
Abstract
Introduction:
Ureteral stone impaction can significantly affect the success of ureteroscopy (URS) in children. While the factors predicting impaction have been well studied in adults, data in children are limited. This study aimed to identify factors that predict ureteral stone impaction in children undergoing URS and to compare the success rates and complications based on the stone impaction status.
Patients and Methods:
Pediatric patients undergoing URS for ureteral stones were retrospectively reviewed. Impaction status of the stones was evaluated by radiological parameters and the children were divided into two groups based on the presence of stone impaction. Peri- and postoperative findings were comparatively evaluated in patients with or without stone impaction.
Results:
A total of 102 pediatric patients were included (40 with impacted stones, 62 with nonimpacted ureteral stones). The mean age was 9.3 ± 5.3 years. Univariate analysis showed significant differences between the groups in degree of hydronephrosis, presenting symptoms, stone density (HU), stone size, upper ureteral diameter, and that of ureteral wall thickness (UWT) (p = 0.004, p = 0.044, p = 0.033, p = 0.005, p = 0.012, p = 0.000, respectively). Multivariate analysis revealed UWT as the only independent predictor of stone impaction, with a cutoff value of 2.63 mm showing 83% sensitivity and 82% specificity (p = 0.000). The highest UWT value in the nonimpacted stone group was 3.1 mm. The mean operation time was found to be significantly longer in cases with impacted stones (p = 0.000). Kids with impacted stones had lower mean success rate (impacted = 70%, nonimpacted = 88.7%) and higher mean rate of complications, longer duration of DJ-stenting, more anesthesia sessions (p = 0.018, p = 0.019, p = 0.000 and p = 0.000, respectively).
Conclusions:
Similar to the adult cases, UWT could be used as a reliable parameter in predicting the impaction status of ureteral stones in pediatric patients. Impacted ureteral stones may reveal decreased success and higher complications rates during and after endoscopic stone surgery in these cases.
Introduction
According to the EAU 2024 Pediatric Urology Guidelines, ureteroscopy (URS) is the first treatment option for distal ureteral stones, and as a highly successful modality, it is also recommended for pediatric proximal ureteral stones when extracorporeal shockwave lithotripsy seems to be unsuccessful. 1 Although endoscopic management (URS)-related complication rates are generally low and often self-limiting, similar to the adults cases, severe complications may be encountered particularly in unexperienced hands. 2
Such complications are also highly likely to occur in cases presenting with large and particularly impacted ureteral stones. 3 Impaction (embedment) of ureteral stones into the ureteral wall is one of the most important factors which could compromise the URS procedure with certain problems either during or after these endoscopic procedures. 4
Regarding the possible detrimental effects of stone impaction on the course and outcomes of the endoscopic stone removal procedures, ongoing research is focused on identifying certain predictive parameters which may give valuable information on the presence and degree of impaction in an attempt to predict the failure and complications to mitigate these risks. 5,6
Studies indicated that an inflammatory reaction develops in the mucosa of the surrounding ureteral portion as a result of the irritating reactions induced by these calculi. 7 –9 Therefore, varying degrees of mucosal edema and polyp formation could be encountered, and these formations growing into the intraluminal space distal to impacted ureteral stones may cause certain problems during the access and treatment of the stones. 10 These problems may be noted as difficulties in safety guidewire placement (in the first attempt), in accessing the ureteral stone and lastly possible hemorrhage during lithotripsy. 11 Taking all these facts into account, it is clear that the success of URS in impacted ureteral stones may be lower compared with the uncomplicated stones with increased risk of complications. 12,13
Unlike the data evaluated and published in adults so far, there are insufficient data on the factors which may help us to predict the degree of ureteral stone impaction observed during URS in pediatric patients and the possible impact of these factors on the success/complications associated with these procedures. To our knowledge, this is the first study focusing on the importance of stone impaction and the relevant predictive factors on its assessment which may enable us to predict the course of applied endoscopic procedure.
