
Abstract
Introduction:
We evaluate radiographical changes involved with the implementation of ureteral rest before robotic ureteral reconstruction (RUR) for the management of ureteral strictures.
Materials and Methods:
We retrospectively reviewed our single-institutional robotic ureteral surgery database to identify all consecutive patients who underwent ureteral rest before RUR for the surgical management of ureteral strictures between 1/2018 and 12/2022. Ureteral rest was defined as having the absence of hardware across a strictured segment before definitive surgical repair. All patients who obtained both pre- and post-ureteral rest retrograde and/or antegrade pyelograms were included for analysis. An experienced genitourinary radiologist reviewed all pre- and post-retrograde and/or antegrade pyelograms to determine stricture quality and length. Primary outcomes included the change in stricture quality and the difference in ureteral stricture length after ureteral rest.
Results:
Overall, 50 patients met the inclusion criteria. Preoperative stricture quality was determined to be narrowed in 86.0% and obliterative in 14.0% of patients. The median duration of ureteral rest was 11.1 (interquartile range [IQR] 5.7–22.8) weeks. Of those with narrowed strictures, 12.0% progressed to obliterative strictures after ureteral rest. There were 37 (74.0%) patients who had an increase in stricture length after ureteral rest. The median growth in stricture length after ureteral rest was 0.2 (IQR: −0.2–0.4) centimeters. At a median follow-up of 6.2 (IQR: 2.9–10.0) months, 88.0% of patients were surgically successful.
Conclusions:
Ureteral rest can lead to changes in stricture quality, which may be valuable in surgical decision-making.
Introduction and Objectives
The role of urethral rest and its benefits before surgical management of urethral stricture disease have been well-established. 1,2 The concept of ureteral rest is an emerging paradigm in the management of ureteral strictures prior to robotic ureteral reconstruction (RUR). Ureteral rest draws parallels to urethral rest, as it involves the absence of hardware across a ureteral stricture for a duration of time before definitive surgical management. Despite its potential benefits, the application of ureteral rest in clinical practice remains varied, with a lack of standardized protocols and guidelines. To provide further objective evidence regarding the implementation of ureteral rest, we evaluate the radiographical changes involved with ureteral rest before RUR for ureteral stricture management.
Materials and Methods
We retrospectively reviewed our single institutional robotic ureteral surgery database for all consecutive patients who underwent ureteral rest prior to RUR for the management of ureteropelvic junction obstruction or proximal, middle, or distal ureteral strictures between 2018 and 2022. The present study protocol was reviewed and approved by the Institutional Review Board of Temple University (Protocol Number: 20793). All patients underwent ureteral rest prior to their RUR procedure. Adult patients with a retrograde pyelogram before ureteral rest and either a retrograde and/or antegrade pyelogram after ureteral rest were included for analysis. All patients included in this study had indwelling hardware across their stricture (Double-J ureteral stent or percutaneous nephroureteral tube) on the day of their pre-ureteral rest imaging. Ureteral rest was defined as the absence of hardware, such as a Double-J ureteral stent or percutaneous nephroureterostomy tube, across the strictured aspect of the ureter for a minimum duration of 4 weeks.
An expert genitourinary radiologist reviewed all retrograde and antegrade pyelograms to determine ureteral stricture length and quality (narrowed vs obliterative). To standardize each fluoroscopic study, each image was calibrated based on the diameter of the 5 Fr regular ureteral catheter seen on each radiograph. Once each image was calibrated appropriately, an accurate ureteral stricture length was measured and compared to other images in this cohort. We did not utilize ureteroscopy to characterize stricture quality in this cohort.
The primary outcomes of this study included the change in stricture quality and the difference in ureteral stricture length after a period of ureteral rest. A descriptive analysis was performed to demonstrate these outcomes.
