
Abstract
Introduction and Objectives:
Renorrhaphy during partial nephrectomy is technically challenging and can extend the warm ischemia time (WIT). This study investigates the use of Veriset™ as an alternative to renorrhaphy in robot-assisted partial nephrectomy (RAPN) and presents our findings.
Methods:
In this retrospective analysis, 43 patients who had Veriset patch placed on the tumor bed post resection were compared against 43 patients who underwent conventional single-layer renorrhaphy for RAPN from January 2023 to January 2024 at our institution. The two groups underwent propensity score matching based on age, body mass index, and R.E.N.A.L. nephrometry score. Data of all patients, including patient demographic details, tumor characteristics including size, location, pre- and postoperative blood investigations, intraoperative findings, blood loss, postoperative course, complications, and follow-up of 6 months duration, were recorded.
Results:
The mean age of the study population was 52.62 ± 13.31 years, and the mean nephrometry score was 6.64 ± 1.91. The Veriset patch application failed in three patients (6.97%) and cortical renorrhaphy had to be performed for hemostasis. The Veriset group (VG) had significantly less console time and WIT when compared with renorrhaphy group (RG) (82.02 ± 25.17 minutes and 11.95 ± 10.02 minutes, respectively, vs 95.53 ± 29.80 minutes and 17.63 ± 6.59 minutes; p = 0.014 and p < 0.001, respectively). The RG witnessed a significant reduction in estimated glomerular filtration rate (eGFR) on postoperative day 1 as opposed to VG (−7.56 ± 15.89 mL/min/1.73 m2 vs −0.21 ± 11.12 mL/min/1.73 m2; p = 0.015). The intraoperative blood loss, need for blood transfusion, postoperative change in hemoglobin rates, readmission, and renal function at 6 months in the VG and RG were comparable.
Conclusions:
The Veriset application instead of renorrhaphy led to reduced WIT, decreased console time, and early return of renal function with no significantly increased rate of complications.
Introduction
Partial nephrectomy is the standard of care for small renal masses. 1 It is a complex surgical procedure that involves both extirpation of the renal tumor and reconstruction of the residual renal parenchyma with minimal warm ischemia time (WIT). 2 Renorrhaphy is an essential component of this operation, which helps attain hemostasis. However, suturing of the renal parenchyma is technically challenging and time-consuming; it is likely to prolong the WIT. 1 Since WIT has a direct impact on postoperative renal function, surgical technique modifications have usually focused on minimizing the WIT without compromising on the oncological outcomes. 3,4 Furthermore, literature reports indicate that suturing of renal parenchyma during renorrhaphy may potentially harm intraparenchymal vessels, resulting in the formation of renal artery pseudoaneurysms that could lead to serious complications. 4,5 In order to overcome this challenge, closure of the renal parenchyma in a suture-free manner using topical hemostatic agents has been explored. Veriset™ patch is one such hemostatic agent that demonstrated promising results when used in hepatic and vascular surgeries. 6,7 The Veriset hemostatic patch, developed by Covidien Inc. in Mansfield, MA, USA, is a topical hemostatic agent consisting of an oxidized cellulose infused with buffer salts, trilysine, and polyethylene glycol (PEG) sourced from nonanimal origins which is absorbed within 4 weeks post application. 8 There is limited literature reporting the use of this agent for robot-assisted partial nephrectomy (RAPN). Erne et al. used this patch as an alternative to parenchymal suturing in laparoscopic partial nephrectomy. 8 With this background, we explored the use of Veriset patch as an alternative to renorrhaphy for RAPN and report our experience here.