In this study, we aimed to evaluate radiological factors that could predict ureteral stone impaction in pediatric patients and the possible impact of impaction on the peri- and postoperative parameters (including success and complication rates) in pediatric patients undergoing URS.
Patients and Methods
The protocol of this retrospective study was approved by the KTO Karatay University Faculty of Medicine Ethics Committee (Approval Date and Number: 2024/027). Clinical data of pediatric patients under 18 years of age undergoing URS for ureteral stones were retrospectively reviewed. Children were divided into two groups based on the presence of stone impaction during endoscopic treatment. Patients without preoperative noncontrast enhanced computed tomography (NCCT), those who underwent simultaneous endoscopic renal surgery, or contralateral URS, and those with insufficient postoperative data were excluded.
Preoperative radiological evaluation was done by using low-dose NCCT. These images were retrospectively assessed by an experienced radiologist, unaware of the surgical outcomes. The stone location was classified as the upper ureter if it was between the ureteropelvic junction and the iliac crest and as the lower ureter if it was located between the iliac crest and uretero-vesical junction (UVJ). Ureteral diameter was measured at the segment just proximal of the stone site. Ureteral wall thickness (UWT) was calculated by measuring the longest wall thickness at the location of stone in transverse axis images under magnification 14 (Fig. 1). Ureteral stone fixation of mucosa (embedment into the ureteral wall) was defined as impaction during the endoscopic ureteral stone disintegration and removal.
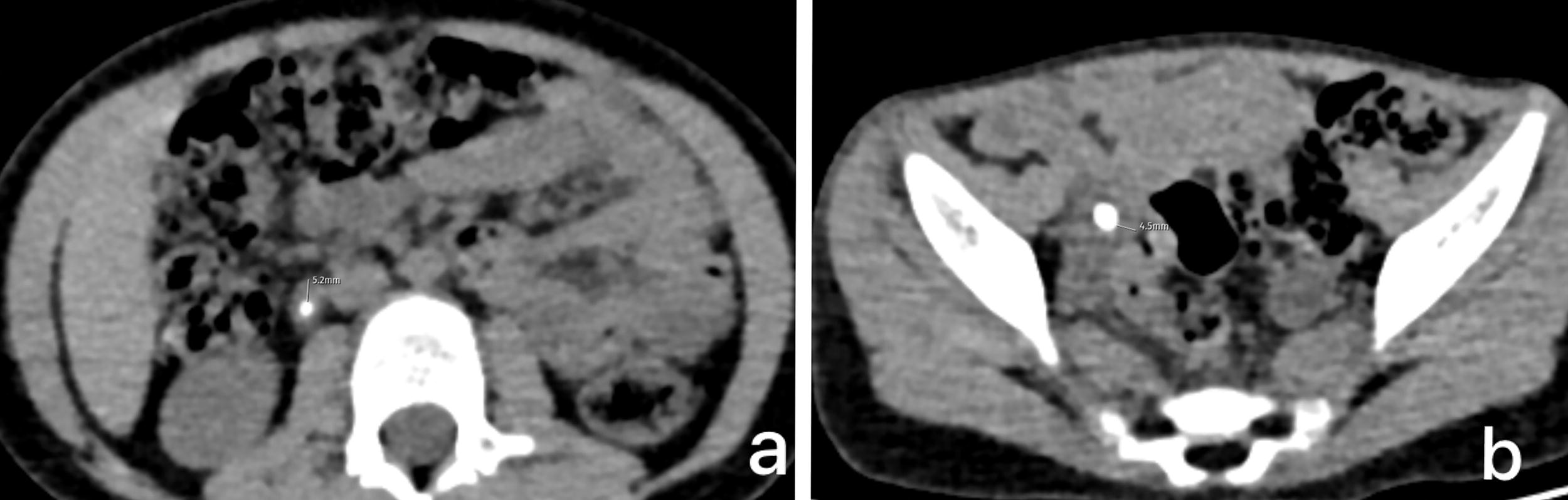
Examples of increased ureteral wall thickness in pediatric patients:
Surgical procedure
URS was performed with sterile urine culture outcomes and all children received antibiotic prophylaxis. All procedures were performed by the same surgical team. Following cystoscopy, a 0.025/0.035 inches safety guidewire was inserted into the involved ureter with a 4.5/6.5 Fr semirigid ureterorenoscope. If the safety guidewire could not be inserted, the stone was first reached with a working guidewire and fragmented (with the holmium:YAG laser) just enough to allow the safety guidewire to pass. Following the placement of safety guidewire, fragmentation was continued/completed. If the stone could not be reached with the ureteroscope, the procedure was further performed by advancing a 7.5 Fr disposable flexible ureteroscope over the guidewire. If the flexible ureteroscope could not be passed, the procedure was terminated by placing a ureteral DJ-stent was chosen in accordance with the patient’s age. 15 When fragmentation was completed, a standard or stringed DJ-stent was placed according to the appearance of ureter and presence of residual fragments.
