
Abstract
Introduction:
The clinical benefits of holmium laser enucleation of the prostate (HoLEP) for managing benign prostatic hyperplasia (BPH) are well-documented. However, HoLEP was performed in less than 5% of all BPH surgeries in the United States (US) prior to 2016, with large regional gaps in care. This study assessed temporal trends and geographic distribution of HoLEP utilization and providers in the US from 2018 to 2022.
Methods:
Claims data from Definitive Healthcare (2018–2022) were used to identify urologists who performed HoLEP and assess utilization across the US. HoLEP rates were calculated by dividing patients who underwent HoLEP by total patients with BPH who underwent any procedure for BPH. Active HoLEP surgeons were defined as those who performed ≥10 annual HoLEP procedures. Regional patient concentration was calculated by dividing patients with BPH by active HoLEP surgeons. Utilization trends over time were analyzed through Cochran-Armitage tests.
Results:
HoLEP utilization in the US increased by 52% between 2018 and 2022. The number of urologists performing HoLEP rose by 16%, from 386 in 2018 to 451 in 2022, while active HoLEP surgeons increased by 43% (106 to 151). High-volume surgeons performed 40.8% of all HoLEP cases in 2018 and 57.6% in 2022. States with ≥1 active HoLEP surgeon increased from 32 to 34, leaving 33% of states without a single active surgeon. The West (1050) and Northeast (786.3) had the highest BPH patient-to-surgeon ratios in 2018 and 2022, respectively, while the South had the best ratio and the most surgeons.
Conclusions:
HoLEP utilization has increased significantly, highlighting the growing demand in the US. Almost a third of states still lack access to an active HoLEP surgeon, and the high ratio of patients per provider in regions like the Northeast indicates a need for facilitating the dissemination of expertise to ensure equitable access to HoLEP.
Introduction
Benign prostatic hyperplasia (BPH) is a prevalent, potentially debilitating disease that affects patients as well as their partners and caregivers. 1 –7 Untreated BPH may result in serious urological complications, including acute and chronic urinary retention, hematuria, urinary tract infection, bladder stones, bladder wall damage, and renal incontinence. 5,6 Chronic lower urinary tract symptoms (LUTS) due to BPH may be associated with serious morbidity and can significantly affect quality of life due to loss of sleep and increased risk of falls, reduced productivity, impaired sexual function, social isolation, and clinical depression. 1 –4
Surgical treatment is an option for men with clinically significant LUTS attributable to BPH. 8 Transurethral resection of the prostate (TURP) is widely used to relieve BPH symptoms with good curative efficacy; however, TURP is associated with significant complications and morbidity. 9 Holmium laser enucleation of the prostate (HoLEP) has gained favor over the years and is considered an attractive alternative to TURP, photovaporization of the prostate (PVP), and minimally invasive surgical therapies (MIST) due to the significantly greater volume of prostate tissue removed, shallow energy penetration, and excellent hemostatic properties. 10 A recent systematic review and meta-analysis found that, compared with TURP, HoLEP had better curative efficacy, maximum urinary flow rates, lower post-void residual volumes, and improved International Prostate Symptom Scores (IPSS), with fewer adverse events such as hyponatremia, blood transfusions, and urethral strictures. 11 Another meta-analysis found significantly higher rates of blood transfusion, urethral strictures, bladder neck contracture, and urinary incontinence for open simple prostatectomy compared to HoLEP. 12 A cost-utility study in the United States (US) indicated that HoLEP, over a 5-year period, was more cost-effective in terms of both total costs and quality of life compared to TURP, prostatic urethral lift (PUL), transurethral waterjet ablation (TWA), and simple prostatectomy. 13
Although the clinical benefits of HoLEP for managing BPH are well-documented and increasingly recognized, 5 access to the procedure remains limited in the US. 14,15 Prior to 2016, less than 5% of all BPH surgeries were HoLEP. 14,15 This study used contemporary data to assess recent temporal trends in HoLEP utilization and to describe the geographic distribution of HoLEP utilization and HoLEP providers in the US from 2018 to 2022.