Materials and Methods
A total of 120 patients underwent RAPN from January 2023 to January 2024 in our institution and were enrolled in the study. Approval of the institutional ethics committee of Aster Medcity Kochi (AM/EC/356-2023) was taken prior to commencing the study. The data of these patients was collected prospectively. Patients with a solitary renal mass on imaging and a normally functioning contralateral kidney were included in the study. Exclusion criteria were patients with massive breach of pelvicalyceal system (PCS) such as breach of two or more renal calyces/pelvis, multiple renal masses, patients on dual antiplatelets, and chronic liver disease. Data of all patients including patient demographic details, tumor characteristics including size, location, pre- and postoperative blood investigations, R.E.N.A.L. nephrometry score, intraoperative findings, blood loss, postoperative course, complications, and follow-up of 6 months duration were recorded. The two groups underwent propensity score matching based on age, body mass index (BMI), and R.E.N.A.L. nephrometry score. 9
Surgical technique
Renorrhaphy group
The patient was placed in a lateral position with ports placed in standard fashion for RAPN. 10 Da Vinci Si robot (Intuitive Surgicals, Sunnyvale, CA, USA) was then docked, and the procedure began with reflecting the colon. Following this, the renal hilum was dissected, isolating the artery and vein, which were secured with vessel loops. Using an intraoperative ultrasound, the tumor was localized. Tumor was dissected all around. Bulldog clamps were applied to the artery and vein. The renal mass was excised completely using blunt and sharp dissection (Fig. 1). If there was a breach in the PCS, it was closed with Stratafix 3-0 (Ethicon, Inc., New Jersey, USA). Spot coagulation of the arterial bleeders was done, and renorrhaphy was performed using a Vicryl 1-0 (Ethicon, Inc.) suture in a single layer by sliding clip technique (Fig. 2). This was followed by releasing the clamps from the renal artery and vein and hemostasis was confirmed.

Images show tumor marking prior to resection followed by tumor bed post resection.
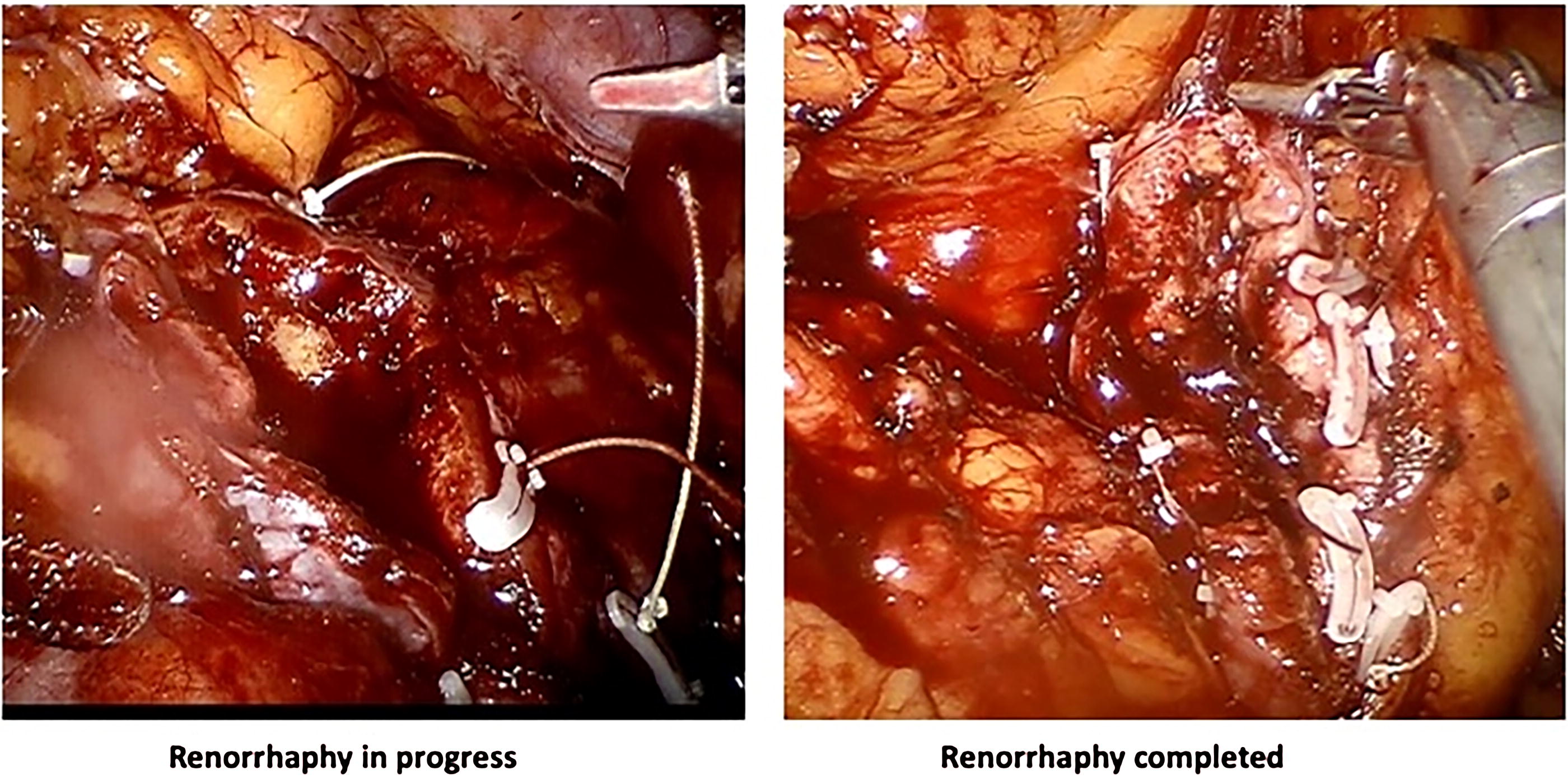
Image depicting renorrhaphy process.