Stringed DJ-stent was removed within 2–7 days. The standard DJ-stent was removed under anesthesia after 3–4 weeks. A second-look URS was performed if necessary.
Stone-free status was evaluated with X-ray and urinary ultrasound on the postoperative 1st month. Success was defined as no fragment in the ureter or fragments sized <2 mm pushed-back to the kidney during the procedure. Modified Clavien–Dindo classification was used for postoperative complications.
Statistical evaluation
All data was analyzed using the SPSS v.25.0. The data distribution was tested with the Kolmogorov–Smirnov. Numerical variables were compared between the two groups with the independent-samples t test. Categorical variables were compared with the chi-square test. A multivariate (logistic regression) analysis was used to determine independent predictors. A p value of <0.05 was considered statistically significant.
Results
A total of 102 pediatric patients with ureteral calculi (n = 40 impacted, n = 62 nonimpacted) undergoing URS were included in the study. Mean age was 9.3 ± 5.3 years and the male to female ratio was 1.08 (53/49). Preoperative data showed no significant differences in gender, age, stone laterality, previous interventions, and stone location (p = 0.368, p = 0.412, p = 0.672, p = 0.175, and p = 0.125, respectively). Similarly, no significant differences were found between the two groups in blood serum analysis parameters. Univariate analysis of radiological data revealed significant differences between the two groups in the degree of hydronephrosis, presenting symptoms, stone density (HU), stone size, upper ureteral diameter, and UWT (p = 0.004, p = 0.044, p = 0.033, p = 0.005, p = 0.012, p = 0.000, respectively).
However, multivariate analysis revealed UWT as the only significant predictor of stone impaction (p = 0.000, 95% confidence interval OR = 24.291). Comparative preoperative data including both univariate and multivariate analyses are shown in Table 1.
Comparison of Impacted and Nonimpacted Ureteral Stones: Univariate and Multivariate Analysis of Preoperative Data
Mean ± std deviation.
95% confidence interval OR = 24.291.
ROC analysis has shown a cutoff value of 2.63 mm for UWT was identified to be predictor enough for stone impaction (sensitivity 83%, specificity 82%)(Fig. 2). A more detailed analysis revealed well that the highest UWT value in nonimpacted stone group was measured at 3.1 mm (Fig. 3).