Methods
Data source
This retrospective, observational, real-world data study identified providers who performed HoLEP using medical clearinghouse claims data obtained from Definitive Healthcare’s Atlas All-Payor Claims Dataset from 2018 to 2022. The Atlas All-Payor Claims Dataset by Definitive Healthcare compiles de-identified medical claims from commercial, Medicaid, Medicare, Medicare Advantage, Veteran’s Affairs (VA)/Champus, and other miscellaneous payors that comprise approximately 60–70% of claim volume in the US, including Puerto Rico. The data includes hospital and medical claims from a wide range of settings, including physician groups, ambulatory surgical centers, hospitals, accountable care organizations, clinically integrated networks, etc. Therefore, both hospital- and clinic-based procedures are captured.
Study measures
HoLEP utilization rates were calculated by dividing the number of patients who underwent HoLEP by the number of total patients with a BPH diagnosis who underwent a procedure for BPH treatment, including TURP, water vapor thermal therapy, PVP, TWA, PUL, and implantable nitinol device. The BPH procedures were identified through current procedural terminology, Healthcare Common Procedure Coding System, and International Classification of Diseases, Tenth Revision codes (see Supplementary Table S1). We restricted the cohort to surgeons with a primary specialty of urology. The number of HoLEP procedures per HoLEP provider was evaluated, and providers were categorized as any HoLEP (≥1 HoLEP procedure), active HoLEP (≥10 HoLEP procedures), and high-volume HoLEP (≥50 HoLEP procedures). The definition of an active HoLEP surgeon was in accordance with previously published research on HoLEP in the US. 14
The primary practice location of each HoLEP surgeon was identified and used to create geographic maps of HoLEP rates in 2018 and 2022. Regional patient concentration was calculated by dividing the number of patients with BPH treated by a HoLEP surgeon by the number of active HoLEP surgeons. Utilization trends over time were analyzed through Cochran-Armitage tests, and a p-value of less than 0.05 was considered indicative of statistical significance. The study was determined to be exempt from Institutional Review Board approval, as this research project did not involve human subjects and used data from an anonymous, de-identified, medical clearinghouse administrative claims database compliant with the Health Insurance Portability and Accountability Act of 1996.
Results
Study findings showed that HoLEP utilization in the US significantly increased by 52% over 5 years between 2018 and 2022 (p < 0.01), though it remained low at 6.7% of total BPH procedures. The total number of BPH procedures varied year-to-year, with an overall upward trend (Fig. 1). The number of urologists performing at least one HoLEP procedure rose by 16%, from 386 surgeons in 2018 to 451 surgeons in 2022. Meanwhile, the number of active HoLEP surgeons increased by 43%, from 106 surgeons in 2018 to 151 surgeons in 2022. The number of high-volume HoLEP surgeons who performed at least 50 HoLEP procedures increased by 92%, from 22 surgeons in 2018 to 41 in 2022 (Fig. 2). High-volume HoLEP surgeons accounted for an increasing proportion of all HoLEP procedures, from 40.8% in 2018 and 57.6% in 2022.