Results
Our cohort consisted of 50 patients who met the inclusion criteria (Table 1). Ureteral strictures were located in the ureteropelvic junction, proximal, middle, and distal ureter in 9 (18.0%), 18 (36.0%), 9 (18.0%), and 14 (28.0%) patients, respectively. Etiologies of stricture formation included radiation (12.0%), idiopathic (52.0%) and iatrogenic secondary to prior endoscopic procedures (36.0%). With regard to preoperative stricture quality, 43 (86.0%) patients had narrowed strictures and 7 (14.0%) patients had obliterative strictures. There were 26 (52.0%) patients who had prior failed endoscopic and/or surgical interventions for ureteral stricture management. The median duration of ureteral rest was 11.1 (interquartile range [IQR] 5.7–22.8) weeks. Twenty-eight (56.0%) patients elected to have a percutaneous nephrostomy tube placed for ureteral rest.
Descriptive Analysis of Variables Pre- and Post-Ureteral Rest
IQR = interquartile range.
There were 6 (12.0%) patients who had a change in stricture quality from a narrowed to an obliterative stricture after ureteral rest (Fig. 1). There were 37 (74.0%) patients with an increase in stricture length after ureteral rest (Fig. 2). The median difference in radiographical stricture length after a period of ureteral rest was 0.2 (IQR: −0.2–0.4) centimeters (Fig. 3). The RUR procedures performed included pyeloplasty (10.0%), ureteroureterostomy (8.0%), buccal mucosa graft ureteroplasty (54.0%), and reimplantation (28.0%). At a median follow-up of 6.2 (IQR: 2.9–10.0) months, 44 (88.0%) patients had surgical success, defined as the lack of any need for additional surgical intervention.
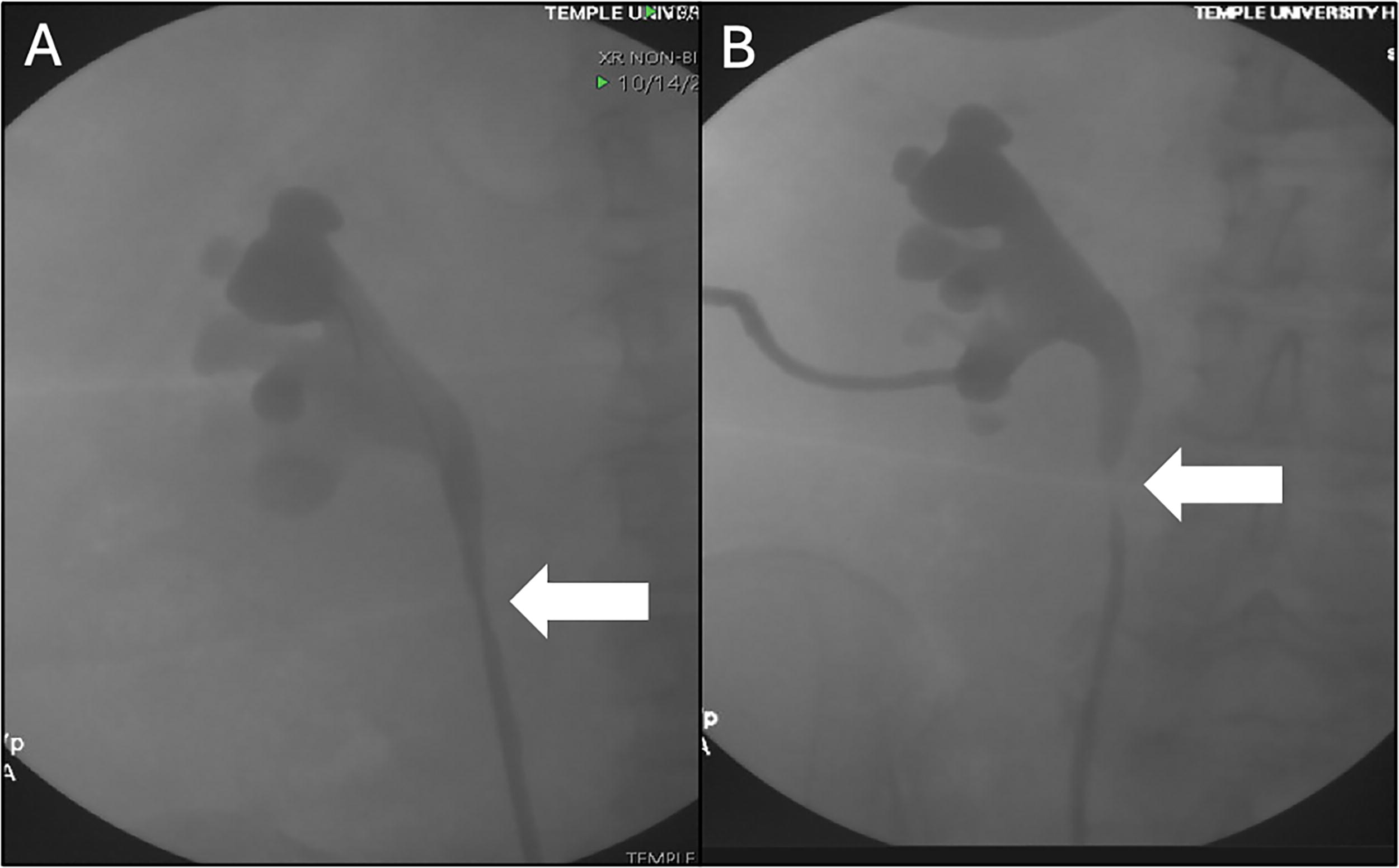
This figure demonstrates a pre-ureteral rest retrograde pyelogram

This figure demonstrates a pre-ureteral rest retrograde pyelogram
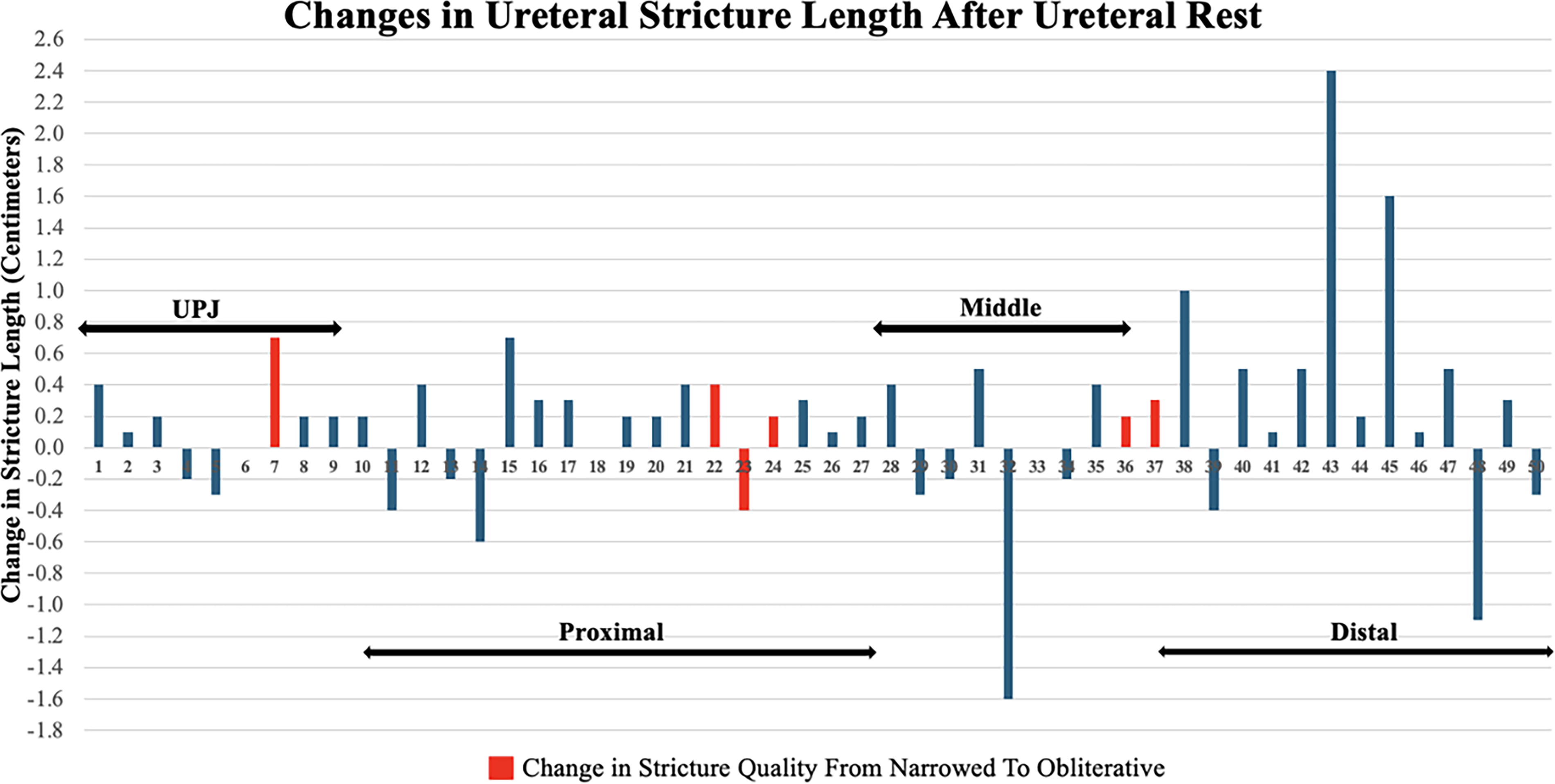
This graph depicts the change in ureteral stricture length after ureteral rest for each patient in our cohort. A negative change indicates a decrease in length following ureteral rest, whereas a positive change reflects an increase in stricture length after the rest period. The red bars highlight the cases in which there was a change in stricture quality from narrowed to obliterative after ureteral rest.
Discussion
