
Abstract
Introduction:
Ureteral stricture after renal transplantation has a reported incidence of 1.4%–4.7%. This is classically repaired using an open surgical approach. The objective of this case series is to demonstrate the feasibility and effectiveness of robot-assisted repair for ureteral stricture following kidney transplantation.
Methods:
Between November 2021 and May 2024, 10 patients underwent robot-assisted repair. Nephrostomy tubes were placed in all patients prior to the robotic repair. Patients were positioned supine with Trendelenburg tilt, and robotic ports were arranged in a W configuration. Indocyanine green was administered through the nephrostomy tube. If necessary, the pre-stented native ureter was identified and dissected. The reconstructive technique was tailored to the location and length of the stricture. Ureteral stents were placed for 4–6 weeks.
Results:
Patient demographics transplant characteristics, and details of stricture repair techniques along with associated outcomes were analyzed. Strictures were located at the ureterovesical anastomosis in eight patients, at the ureteropelvic junction in one patient, and at multiple sites in one patient. Repair techniques included ureteroneocystostomy (five patients) and Boari flap reconstruction (two patients). The native ureter was used in three patients (two ureteroureterostomies and one ureteropyelostomy). A bladder hitch was performed in two patients. Median operative time was 255.5 minutes, blood loss was 62 mL, and the hospital stay was 2 days. Postoperative complications occurred in two patients, and five patients required readmission within 30 days. At 3-month follow-up, all patients had excellent renal allograft function (median serum creatinine = 1.63 mg/dL) and were nephrostomy tube- and stent-free.
Conclusions:
Robotic repair of ureteral stricture following kidney transplantation is a safe, minimally invasive approach with reduced postoperative pain and shorter hospital stays. This approach should be considered the primary treatment option for renal transplant ureteral strictures and included within the renal transplant surgeons’ repertoire of procedures.
Keywords
Introduction
Kidney transplantation stands as the optimal choice for enhancing both quality of life and survival rates in individuals with end-stage renal disease. 1 However, this procedure is not without its complexities, and recipients face a spectrum of complications that vary in severity, influencing both patient and graft survival.
Among these complications, ureteral stricture following kidney transplantation has an estimated incidence ranging from 1.9% to 3.7%. Despite its relatively low frequency, it is the reason behind 78% of reoperations after kidney transplantation. 2 Ureteral ischemia emerges as the primary culprit for transplant ureteral strictures (TUSs), with factors such as multiple renal arteries and advanced donor and recipient age contributing to an elevated risk.3,4
The manifestations of TUS are diverse, ranging from asymptomatic gradual decline in kidney function to abdominal pain, recurrent urinary tract infections (UTIs), and, in severe cases, life-threatening sepsis. 5 Given these challenges, various management modalities with variable success rates and morbidity profiles have been explored. Endoscopic interventions, often used as first-line solution, have low morbidity but are associated with 55% success rate. 6 A substantial portion of patients ultimately requires open surgical correction that is associated with 92% success rate but a heightened morbidity profile.6–8
In broader context of ureteral stricture management, robotic approach is proven effective in managing non-TUSs. 9 Emerging case series have demonstrated feasibility of robotic surgical correction for TUS.10–12 This study aims to contribute to the growing body of knowledge by detailing our experience in robotic management of TUS, emphasizing the diverse techniques employed. We aim to highlight our individualized approach to plan and execute a plan to manage TUS robotically.
Materials and Methods
Study design
This retrospective analysis encompasses ten cases of TUS treated with robot-assisted laparoscopic repair between November 2021 and May 2024 at our institution. Following Institutional Review Board (IRB # 24-493) approval, we collected transplant details, preoperative, operative, and postoperative data.