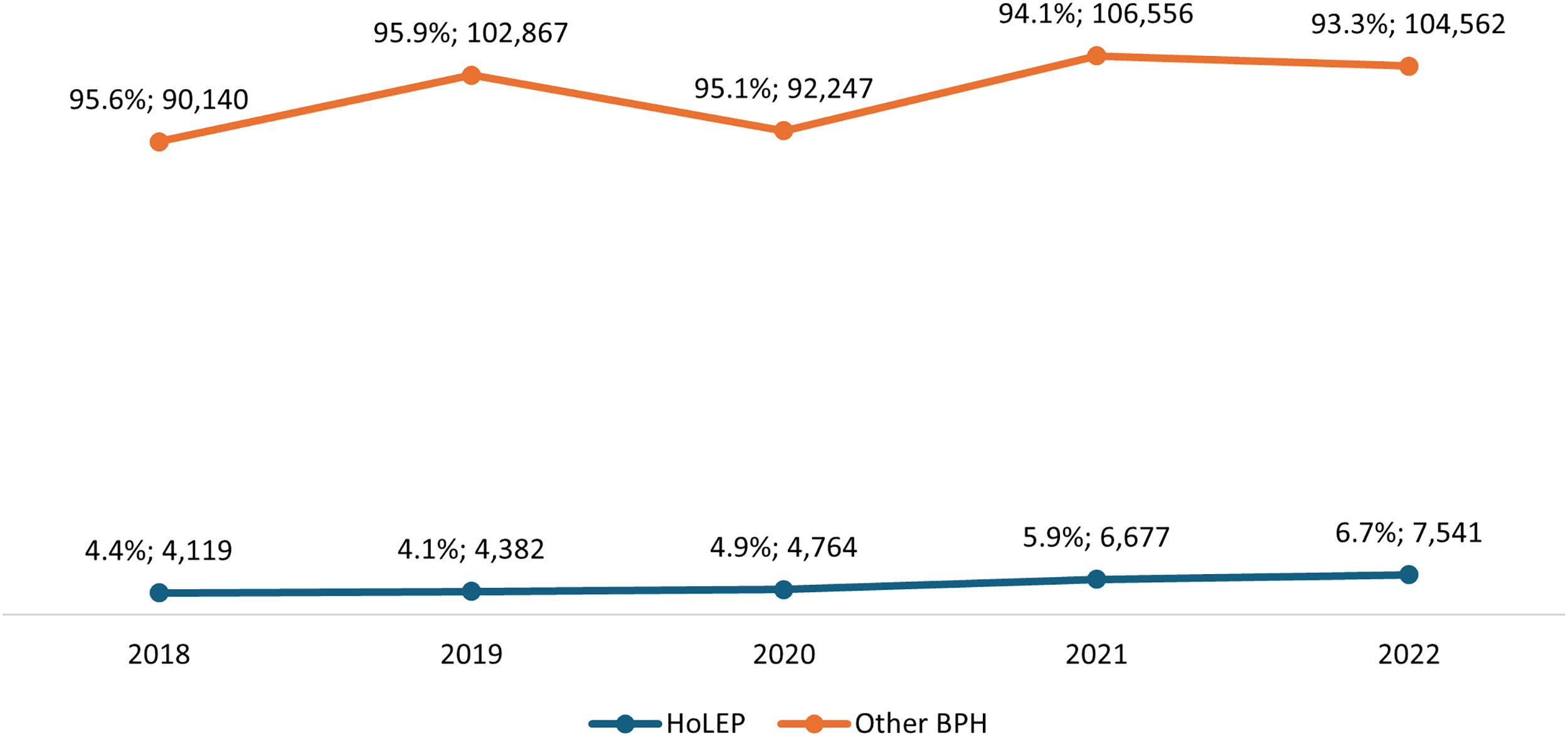
Proportion of HoLEP vs other BPH procedure utilization in the US between 2018 and 2022.