Veriset group
The port placement and surgical technique were similar to the RG. Post application of bulldog clamps on the hilum, the renal mass was excised. Spot coagulation of arterioles was done, larger arteries were clipped, and PCS was sutured with Stratafix 3-0 (Ethicon, Inc.). A single Veriset patch of appropriate size was placed on the tumor bed post excision and compressed with a moist gauze for 30 seconds as per the manufacturer’s recommendation (Fig. 3). Size of the patch used ranged from 2 × 4 cm to 5 × 5 cm depending on the tumor bed size post excision. Hilar clamps were removed, and hemostasis was ensured. Drains were not placed in either group.
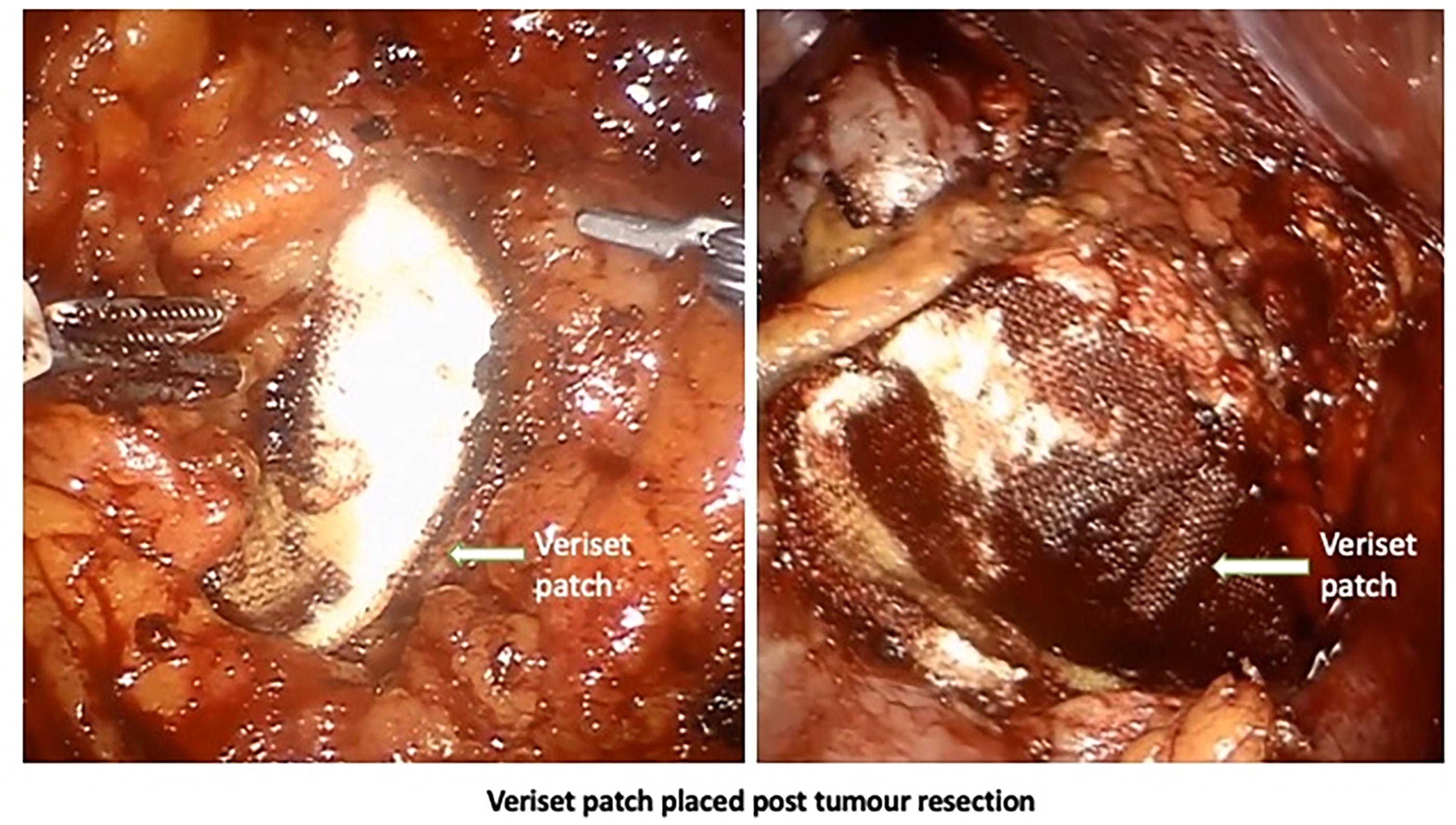
Image demonstrating the application of Veriset patch used for varying tumor sizes.