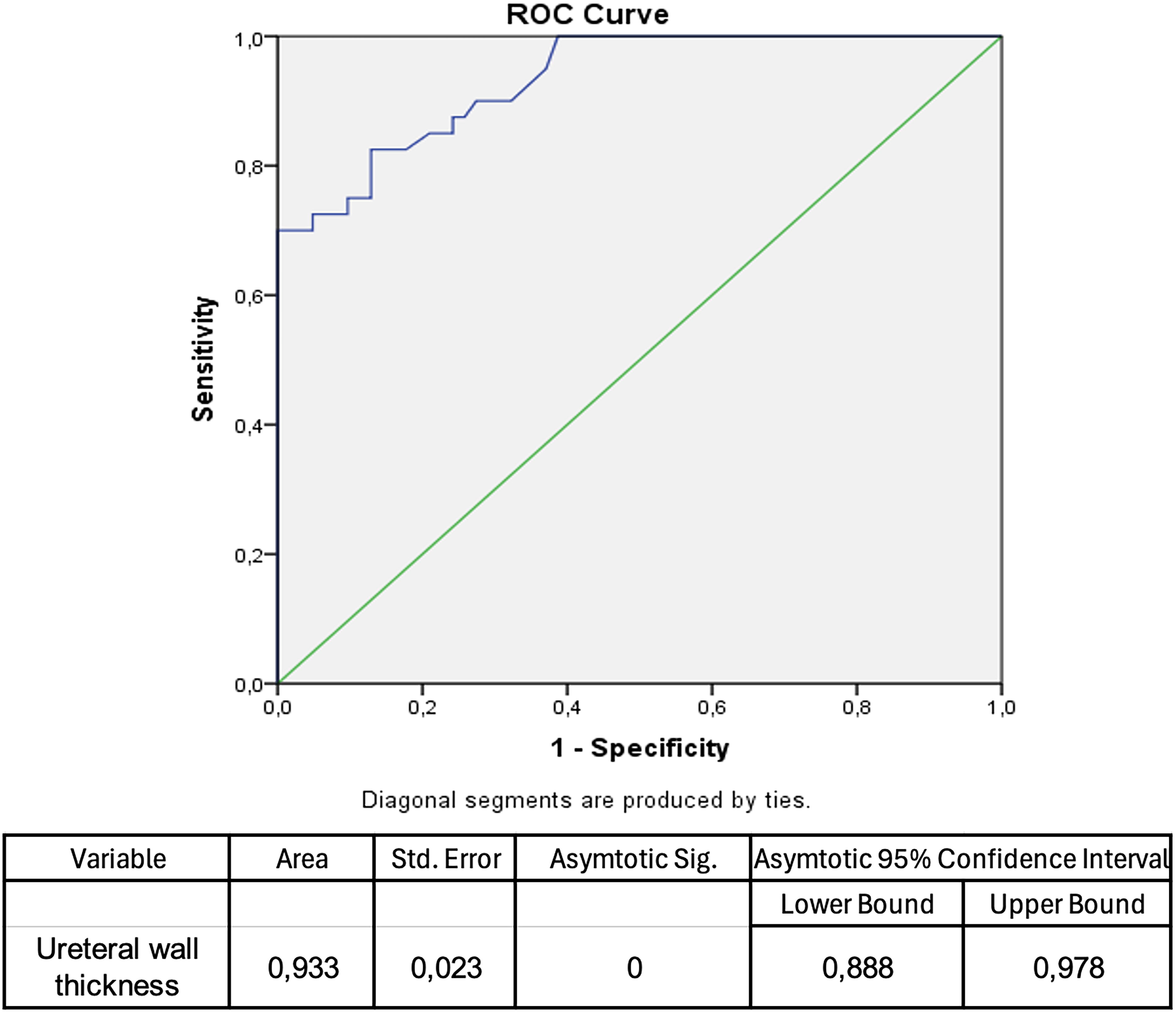
ROC curve of ureteral wall thickness.