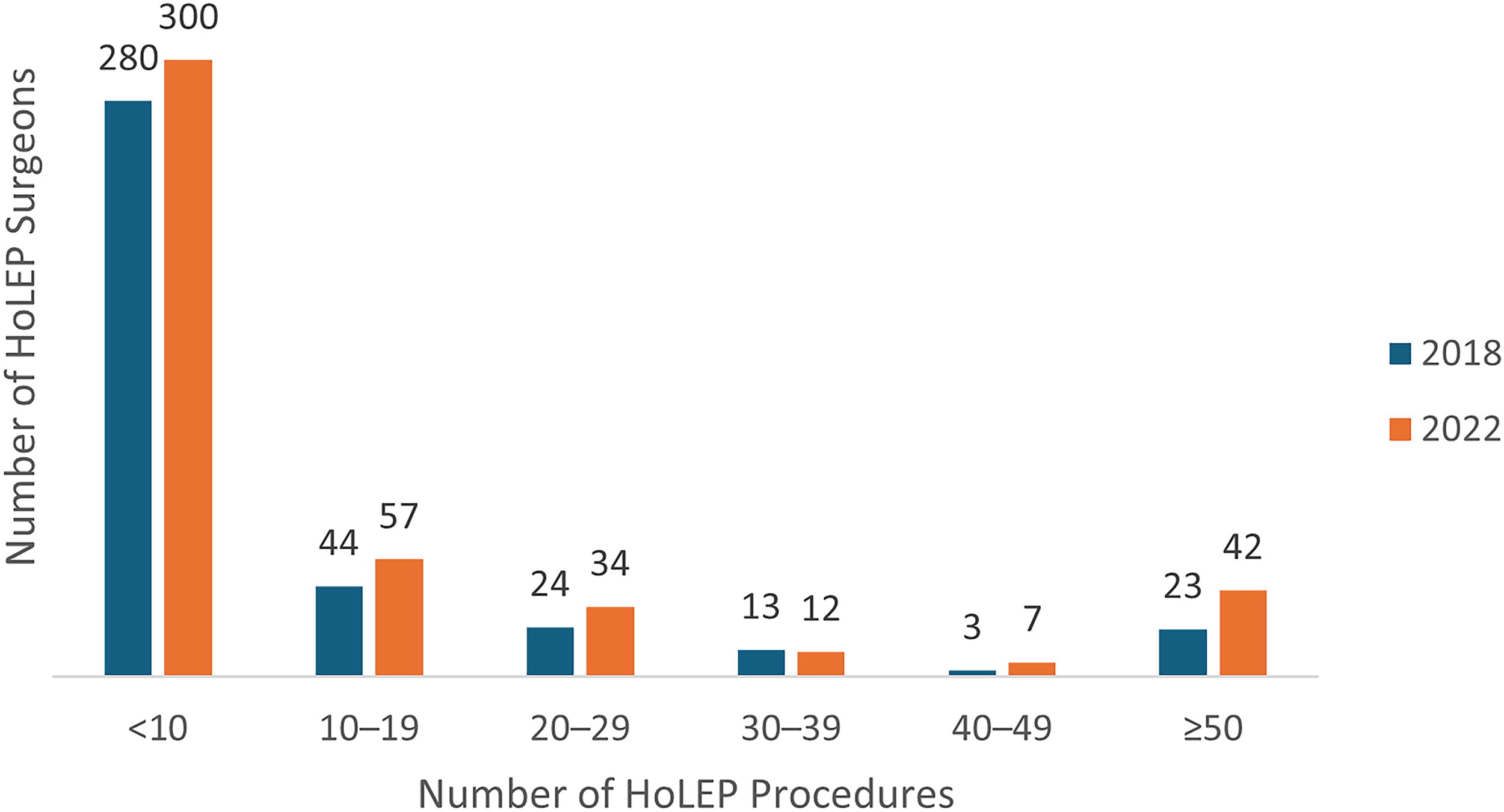
Distribution of HoLEP procedure volumes performed by surgeons in 2018 vs 2022 in the United States.
From 2018 to 2022, states with at least one active HoLEP surgeon increased only from 32 to 34 (including Washington, DC), leaving 33% of states without a single active surgeon. The South had the greatest number of active surgeons in both 2018 and 2022 (51 and 52, respectively), while the West had the fewest in 2018 with 11 surgeons and the Northeast the fewest in 2022 with 24 surgeons (Fig. 3). In 2018, the West had the worst overall patient concentration of 1050 patients with BPH per active surgeon, while the South had the best overall concentration at 889.5 patients per active surgeon. In 2022, the Northeast had the worst overall patient concentration of 786.3 patients with BPH per active surgeon, while the Midwest had the best overall concentration at 558.1 patients per active surgeon. Figure 4 demonstrates that states with at least 100 annual HoLEP procedures increased 46% from 15 to 22 (including Washington, DC).