Implementation of ureteral rest prior to RUR may facilitate ureteral stricture maturation and stabilization. 3 This is similar to the concept of urethral rest, which encourages tissue recovery and initiates tissue remodeling. Terlecki et al. demonstrated that urethral rest may allow for stricture contraction to determine the true extent and severity of a urethral stricture, which facilitates proper selection for reconstructive repair. 1 In their study, the authors showed that a period of urethral rest promoted the identification of obliterative stricture segments, which warranted the implementation of transecting urethroplasty techniques rather than non-transecting onlay techniques. 1 Furthermore, Da Silva et al. evaluated the histological changes associated with urethral rest by staining histological sections of the proximal and distal healthy urethral ends during an end-to-end anastomotic urethroplasty. 3 The authors noted that urethral tissue without a suprapubic cystostomy tube preoperatively demonstrated more robust fibroblast and inflammatory cells, including an increased ratio of collagen type III:I as compared to urethral tissue with a suprapubic cystostomy tube. 3
The benefits of accurate preoperative characterization of stricture length have been demonstrated in the urethral literature. In a multi-institutional study from the Trauma and Urologic Reconstruction Network of Surgeons, authors analyzed 20 radiographs of patients with anterior urethral strictures before and after a period of urethral rest with a suprapubic cystostomy tube. 2 The mean radiographical stricture length post-suprapubic cystostomy tube placement vs intraoperative stricture length was 3.0 (standard deviation [SD] 2.6) vs 3.8 (SD: 3.3) centimeters, respectively (p < 0.0001). Furthermore, there was a higher incidence of urethral obliteration on imaging after urethral rest (23% vs 58%, p < 0.0005). The group suggested that this finding in stricture quality after urethral rest drove changes in the proposed surgical plan from an augmentation to an excision procedure in 7% of patients. 2
There is limited evidence evaluating the role of ureteral rest before definitive reconstruction surgery. In a multi-institutional retrospective analysis, Lee et al. compared outcomes in 194 (92.9%) patients who underwent ureteral rest before RUR vs 40 (17.1%) patients who did not. 4 The patients who underwent ureteral rest were associated with a higher success rate compared to those not undergoing ureteral rest (90.7% vs 77.5%, respectively; p = 0.027). In their series, the ureteral rest group was associated with lower estimated blood loss (50 vs 75 milliliters, respectively; p < 0.001) and lower likelihood of undergoing a buccal mucosa graft ureteroplasty (20.1% vs 37.5%, respectively; p = 0.023). The reasoning for the latter association was hypothesized to be due to the inability to identify exact stricture margins in those not undergoing ureteral rest, encouraging the utilization of a repair that could treat longer strictures rather than a primary anastomosis. 4