Patient selection and preoperative planning
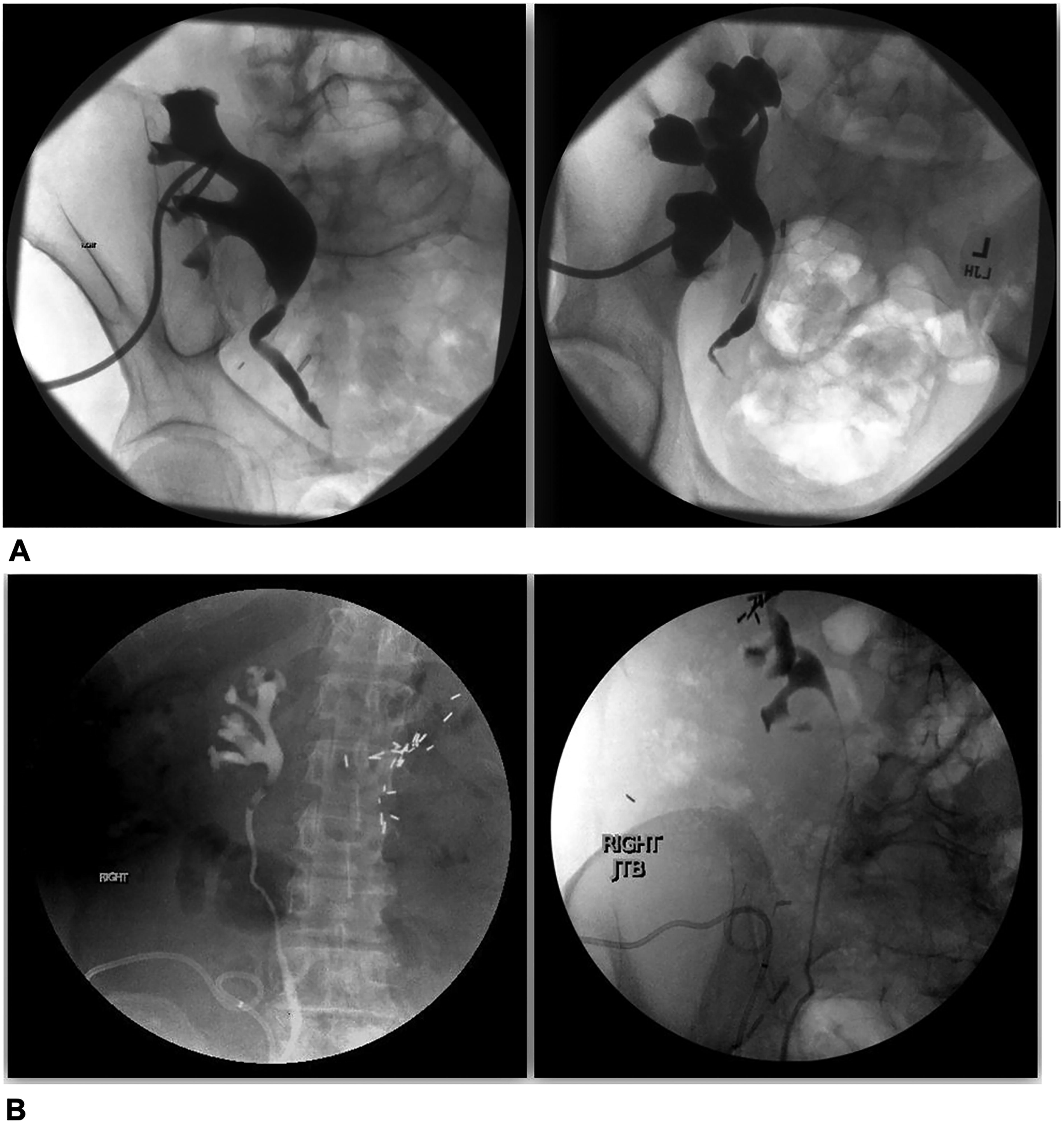
Patients included in the study met the criteria of having TUS. All patients had a nephrostomy tube in place prior to procedure. Confirmation of stricture location and length was performed using preoperative nephrostograms (Fig. 1A). The laterality of kidney graft is important to be known in relation to the laterality of graft placement site. The renal pelvis of grafts placed on the contralateral side is expected to be more superficial than the grafts placed on the ipsilateral side. This is particularly important in managing more proximal strictures. Patients are counseled on the possible need for ipsilateral nephrectomy if native ureter is utilized for reconstruction.
Patient positioning and port placement
During procedure, if the use of native ureter is anticipated, retrograde study is performed to confirm the patency of ipsilateral native ureter followed by stent placement. The native ureter caliber can be expected to be small especially in patients with no urine output prior to transplant for an extended number of years (Fig. 1B). All patients were positioned supine with slight Trendelenburg tilt with meticulous padding of pressure points. The camera port is placed 8–10 cm above the umbilicus. The right robotic arm port is placed 8–10 cm lateral to the camera port along the same horizontal line. The assistant port is placed 8–10 cm lateral to the right robotic port just inferior to the costal margin. The two left robotic arm ports are placed 8–10 cm apart at more caudal level, helping camera port point downward and to the left. This setup allows for better triangulation toward the target anatomy, which is in the right iliac fossa (Fig. 2).