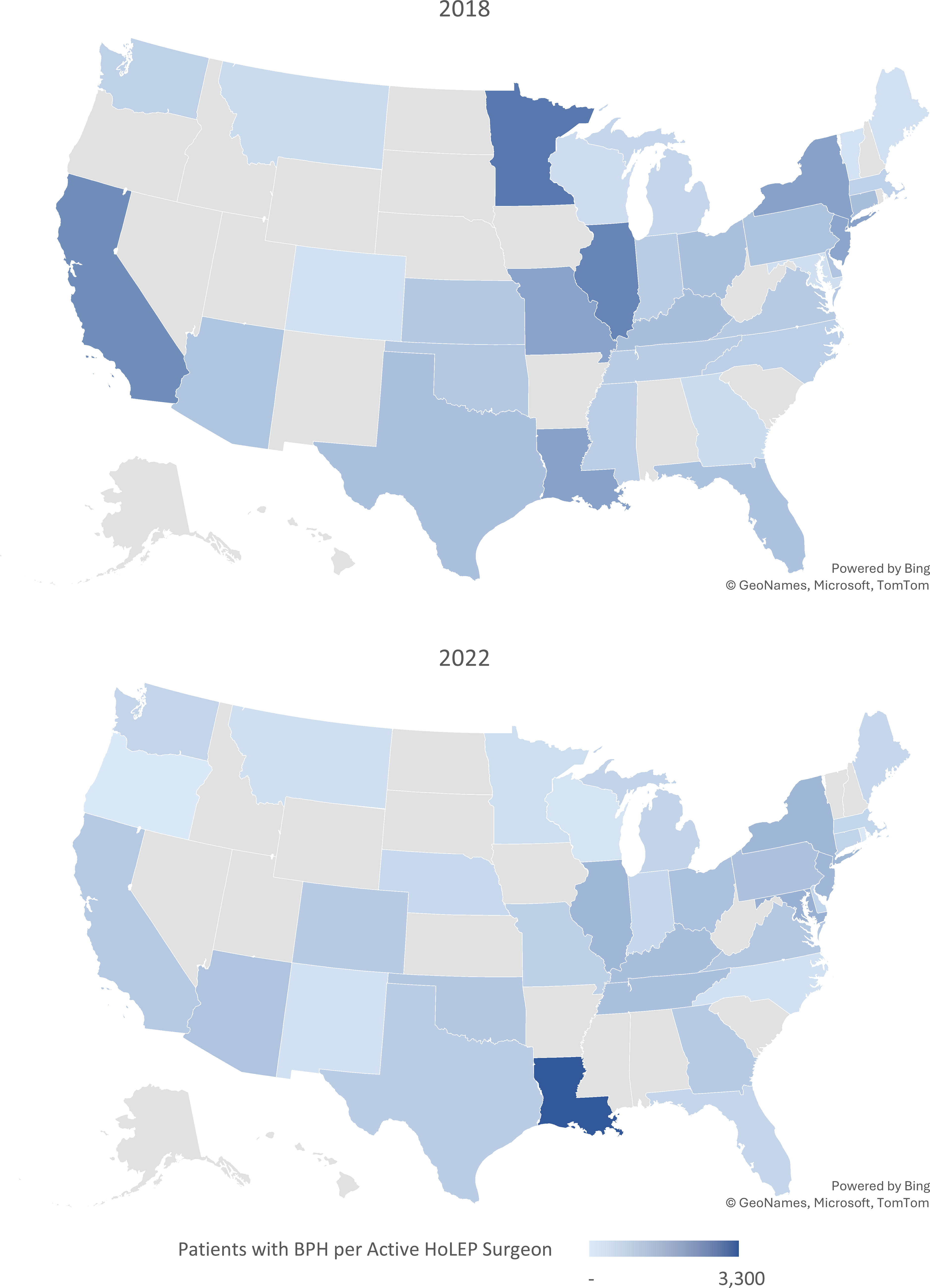
Geographic distribution of concentration of patients with benign prostatic hyperplasia by active holmium laser enucleation of the prostate (HoLEP) surgeons (10+ HoLEP procedures annually) in the US in 2018 vs 2022.