To our knowledge, our study is the first to analyze radiographical changes of strictures before and after ureteral rest. We demonstrated that after a median duration of 11.1 (IQR: 5.7–22.8) weeks of ureteral rest, there was a radiographical change in stricture quality from narrowed to obliterative in 12.0% of all cases. When stratifying among those patients who had narrowed strictures preoperatively, the change in stricture quality from narrowed to obliterative was observed in 14.0% of cases. As such, in these six cases, a transecting (dismembered pyeloplasty, refluxing reimplantation, or an augmented anastomotic buccal mucosa graft ureteroplasty) rather than a non-transecting ureteroplasty was performed. Our preference is to perform non-transecting ureteroplasty in cases of narrowed strictures, where the lumen remains preserved. As more non-transecting techniques are being performed, 5 –7 especially during redo cases where preservation of ureteral vasculature is critical, an accurate diagnosis of the quality of the stricture (narrowed vs obliterative) is necessary. In the absence of ureteral rest, it may not be evident that a stricture is truly obliterative, and performing a non-transecting technique in that setting may risk inadequate reconstruction and potential surgical failure. Furthermore, similar to data in the urethral literature, 2 our study demonstrated that ureteral rest was associated with a minimal degree of stricture lengthening (median difference of 0.2 centimeters, IQR: −0.2–0.4). Overall, there was a high frequency (74.0%) of stricture lengthening observed after ureteral rest. It is difficult to conclude that the modest increase in stricture length after ureteral rest made an impact on surgical decision-making. However, the overall radiographical changes (i.e., change in stricture quality, high frequency of stricture lengthening) associated with ureteral rest may be valuable in surgical planning. We believe ureteral rest may facilitate stricture maturation, which may lead to better operative decision-making and surgical outcomes. 8