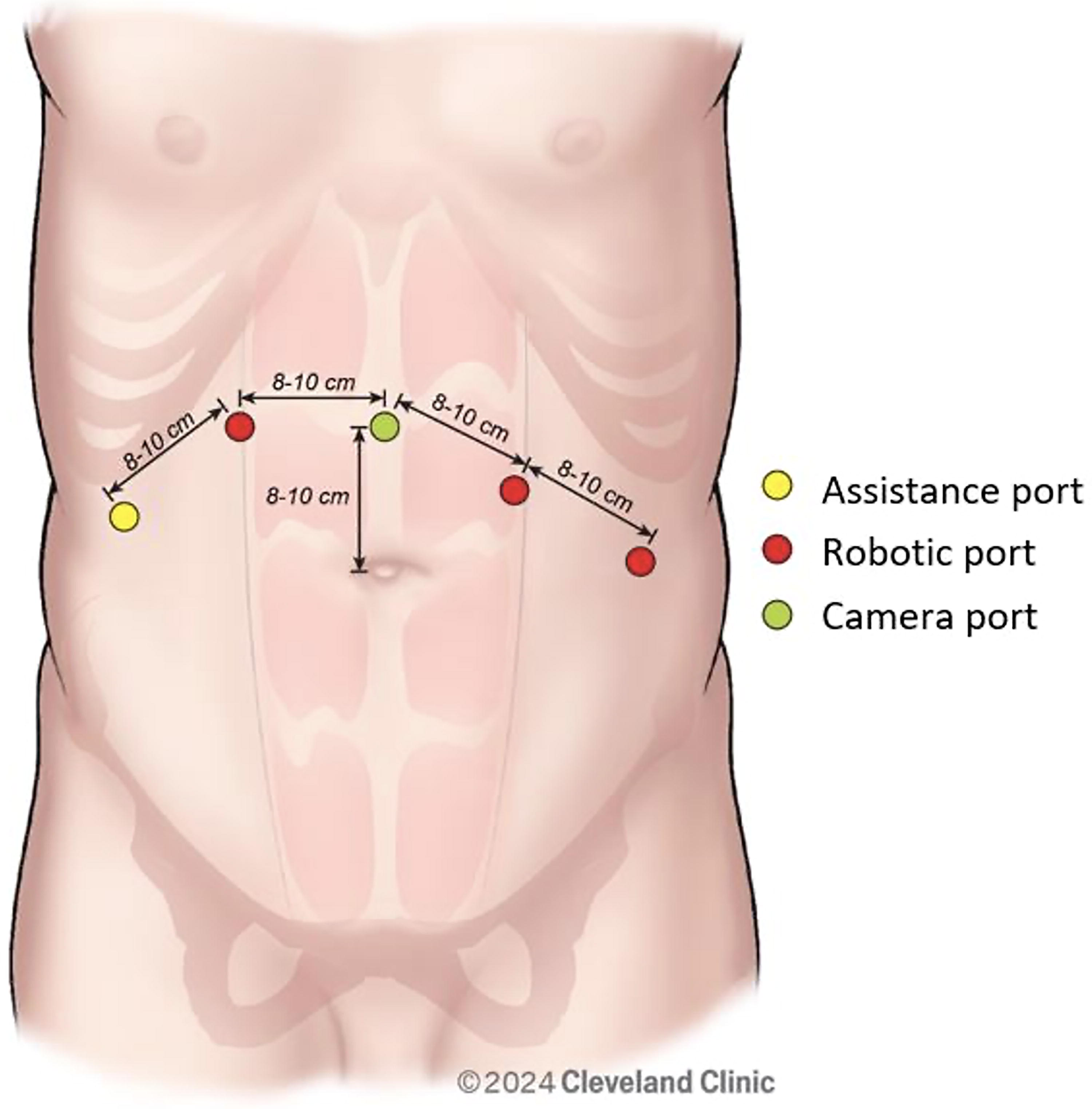
Robotic port placement during repair of transplant ureteral stricture.
Localization of transplant ureter
After gaining access, bladder is dropped starting with side of the transplant graft reaching the extraperitoneal space. The ureter can be expected in the space between lower pole of graft, the ipsilateral medial umbilical ligament, and the round ligament/vas deferens (Fig. 3A). In densely scarred patients, filling the bladder can help in identifying ureterovesical junction. Given the variability in the location of transplant ureter, we used indocyanine green (ICG) solution injected through the nephrostomy tube. ICG provided enhanced fluorescence, aiding identification of renal pelvis and ureters (Fig. 3B). It is important to note that the utility of the ICG is limited in densely scarred ureter. After identifying the ureter, it is isolated with vessel loop. Careful dissection is warranted, as proximity and adhesions to the graft vasculature or the external iliac vessels can be expected. The stenotic segment is excised, the proximal healthy ureter is spatulated, and the defect length is measured (Fig. 3C). When needed, a flexible scope through the assistant port was also used to ensure the passage of stricture.