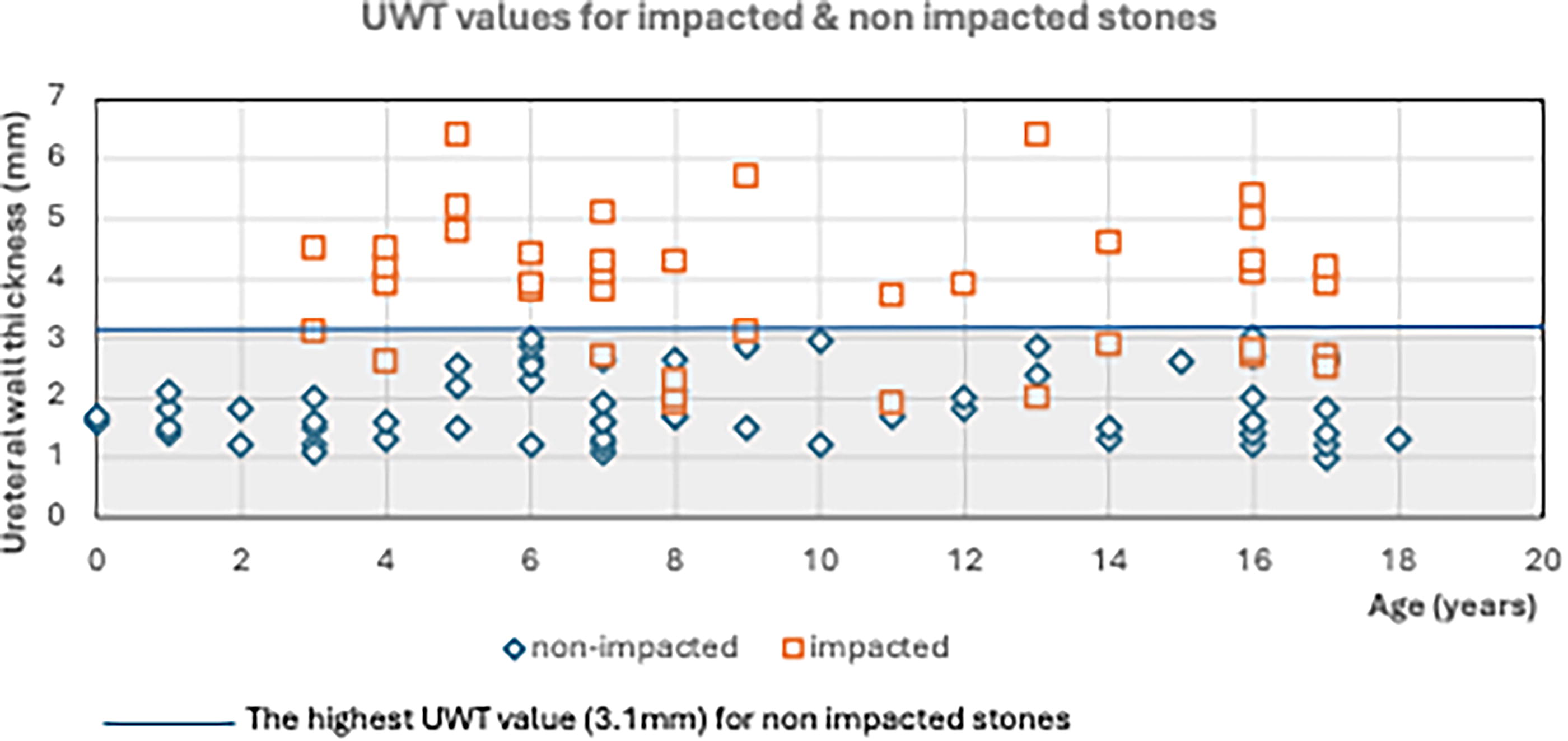
UWT values for impacted and nonimpacted ureteral stones. UWT, ureteral wall thickness.
Although the mean operation time was found to be significantly longer in the impacted group, mean length of hospital stay was similar between the two groups (p = 0.000, p = 0.258, respectively). Mean follow-up period was 21 months and was comparable between the groups.
Lastly operative outcomes in both groups revealed that, in addition to the significantly lower success rates, duration of DJ-stenting, and number of anesthesia sessions and complications were significantly higher in children treated for impacted stones (p = 0.018, p = 0.000, p = 0.000, and p = 0.019, respectively). A detailed perioperative and postoperative findings based on the presence/absence of impaction is shown in Table 2.
Evaluation of Peroperative and Postoperative Data Based on Ureteral Stone Impactation
Mean ± std deviation.
