
Abstract

We write to describe our findings regarding the imaging used in studies reporting stone-free rates (SFRs) after retrograde intrarenal surgery (RIRS) following the Journal of Endourology 2023 announcement that non-contrast computed tomography (NCCT) with 2- or 3-mm cuts must be used to determine SFRs. The announcement specified that SFRs are divided into grades: Grade A has no stone fragments, Grade B includes fragments ≤2 mm, and Grade C contains 2.1–4 mm fragments; no timeframe for postoperative imaging was suggested. These criteria were created to standardize and improve the reliability of SFRs. 1 NCCT is the most sensitive method for detecting residual fragments (RFs) ≤5 mm but is often less favored in “real-world” practice compared with ultrasound and X-ray, which are cheaper, decrease radiation exposure, and are more readily available compared to NCCT. 2
We conducted a focused literature review to understand how the landscape of endourology research changed from the 6 months prior to the criteria adoption to a recent 6-month period. We searched major databases such as PubMed from 07/1/2022–12/31/2022 and 10/1/2024–4/1/2025 for studies reporting SFRs. In the prior period, 37% of studies used NCCT to determine SFR, compared with 57.9% more recently (Fig. 1). NCCT was used in 44.4% of randomized controlled trials, 30.0% of prospective studies, and 37.5% of retrospective studies before the announcement, compared to 60.0%, 57.1%, and 57.1%, respectively, recently. The odds of using NCCT were 2.34 times following the criteria from the Journal of Endourology (odds ratio = 2.34, 95% confidence interval = 0.85–6.43). These findings indicate an overall trend toward SFR standardization across all study types. Despite a lack of statistical significance, there is a growing consensus on the standard imaging for evaluating SFRs and its feasibility for implementation in endourology research.
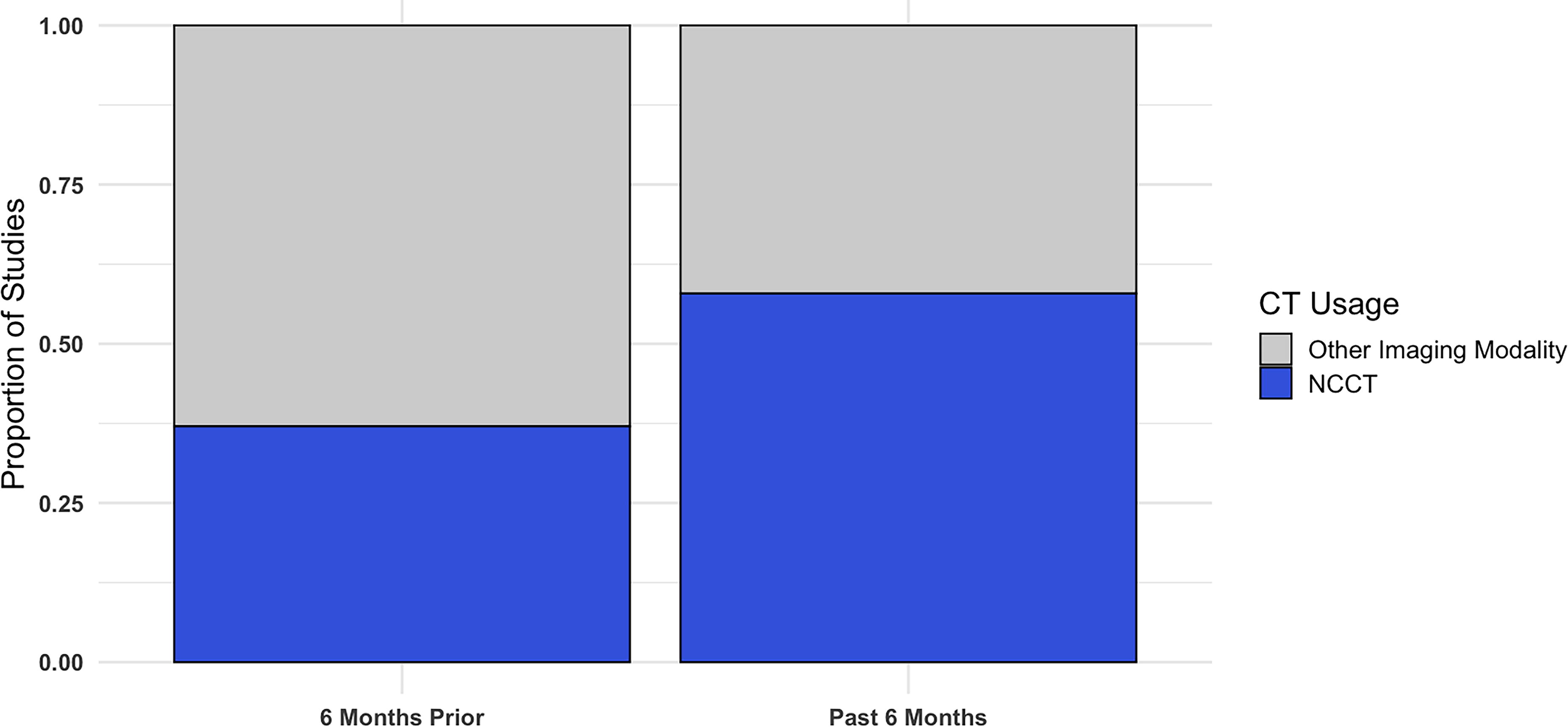
Proportion of studies using NCCT to report SFR in the 6 months before the Journal of Endourology’s criteria publication and in the most recent 6 months. NCCT, non-contrast computed tomography; CT, computed tomography; SFR, stone-free rate.
In addition to imaging modality, variations in RF definition and timing of postoperative NCCT remain additional elements that impact SFR standardization. A recent systematic review showed variability in definitions of RF across studies, ranging from <2 mm to <5 mm, alongside differences in postoperative imaging timing. 3 NCCT is the most sensitive method for detecting RFs; however, concerns regarding unnecessary radiation exposure suggest limiting the performance of NCCT to at least one postoperative scan. 2 American Urological Association guidelines do not provide specific recommendations regarding the type of postoperative imaging, the appropriate timing for postoperative imaging, or the definition of RFs, leaving the evaluation and decision for re-intervention to the surgeons’ discretion. 2,4 This lack of standardization across definitions of SFR thus creates difficulty in comparability across studies and assessing patient outcomes. 3
The results of this brief review and other recent systematic reviews further emphasize the need for standardized definitions and imaging protocols for postoperative urolithiasis management. We strongly feel the Journal’s decision to promote standardization and high-quality evidence when reporting SFR is valuable. Trends in study design appear to favor NCCT for SFR evaluation. Next steps include more widespread adoption of the Journal of Endourology’s comprehensive SFR criteria. Continued dialogue on this topic may help optimize SFR reporting to balance standardization with real-world practices.