States with at least 100 annual holmium laser enucleations of the prostate performed in 1 year.
Discussion
The goal of BPH treatment is to prevent disease progression that would diminish health and result in more invasive surgical procedures. HoLEP is an extremely durable and effective treatment for patients suffering from LUTS due to BPH. 16 Compared to TURP, PVP, and MIST procedures, HoLEP has been shown to have better curative efficacy and a lower incidence of adverse events in patients with BPH. 11 The European Association of Urology (EAU), American Urological Association (AUA), and the National Institute for Clinical Effectiveness guidelines on the surgical treatment of BPH recommend HoLEP as a size-independent treatment option for men with moderate to severe BPH symptoms. 17,18 HoLEP is an excellent option for many patients who may not be good candidates for other procedures based on prostate size, age, or bleeding risk. 16,19
The findings of this study demonstrate a positive trend in the utilization and geographic distribution of HoLEP across the US and highlight a shift toward adopting HoLEP; however, overall utilization remains low, suggesting the need for continued support and training to ensure wide patient access to HoLEP care. A survey of urologists (69.8%) and urologist trainees/residents (30.2%) from the from EAU Section of Uro-Technology (ESUT) found that 71.9% had seen HoLEP performed, but only 53.2% had performed HoLEP themselves in surgical practice. 20 Interestingly, a greater proportion of the urologists chose HoLEP as a treatment option for themselves as a patient (40%) than what they would choose as an option for their patients (25%). 20
Our study findings regarding US HoLEP utilization and geographic distribution build upon those of previously published studies. 14,15,21 A previous study using Medicare claims found that total surgical BPH treatment volume decreased 24% from 2008 to 2014, while HoLEP volume and regional adoption tripled. 14 Data from the American College of Surgeons National Surgical Quality Improvement Program found that rates of HoLEP were only 5% of all BPH procedures in 2015. 15 Our study found that the HoLEP utilization rate between 2018 and 2022 increased by more than 50% but remained low at 7%. In 2014, over half of states had ≤1 active HoLEP surgeon, 14 and our data demonstrate that in 2022 almost 1/3 of states still did not have any active HoLEP surgeons. Though the volume of both active and high-volume HoLEP surgeons has significantly increased from 2018 to 2022, they tend to be concentrated in states where there are already other HoLEP surgeons.
A retrospective cohort study evaluating patients that underwent HoLEP at the Mayo Clinic in Phoenix, Arizona, from 2007 to 2019 found that 44.2% of patients traveled from out-of-state for HoLEP care, traveling a median of 597 miles. 21 Patients who came from out-of-state had larger prostates and worse preoperative IPSS scores, potentially reflecting delayed treatment due to lack of access to care. While we found that there were increasing numbers of active HoLEP surgeons in previously underserved regions of the US, such as the West, persistent large regional gaps in care and the high ratio of patients per provider in regions like the Northeast underscore a need to address disparities in the availability of HoLEP care in the US.
Several factors may contribute to these disparities. First, there are a limited number of training programs that provide some level of exposure to HoLEP—only six out of 49 US-based endourology fellowships listed HoLEP as a component of training as of 2019. 22 Additionally, HoLEP is a procedure that has a learning curve and requires specialized equipment, which may deter some hospitals and surgeons from adopting it. As a result, surgeons trained in HoLEP, particularly those who learned the procedure during their fellowship programs, may be concentrated in regions where these programs are located, leading to scarcity in other areas.