A total of 9 kids (22.5%) in the impacted group and 3 kids (4.8%) in the nonimpacted group developed complications, revealing an overall complication rate of 11.8% (n = 12). There were two major complications which were noted in children with impacted stones. One patient, undergoing URS for an impacted proximal ureteral stone required repeated stent placements (twice). Due to stricture formation, which manifested as worsening hydronephrosis and poor drainage observed on dynamic scintigraphy, laparoscopic uretero-ureterostomy was performed in this case. In another case developing fever during early postoperative period, where the X-ray revealed migration of the DJ-stent, re-stenting was performed.
Minor complications occurred in 7 patients with impacted stones and in 3 patients with nonimpacted stones. In the impacted group, 1 patient developed fever in the early postoperative period. While the mean number of hospital re-admissions was 7 (17.5%) in children referring with impacted stones, this number was noted to be 2 (3.2%) in the kids with nonimpacted stones, with significant difference (p = 0.013). Following discharge, 2 patients in the impacted stone group experienced severe pain, 2 had delayed hematuria, and 2 presented with fever and recurrent emergency visits. All patients were managed with appropriate medical treatment and followed up uneventfully. In the nonimpacted group, however, only 1 patient experienced severe pain after discharge and another developed incontinence due to migration of the DJ-stent into the urethra. The DJ-stent was removed and patient had an uneventful postoperative course.
Discussion
With a significantly increasing incidence particularly in some developing countries (where the disease is endemic), pediatric urolithiasis remains as a serious healthcare concern due to the high recurrence rates. 16 Of all the stones diagnosed in this population ureteral ones account for ∼20%, requiring an active treatment in a certain percent of these cases. 17 Pediatric URS began following the use of an 8.5 Fr rigid ureteroscope for the treatment of a distal ureter stone in a four-year-old child in 1988. 18 Since this initial report, as a result of the marked advancements in the endoscopic equipments and evolving management techniques, a significant progress has been noted in the minimal invasive treatment of pediatric ureteral stones. After obtaining an adequate level of experience, authors began to focus on the prediction success as well as complications rates of this particular procedure in this specific population.
The ultimate success of URS is influenced by factors such as stone size and location, with larger and proximally located stones being associated with higher failure rates. 19 Evaluation of the published data on this aspect demonstrates that the rates of complications following URS in the pediatric population range from 0% to 24%. 20 These rates are even higher in younger patients as reported in one systematic review with a complication rate of as much as 24% in preschool children. 21
On the other hand, management of impacted ureteral stones pose a further significant challenge to the urologists due to certain factors evaluated in a number of studies performed in adults. The persistent irritation caused by the impacted stone can lead to the formation of ureteral epithelial hypertrophy and edema, which may further limit the change of spontaneous stone passage. 22 Accumulating evidence demonstrates well that as a stone becomes more embedded in the ureteral wall, in addition to the less likelihood of spontaneous passage, this situation has been found to affect the success rates of stone removal procedures in a negative manner. 23 Moreover, URS procedure may become more difficult to perform in such cases due to the impaired visualization and the need for the fine/careful separation of the stone from the ureteral mucosa. 22 In addition, the risk of intraoperative complications seems to be higher in impacted stones among which ureteral perforation is the most crucial one which potentially lead to adverse surgical outcomes and postoperative severe problems. 12 In an attempt to predict the impaction status of the stone(s) along with the possible endoscopic findings at the stone site, UWT measurement on CT images at the impacted site has been shown to be helpful in the prediction of both the success and complication rates following endoscopic management of such stones in adult patients. 24 In some pediatric patients, the low-dose NCCT protocol makes it difficult to define the limits of the ureteral wall. This limitation may be overcome by using Hounsfield units, which can help identify the ureteral wall limits (especially fat vs soft tissue). 14 Although CT urography could offer a more objective evaluation, its use is avoided specifically in pediatric patients with stones due to the potential risks associated with radiation exposure.