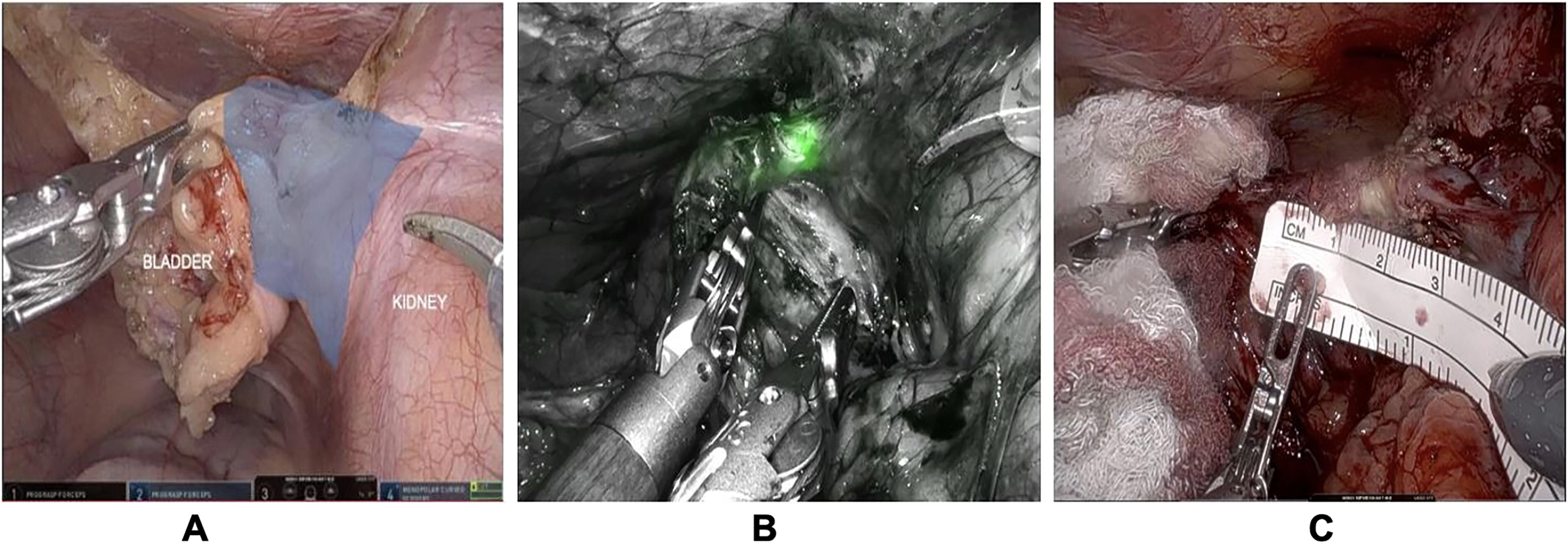
Localization of the ureteral stricture.
Surgical options
Ureterovesical anastomosis
Used in cases of short segment strictures and good bladder mobility. The old cystostomy is closed, and a new one is made in an appropriate location. The anastomosis is reconstructed using interrupted 4-0 Vicryl sutures (Fig. 4A). Bladder filling is routinely done to check for watertightness (Fig. 4B).
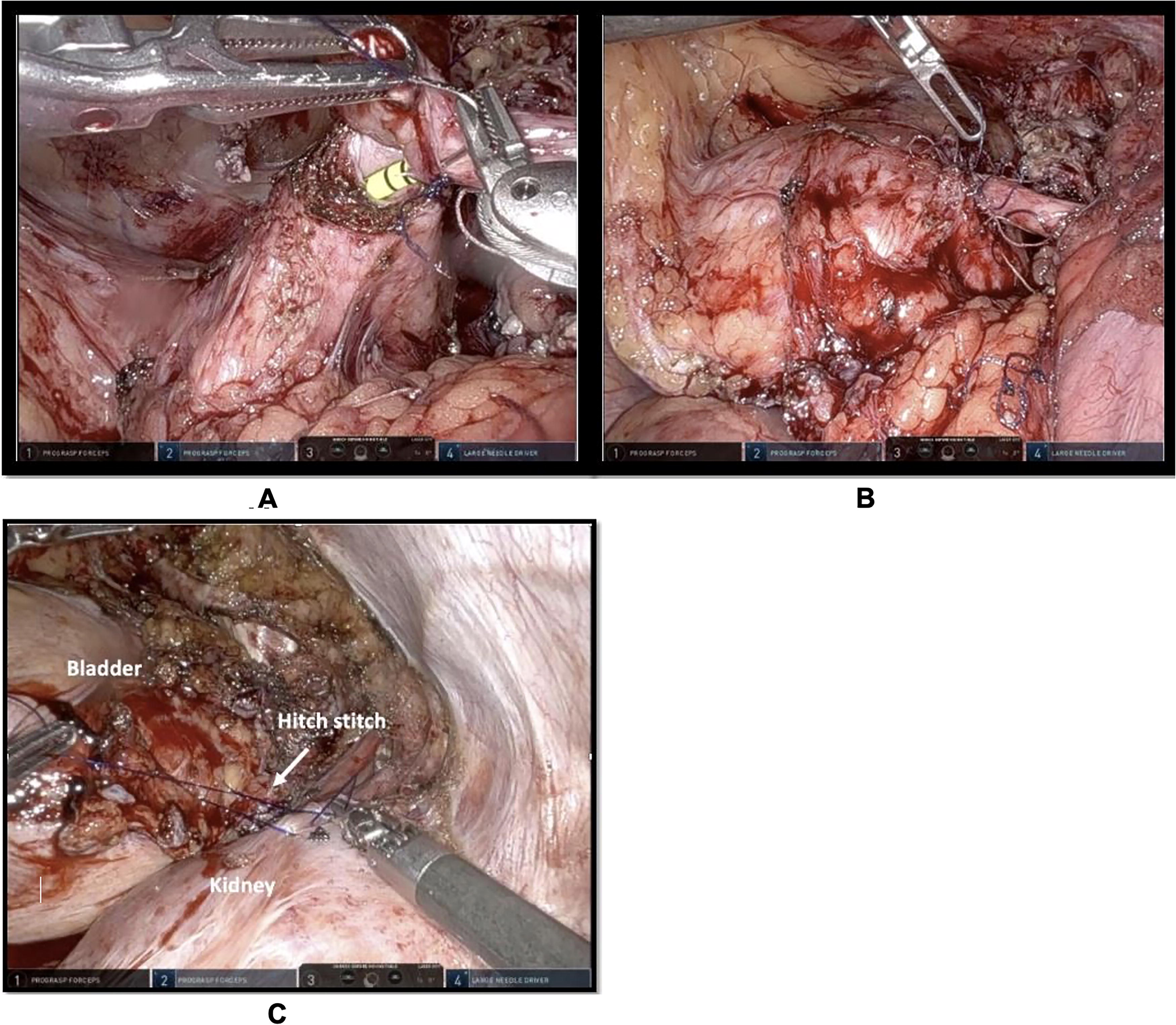
Ureterovesical anastomosis.
Bladder hitch
When the new ureterovesical anastomosis is expected to be under tension, bladder hitch can be performed. The bladder is filled with saline mixed with methylene blue, and the bladder is mobilized. A Polydioxanone Suture (PDS) is used between the bladder and the peritoneum covering the graft to bring the cystostomy site closer to the transplant ureter to allow for tension-free anastomosis (Fig. 4C).