Statistical analysis
Data was retrospectively retrieved, coded, and recorded using Microsoft Excel. Statistical analysis was performed using R version 4.0.0 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics were presented as means with standard deviations or medians with interquartile ranges for continuous variables and as frequencies and percentages for categorical variables. Propensity score matching was performed to balance baseline characteristics, including age, BMI, and R.E.N.A.L. nephrometry score, between the VG and RG. Matching was conducted using a 1:1 nearest-neighbor approach without replacement to ensure comparability between the groups, yielding 43 patients in each group. Comparisons of continuous variables, such as WIT, console time, and changes in renal function parameters (serum creatinine and eGFR), were conducted using independent sample t-tests. Categorical variables, including postoperative complications, were compared using the chi-squared test or Fisher’s exact test where applicable. Statistical significance was considered at a p value of <0.05.
Results
A total of 120 patients were included in the study, of whom 43 received a Veriset patch. This group was denoted as Veriset group (VG). Seventy-seven patients underwent conventional renorrhaphy group (RG) post tumor resection. The mean age of the study population was 52.62 ± 13.31 years, and the mean nephrometry score was 6.64 ± 1.91. The other features are listed in Table 1.
Patient and Tumor Characteristics of the Two Groups Post Propensity Score Matching
BMI = body mass index; RG = renorrhaphy group; VG = Veriset group.
Propensity score matching yielded 43 patients in the VG and 43 patients in the RG. The two groups were similar with respect to the age, gender distribution, BMI, and nephrometry score of the participants. The WIT (11.95 ± 10.02 minutes vs 17.63 ± 6.59 minutes; p < 0.001) and console time (82.02 ± 25.17 minutes vs 95.53 ± 29.80 minutes; p = 0.014)were observed to be significantly lesser in VG. The use of Veriset patch did not have a significant impact on the margin status of the renal mass post resection. In three (6.97%) patients of VG, Veriset failed to achieve complete hemostasis, necessitating additional cortical renorrhaphy. The RG witnessed a significant reduction in eGFR on postoperative day 1 as opposed to VG (−7.56 ± 15.89 mL/min/1.73 m2 vs −0.21 ± 11.12 mL/min/1.73 m2; p = 0.015). However, following the two groups over 6 months, the difference in eGFR was not significant anymore (−5.88 ± 14.14 vs −5.45 ± 12.49; p = 0.882). One patient from the VG had significant bleeding on postoperative day 1, which required angioembolization to be performed by interventional radiologist. Four patients of the RG and two patients of VG had postoperative hematuria, which settled with conservative management.