To date, only two studies have specifically addressed the value of UWT measurement in pediatric patients with ureteral stones. Tuerxun et al. reported that a thicker ureteral wall was a strong predictor of medical expulsive therapy failure, suggesting that stone removal should be considered in children with a thickened ureteral wall at the stone site. 25 Similarly, Kirli et al. found that UWT could serve as a predictive factor for both URS outcomes and complications in children. 26 Our findings indicated well that stone impaction is associated with lower success rates, higher complication rates, increased likelihood of hospital readmission, longer duration of stent placement, and a greater number of anesthesia sessions in these cases. Notably, the findings of our study are of importance, as it is the first one to demonstrate the importance of UWT measurement in the prediction of such outcomes in the pediatric population. Multivariate analysis of our findings identified UWT as the only significant predictor on this aspect. If the presence of ureteral stone impaction can be accurately predicted, families of these pediatric patients can be better informed about potential outcomes and management strategies.
Given the higher risk of complications and lower success rates associated with impaction, cutoff values have been proposed for consideration in adult populations, and various nomograms have been suggested. Kirli et al. stated that a UWT value of greater than 4.5 mm could be associated with increased risk of complications and treatment failure in pediatrics. 26 In our pediatric cohort, the cutoff value for the prediction of impaction was found to be 2.63 mm, with a maximum value of 3.1 mm. In other words, if the UWT value assessed on NCCT images exceeds 3.1 mm in pediatric patients, impaction of the ureteral stone seems to be highly likely.
Kirli et al. further reported that UWT was associated with an elevated white blood cell count and a higher proportion of neutrophils. Their rationale was that serum levels of inflammatory markers increase in direct proportion to the severity of tissue inflammation, as the interaction between the stone surface and the ureteral wall may induce inflammatory responses over time. 26 However, in our cohort, we did not observe such correlations with no significant differences in the hematological parameters between the cases with impacted and nonimpacted calculi. In our view, if there is no widespread inflammation or active infection, the inflammation within the ureter appears to be localized and may not reach a critical level to impact systemic blood levels. Furthermore, hematological parameters can vary considerably across different pediatric age groups. Given the wide age range in our cohort, these variations may limit the generalizability of our findings in this context.
Common postoperative complications following URS include renal colic, fever, hematuria, and urinary tract infections. The most consistently reported long-term complication is UVJ stricture, which typically requires reimplantation and occurs in <1% of patients. 27 In our cohort, majority of the complications were minor in nature, and they all were managed with proper medical treatment on time. Although no serious complications such as UVJ stricture were observed, one case with an impacted proximal ureteral stone required a uretero-ureterostomy due to stricture formation.
Our current study is not free of limitations. First of all the retrospective design of the study protocol may constitute a main limitation. As a second limitation, defining the limits of UWT measurement is difficult in some studies. As mentioned earlier, Hounsfield unit measurements under magnification could be helpful in this regard. In addition, the small size of our cohort did not allow us to evaluate proximal and distal ureter stones separately on this aspect. However, taking the highly limited number of publications available in the literature and the limited number of centers where pediatric endoscopic surgery is performed, we believe the preliminary findings of this study carry considerable significance in an attempt to contribute to the existing information in the literature.
Conclusions
Our findings indicated well that the presence of impaction in ureteral stones could decrease the success rates and increase the complications during or after endoscopic stone procedures in kids. Assessment of UWT may help well as an independent parameter in the prediction of the impaction status of pediatric ureteral stones which may be highly helpful for a rational management plan in these particular cases.
Footnotes
Acknowledgment
The authors would like to thank Nadir Sezer (M.D.), the radiologist who performed the measurements by reviewing the preoperative CT images.
Authors’ Contributions
All the authors contributed to the study conception and design. Material preparation and data collection were performed by A.S. and B.T. Formal analysis was made by E.B. and H.Y. The first draft of the article was written by A.S., E.B., and B.T., and all the authors commented on previous versions of the article. A.S., B.T., and K.S. wrote the final draft, and all the authors read and approved the final article. Supervision and critical review were made by K.S.
Author Disclosure Statement
The authors declare that they have no conflict of interest.
Funding Information
No funding was received for this article.