patients with the resources required in the event of a problem. We postulate that these efforts reduced the postoperative anxiety rate (only 1.4% of the patients had a clinically significant HADS anxiety score).
We did not identify significant differences in anxiety for any of the subgroups we considered. A 2020 meta-analysis identified that preoperative anxiety could depend on age, gender, the educational level, the type of surgery, and the fear of financial loss, among other factors. 20,30 On the other hand, previous anesthesia or surgical experience significantly reduce preoperative anxiety, but we were unable to confirm these findings, probably due to the very low rate of anxiety in our cohort.
Our study has several limitations. First, we examined a cohort limited to a single surgeon and center in Canada, which makes the results difficult to extrapolate to other contexts. Second, long delays before HoLEP might have reduced the stress among catheter-dependant patients who were eager to undergo the operation, although this did not translate into statistically significant results. Third, it would have been ideal to administer the HADS questionnaire the day before the surgery, but due to logistical reasons and the availability of the research team, we considered the week before to be acceptable. Finally, although 70 patients represent a small sample, our study was powered to detect a difference of 1 point between the preoperative and postoperative mean HADS scores.
Conclusion
We showed that the majority of patients reported minimal anxiety and fear during ambulatory HoLEP. Moreover, the vast majority of patients indicated that they would undergo ambulatory HoLEP again in the same setting. Despite the low level of fear, preoperative discussions could focus more on postoperative pain and side effects to reassure patients. Given the low levels of anxiety and complications, along with excellent functional outcomes, widespread adoption of ambulatory HoLEP should be considered.
Footnotes
Acknowledgments
The authors would like to thank Samuel Lemaire-Paquette, statistician from the research center of the CHUS, for his support in the development of statistics and contribution to the elaboration of the statistical analysis subsection of the article. The authors would also like to express gratitude to Dr Robert Sabbagh, Dr Claudio Jeldres, and Dr Michel Carmel of their urology department, for measuring prostate volumes by ultrasound during HoLEP workup.
Authors’ Contributions
S.B., A.M., and S.L.: Conceptualization. S.B., A.M., M.-A.B., and S.L.: Acquisition of data. S.B., A.M., and S.L.: Methodology. S.B., A.M., and S.L.: Writing—original draft preparation. S.B. and S.L.: Writing—review and editing. S.B. and S.L.: Supervision. All authors have read and agreed to the published version of the article.
Author Disclosure Statement
The authors have nothing to disclose.
Funding Information
This research received no external funding.
Supplementary Material
Supplementary Data
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.