Discussion
With the widespread availability of technology, RAPN has emerged as a popular surgical treatment option for small renal mass. 11 Along with the advantages of minimally invasive operation, this surgical technique has been successful in achieving the “trifecta” goals of negative surgical margins, maximum preservation of functional renal parenchyma, and minimal surgical complications. 12 As per the literature, the main factors believed to contribute to the loss of renal function are the volume of viable renal parenchyma excised, the duration of ischemia, and the damage caused by renorrhaphy. 13–14 Simmons et al. state that renorrhaphy causes tissue damage because of the ligation of segmental arteries and strangulation of the parenchyma. 15 In order to overcome these shortcomings, our surgical practice initially evolved from performing renorrhaphy in two layers to single-layer outer cortical renorrhaphy and thereby reduced WITs and symptomatic pseudoaneurysm rates. 16 Limiting WIT to less than 30 minutes limits the renal function damage and thereby prevents long-term renal dysfunction. 17
Several alternatives to preserve vascularized renal parenchyma have been proposed by various authors like selective clamping, off clamp renorrhaphy, use of sealant agents such as BioGlue, and use of TachoSil containing human thrombin and fibrin glue. 18,19 These alternatives had drawbacks of excessive bleeding or were reserved for tumors of small size. There are isolated case reports of fibrin glue causing ureteral obstruction because of periureteral adhesions and inflammation, thus precluding its use. 20
In our study, we assessed if Veriset hemostatic patch can be used as an effective alternative to renorrhaphy in RAPN. Veriset gets activated on contact with blood or body fluid and acts as a mechanical hemostatic agent by concentrating and activating platelets and clotting factors to promote hemostasis. 21 It gets completely absorbed over 28 days. It can be easily introduced into the operative field through one of the surgical ports without prolonging the operative duration. Although suturing of the renal parenchyma is a time-consuming process, the use of Veriset hemostatic patch avoids this and is hence faster. This logically results in shorter warm ischemia and operative times. We observed similar findings in our study, where the VG had significantly shorter WIT and console time than the RG. This reflected in the serum creatinine and eGFR on postoperative day 1. However, after 6 months of follow-up, the change in serum creatinine levels and eGFR did not vary significantly among the two approaches. This could be attributed to the fact that care was taken to maintain the mean WIT of less than 25 minutes, irrespective of the approach used. The intraoperative blood loss, need for blood transfusion, and postoperative change in hemoglobin rates in the VG were comparable to the RG. Three patients had failed Veriset patch application which was identified intraoperatively and renorrhaphy was performed for damage control. One patient with a nephrometry score of 8p, in the VG had significant bleeding in the immediate postoperative period. CT angiogram showed the presence of active arterial bleeder in one of the renal artery branches and angioembolization was performed with gelfoam particles for hemostasis. In this particular case, brisk bleeding occurred after clamp release; however, sustained pressure on the patch eventually controlled the bleeding. We believe this was a case of poor selection, which warranted additional cortical renorrhaphy. The key takeaway from these instances is that if hemostasis is not optimal, performing renorrhaphy would be the preferred approach. Since the activation of the patch requires an intact coagulation cascade, it should be avoided in patients with known bleeding disorders or coagulopathy. We have not excluded patients with comorbidities such as hypertension, renal insufficiency, or diabetes. On the contrary, we believe that minimizing parenchymal damage and reducing warm ischemia time may be beneficial for patients with chronic kidney disease. It is to be noted that no patient in either group suffered from urine leak. This reinforces the relevance of identifying and repairing breach in the PCS appropriately before placing hemostatic patch or performing renorrhaphy. Four patients in the RG group and two patients in the VG group had mild hematuria, which was self-limiting and did not require any treatment. It was feasible to use the Veriset patch for tumors across all ranges of nephrometry scores. The mean tumor size for patients in the VG was 3.00 ± 1.19 cm. However, the range of tumor size treated in the VG varied from the smallest of 1 cm to the largest tumor of 6 cm dimension. The surgical margin positivity rates were similar in both groups. The use of the Veriset patch may slightly increase the cost of surgical consumables, but this would be nullified by eliminating the need for sutures and Hem-o-Lok® clips. This technique is likely to be particularly beneficial for patients with a solitary kidney, multiple tumors, or borderline renal function, where minimizing WIT is of paramount importance.
Limitations
Our study was not a randomized study. Three of our patients had failed Veriset patch application. Bleeding did not settle with patch placement, and reinforcement with cortical renorrhaphy was needed in these patients. We observed that failures in our cases were primarily caused by brisk arterial bleeding from the base of the defect. Another contributing factor was inadequate patch coverage over the bed or a poor fit. We also did not prefer to place the Veriset patch in cases where there was a major breach of the PCS. This may have introduced a selection bias, but it was mitigated through propensity matching.
Conclusion
VG has less WIT, decreased console time, and early return of renal function with no increased rate of complications. The VG was equivalent to the RG in achieving the trifecta outcome after RAPN. It is feasible to use the patch without drastically increasing the operative charges and operative duration.
Footnotes
Acknowledgment
The authors thank Dhanya Jose for data compilation.
Authors’ Contributions
J.E.M.: Data analysis, article writing, and editing. A.K.P.: Data collection and article editing. T.A.K.: Project development, article writing, and editing.
Author Disclosure Statement
There are no conflicts of interest to declare.
Funding Information
There are no funders to report for this submission.