Uretero-ureteral and ureteropelvic anastomosis with the native ureter
Used in longer segment strictures and/or small or thickened defunctionalized bladders. This surgical option carries the advantage of being antirefluxing, which is beneficial in a certain cohort of patients with recurrent cystitis and pyelonephritis. The dissection is carried out proximally and distally without stripping the ureter to preserve its blood supply. The native and transplant ureters are both spatulated, and anastomosis is constructed using running 4-0 Vicryl sutures over a ureteral stent (Fig. 5A). After passing the stent into the bladder through the native ureter, the guidewire is reinserted through one of the stent’s side holes to facilitate passing the stent into the transplant pelvis (Fig. 5B). Clipping the ureter and staging the nephrectomy later if needed is also a feasible option. 13 Alternatively, an end-to-side anastomosis between the graft ureter and native ureter could be considered to preserve the drainage of the native kidney. 14
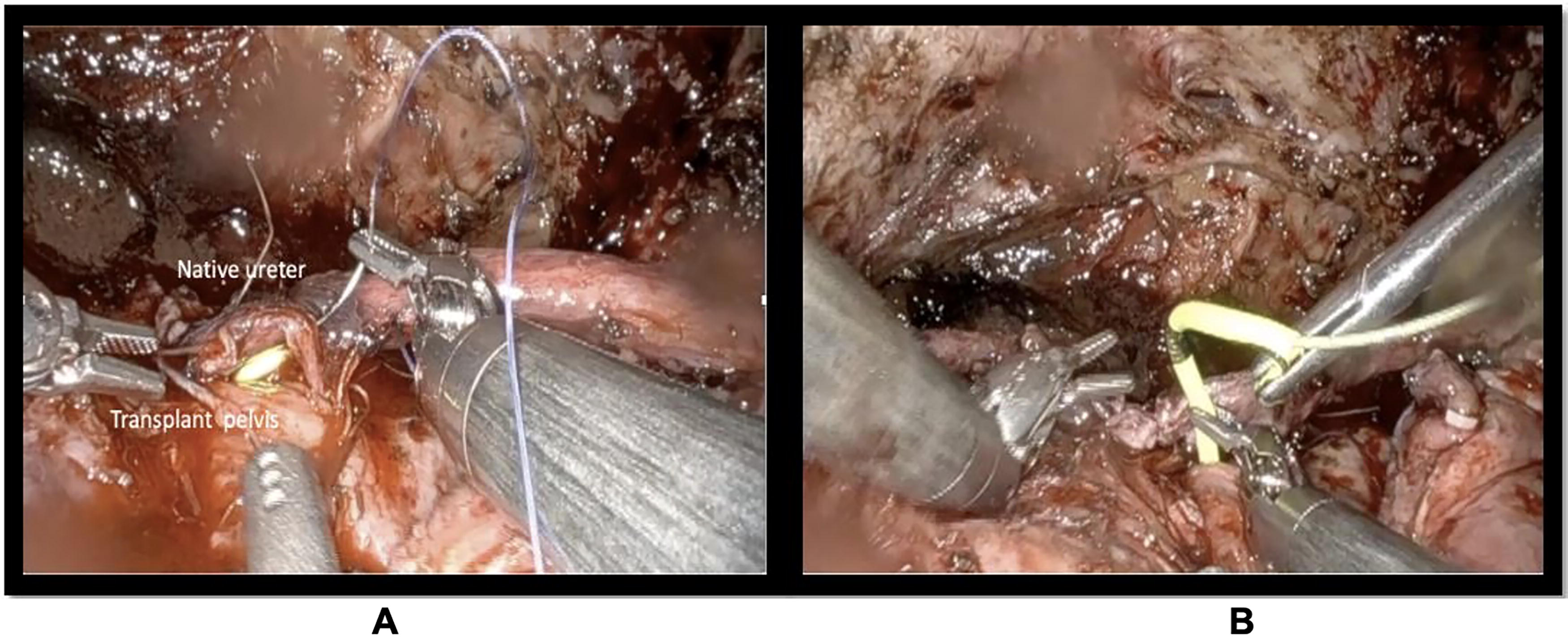
Ureteropelvic anastomosis.
Boari flap
A Boari flap could be used in cases of long strictures and good bladder capacity and mobility. The bladder is filled with saline, and the triangular Boari flap is marked using electrocautery (Fig. 6A). The flap is designed so that the base is toward the graft side rather than the upper part of the bladder. The anastomosis is constructed between the transplant ureter and the flap using running Vicryl sutures over a stent (Fig. 6B).
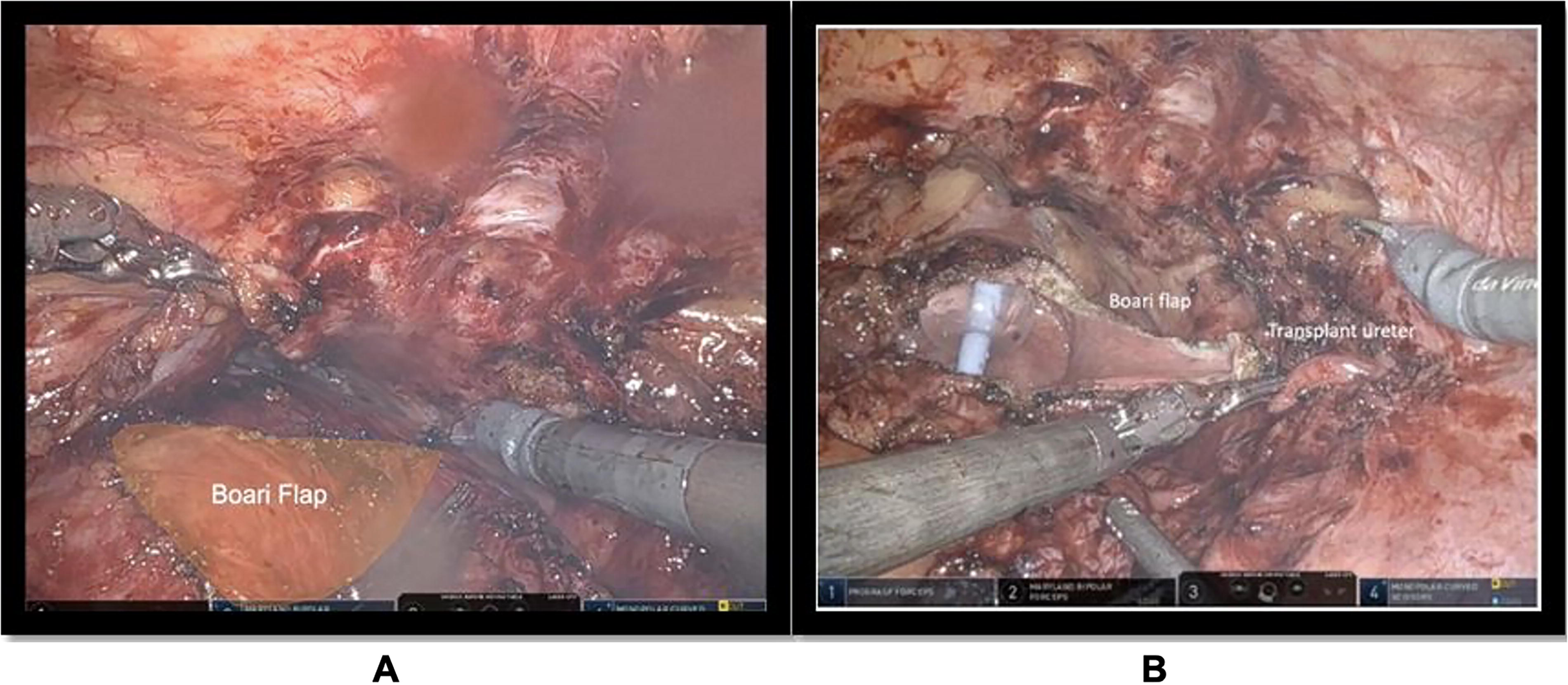
Boari flap reconstruction.