Our study is limited by its small sample size, single radiologist evaluation, and retrospective design. There is a degree of selection bias, as our analysis is limited to those patients who had both a satisfactory pre- and post-ureteral rest retrograde and/or antegrade pyelogram. Also, patients had different caliber ureteral stent sizes prior to ureteral rest, which may add bias. Furthermore, we included ureteral strictures from all segments of the ureter and performed a variety of surgical techniques for each stricture and type. The etiology of stricture type also varied within our cohort. We acknowledge that the cohort was small and that outcomes may differ depending on individualized factors. Additionally, most of our patients (56.0%) underwent percutaneous nephrostomy tube placement for ureteral rest, as these patients were typically those who had flank pain associated with their stricture. We could not make any meaningful comparisons to those who decided to simply have their ureteral stents removed preoperatively as the mechanism of ureteral rest. Furthermore, our analysis did not include a control comparison group to determine whether ureteral rest is truly beneficial. Lastly, given the design of this study, we are unable to determine the ideal duration of ureteral rest; however, all patients in our cohort underwent ureteral rest for at least 4 weeks. The median duration of ureteral rest among those patients with a radiographical change in stricture quality from narrowed to obliterative was 15.4 (IQR: 5.8–26.5) weeks. Further larger cohort studies observing histopathological changes involved with ureteral rest may help to establish a recommended time period for ureteral rest.
Conclusions
Ureteral rest can lead to changes in stricture quality, which may be valuable in surgical decision-making. A period of ureteral rest may help reveal the true nature of a stricture, distinguishing narrowed from obliterative disease. This distinction is critical, as it may alter the surgical approach, prompting a shift from a non-transecting to transecting ureteroplasty when the stricture is found to be obliterative.
Institutional Review Board Approval
The present study protocol was reviewed and approved by the Institutional Review Board of Temple University. Informed consent was obtained by all subjects when they were enrolled.
Footnotes
Authors’ Contributions
M.L. and D.E.: Research conception and design. M.L., K.Z., and N.L.: Data acquisition. M.L.: Statistical analysis. M.L., D.E., O.A.: Data analysis and interpretation. M.L. and K.Z.: Drafting of the article. D.E. and O.A.: Critical revision of the article. D.E.: Administrative, technical, or material support. D.E. and O.A.: Supervision. M.L., D.E., and O.A. Approval of the final article.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
D.D.E. is a paid speaker, consultant, and proctor for Intuitive Surgical, a shareholder of Melzi Corp and has received trainee support from Hitachi Medical.