Our study findings also showed that most surgeons performed at least one but less than 10 HoLEP procedures per year. It is possible that these physicians were trained but do not regularly perform HoLEP due to the barriers to utilization (i.e., learning curve, amount of time and dedication required to proficiently perform HoLEP, and requirement for specialized equipment). 22 Some physicians may have been trialing the procedure, changed practice settings, or experienced shifts in their clinical focus during the study period. Additionally, some may prefer to offer alternative BPH procedures that are more established within their clinical workflow. 17,18
Structured HoLEP training programs 23 and mentored HoLEP training 22 have been shown to be beneficial in helping overcome the steep learning curve of HoLEP. Studies have also shown that most surgeons who receive HoLEP training in a fellowship program are comfortable completing HoLEP independently and go on to incorporate HoLEP into their practice after the fellowship training. 22 Addressing the barriers to HoLEP utilization by expanding training opportunities, both the number of fellowship training sites and facilitating the dissemination of expertise to allow urologists to receive training outside of fellowship, may help to ensure equitable access to HoLEP across the US. Professional societies and urologist opinion leaders may also work to improve patient and physician awareness of the benefits of HoLEP in order to increase utilization.
Strengths of this study include the large number of patients available for analysis and comparison from a variety of payor sources, the granularity of geographic data, and the ability to quantify the number of HoLEP procedures per surgeon. The study used administrative data, and it is important to keep in mind that billing data are not designed specifically for research purposes and may have clerical inaccuracies. Detailed information about potentially important clinical variables is not available. 25,26 The study is also limited in that the findings from the Definitive Healthcare database may not be generalizable to all patients in the US or to patients in other countries, as claims databases often represent a subset of the population with specific types of insurance coverage and may exclude key demographic groups and geographic areas. However, our inclusion of private, Medicaid, Medicare, and VA populations does cover the majority of payor and patient groups. Another limitation of this study is that geographic data were only available for HoLEP procedures and not for other BPH treatments, precluding a comparative geographic analysis across all modalities. Additionally, while normalization of HoLEP volume to state population was considered, we opted against it due to the potential for confounding by factors not fully captured in our dataset, including differences in age distribution, BPH prevalence, comorbidities, healthcare access, provider availability, and insurance coverage. Presenting raw HoLEP volumes by state avoids over-simplification, but limits interpretability of geographic variation.
Conclusions
A strong upward trend in HoLEP utilization in the US over 5 years, coupled with an increase in both the overall number of HoLEP surgeons and the proportion of patients being treated by high-volume HoLEP surgeons, underscores growing demand for HoLEP in the US. The findings demonstrate a positive trend in the geographic distribution and utilization of HoLEP across the US, with increasing numbers of active HoLEP surgeons in previously underserved regions. However, almost a third of states still lack access to an active HoLEP surgeon, and the high ratio of patients per provider in regions like the Northeast underscores a need to address disparities in the availability of HoLEP care in the US. Enhancing training programs, promoting awareness, and facilitating the dissemination of expertise may help ensure equitable access to HoLEP.
Footnotes
Acknowledgments
The authors would like to thank Natalie Edwards of Health Services Consulting Corporation for her assistance in preparing this article. This abstract was previously published in the Journal of Endourology, Vol. Thirty-eight, No. S1, Abstracts of the 41st World Congress of Endourology and Urotechnology (WCET 2024). ![]() .
.
Authors’ Contributions
J.R. and N.L.M.: Study design, data interpretation, and article writing and editing; Y.E.S. and S.R.: Study design, implementation of data analysis, data interpretation, and article writing and editing.
Data Availability
The data that support the findings of this study are available from the corresponding author.
Ethics Committee Approval
Ethics approval from an institutional review board and informed consent were not required for this study as de-identified claims data was used.
Author Disclosure Statement
J.R. and N.L.M. are practicing urologists and were not compensated for their participation in this study; however, each serves as a consultant for Boston Scientific in other capacities. S.R. is an employee of Boston Scientific when the study was conducted and holds stock options within the company. Y.E.S. is a graduate student at the University of Cincinnati and is not a Boston Scientific employee; however, she is working on a Global Health Economics and Market Access project with Boston Scientific.
Funding Information
The study was supported by Boston Scientific.
Supplementary Material
Supplementary Table S1
Abbreviations Used
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.