Customized Robotic Repair of Transplant Ureteric Strictures: Surgical Tips & Tricks and Common Pitfalls
Nephrostomy tubes were clamped at the end of the procedure. A ureteral stent remained in place for 4–6 weeks, removed by outpatient cystoscopy. Creatinine levels were obtained weekly after stent removal, and an ultrasound was ordered at 3 months.
Results
Demographics
The demographic characteristics are summarized in Table 1. A total of 10 patients, 7 males and 3 females, underwent robotic repair of TUS. The median age was 51.5 years, and median BMI was 28.1 kg/m2.
Demographics and Preoperative Outcomes

ADPKD = autosomal dominant polycystic kidney disease; BMI = body mass index; DM = diabetes mellitus; ESRD = end stage renal disease; HTN = hypertension; UOP = urine output.
Transplant episode
The details of kidney transplant episodes are described in Table 2. Of 10 patients, 1 had robotic kidney transplant, and 3 patients received living donor kidneys. Among the 10 donated kidneys, 8 had a single renal artery, whereas 2 kidneys had multiple renal arteries (1 with 2 arteries and the other with 3). Delayed graft function, defined as the necessity for dialysis within the first week posttransplant, was observed in six patients. Additionally, six patients experienced episodes of UTIs necessitating antibiotic treatment. The presence of BK virus was detected in one patient. Notably, 5 out of 10 patients exhibited acute rejection upon biopsy.
Kidney Transplant Episodes

CIT = cold ischemia time; DGF = delayed graft function; UTI = urinary tract infection; WIT = warm ischemia time.
Stricture diagnosis
Patients were assessed for TUS based on various presenting symptoms, including lower flank pain, recurrent UTIs, a continuous increase in serum creatinine levels, and the presence of hydronephrosis. The diagnoses of TUS were established through nephrostograms. The median duration from transplant to the diagnosis of TUS was 135 days. Notably, three patients had previously undergone surgical repairs for TUS (Table 3).
Stricture Repair and Outcomes

LOS = length of stay; UTI = urinary tract infection.
Stricture repair
The median total operative time for robotic repair was 255 minutes, with median blood loss of 62 mL. The choice of repair technique was planned based on the stricture length, bladder size and mobility, and the presence of the ipsilateral native ureter. Five patients underwent ureterovesical reimplant, as the strictures were located more distally. In two of these patients, bladder hitch was performed as an adjunct procedure when the anastomotic tension was anticipated. In two patients, transplant ureters were anastomosed with the native ureter (uretero-ureteral), whereas ureteropelvic anastomosis was performed in one patient with multiple-level strictures. In two patients, Boari flap was used to bridge a larger ureteral defect (3 cm). All anastomotic repairs except for the Boari flap were done in an interrupted fashion. One patient had an injury to right external iliac vein that was promptly repaired intraoperatively without any complication (Supplementary Fig. S1).
Outcome
The median length of stay following robotic repair of TUS was 2 days. Two patients experienced postoperative complications: one patient who had undergone native uretero-ureteral repair presented with continuous flank pain, necessitating a left laparoscopic native nephrectomy. The second patient encountered an occlusion of ureteral stent, requiring stent exchange. Within 30 days postoperatively, five patients required readmission: three for acute kidney injury (two with UTI), one for the rejection, and one for the stent exchange. Notably, no instances of urine leak or hematoma were observed in any patient. Median serum creatinine levels at 1 month were 1.89 postoperatively, which trended down to 1.63 at 3 months after repair. At last follow-up, all patients were nephrostomy- and stent-free with no evidence of obstruction on follow-up imaging.
Discussion
TUS is one of the delayed surgical complications that can impact the graft functions and can be devastating to manage. 2 The presumed cause of TUS is the ischemia to the distal ureter, but there are few other factors that contribute to this complication, including advanced recipient and donor age, the presence of multiple renal arteries, delayed graft function, and length of the graft ureter. Also, infections such as the BK virus can play a role in ureteral strictures.2,8,15,16 The main preventive surgical concepts include preserving the periureteral tissue, trimming the ureter to the shortest length possible, and delicate handling of the ureter. 17 However, because of the existence of multiple factors for TUS, complete elimination of this problem is not possible, and reliable management has to be planned and implemented.
TUS poses challenging surgical dilemma. Open procedure was traditionally viewed as the gold standard for treating this complication because of its high success rate of 92%.4,7 The procedure is typically morbid and technically difficult as it necessitates going through the old transplant incision usually encountering dense scarring. The role of endoscopic procedures such as balloon dilatation and stricture incision has continuously grown in the past few decades. Although minimally invasive, success rate of balloon dilatation is 51% on the first attempt and declines significantly with each attempt. Such a low success rate is to be accepted given the ischemic etiology of the strictures in most of the cases and the high prevalence of >1 cm strictures.6,18 Placement of indwelling catheter with regular exchange is also feasible; however, most of those patients end up with recurrent episodes of antibiotic-resistant infections in the long run. This is specifically suboptimal in this immunocompromised patient population. 19
Robotic repair of ureteral stricture carries the advantage of being minimally invasive while allowing definitive repair of the TUS. The use of the robotic platform has been shown to reduce the risk of wound complications, decrease the hospital stay, and hasten recovery.9,20,21 The intraperitoneal approach avoids the older surgical field and provides faster and easier access to the stricture area.
Recently, Heidenberg et al. 10 reported series of 41 patients who underwent robotic reconstruction procedure because of TUS. Primary ureteroneocystostomy was performed in 23 patients, pyelovesicostomy in 8 patients, whereas the Boari flap technique was employed in 4 patients. At median follow-up of 36 months, no postoperative urine leaks or recurrence of strictures were reported.
In another study, 12 Kim and Buckley reported five robotic repairs of ureteral strictures, three patients underwent pyelovesicostomy, whereas two required ureteroneocystostomy. No postoperative complications were reported in the follow-up of 97 days.
Chen and Lee Zhao 14 have demonstrated the feasibility of TUS repair in three patients via single-port robotic procedure. Two patients underwent uretero-ureteral anastomosis, in which one patient had side-to-side anastomosis of transplant to the native ureter, whereas the other had end-to-side anastomosis. In one patient, ureteroneocystostomy was performed.
Benamran et al. reported a high open conversion rate of 40% for management of TUS utilizing the native ureter, citing fibrosis and scarring as the reason for the conversion. 11
In our series of 10 patients, various repair techniques were employed, tailored to the specific characteristics of each case. Ureteroneocystostomy, utilized in patients with distally located strictures, was used in five patients. Two of these patients required bladder hitch as an adjunct procedure to render the anastomosis tension-free. The Boari flap technique was employed in two patients with long-segment strictures and healthy bladder. These patients had undergone previous robotic ureterovesical anastomosis. The utilization of the native ureter for transplant ureter reconstruction has been reported in the literature with favorable outcomes. In their study, Hau et al. demonstrated comparable outcomes when he compared patients who underwent ureteroneocystostomy and those where the native ureter was utilized. 22
It has been our practice to ligate the ureter without performing native nephrectomy in patients with <500 cc urine output prior to transplant. A small subset of patients might develop flank pain and infection for whom native nephrectomy is indicated. 23 As mentioned earlier, selective patients could be selected for simultaneous native nephrectomy, and all patients must be counseled on the possibility of delayed native nephrectomy if needed.24,25 In their large series of 278 patients where the native ureter was ligated with no native nephrectomy, Gallentine and Wright reported six cases (2.2%) of delayed nephrectomy for flank pain despite including patients with >500 cc urine production per day. 13
The median length of stay after TUS repair was 2 days. At last follow-up, all patients were stent- and nephrostomy-free with imaging demonstrating absence of obstruction.
In conclusion, robotic repair of TUS is a technically feasible and a successful alternative to open procedure for definitive management of TUS. Besides being minimally invasive, we demonstrated the versatility of the robotic platform enabling different reconstruction options tailored to the patient’s needs. If the native ureter will be used for reconstruction, it is important to counsel patients on the possible need of simultaneous or delayed nephrectomy. Limitations of this study are the small sample size and the retrospective nature. However, this study adds to the growing body of literature confirming the viability and versatility of the robotic approach in managing TUS.
Authors’ Contributions
H.U.S.: Contributed to the conception, literature search, study design, and data collection. H.U.S., D.I., and K.R.: Contributed to the data analysis and interpretation. A.W. and Y.-C.L.: Designed and managed the qualitative analysis, project administration, and review. V.K. and M.E.: Contributed to the project design, conception, supervision, review, and editing.
Footnotes
Author Disclosure Statement
The authors of this article have no conflicts of interest to disclose.
Funding Information
There are no funders to report for this submission.
Data Availability Statement
Data are available for bona fide researchers from the corresponding author, M.E., upon reasonable request.