
Abstract
Abstract
Objective:
The purpose of this project was to evaluate (a) the knowledge of Latina women who participated in an educational “Healthy at Home” intervention on environmental hazards in the home and (b) the effect of the program on clients' behavior regarding exposure to environmental hazards in the home.
Methods:
Data was collected using a cross-sectional survey administered at two points in time. Latina women participating in the “Healthy at Home” program were surveyed at the first home visit and six months following program completion. Maternity Care Coalition (MCC) in Philadelphia recruited 73 families via their MOMobile Program to participate in the “Healthy at Home” environmental outreach program. Participants included pregnant or newly parenting women from the Latina MOMobile in North Philadelphia.
Results:
On average, the women received high scores in all environmental content areas. Results showed significant increases related to asthma and lead knowledge along with significant behavioral changes related to environmental pests (P = .05), effective cleaning techniques (P = .048), and using cold water for cooking to reduce lead exposure (P = .001).
Conclusions:
Future research should be conducted to (a) better understand the links between knowledge and behavior change in Latino populations; (b) better tailor health education messages for this population; (c) capitalize upon the potential social capital within the Latino community to reach out to pregnant, low-income, urban women; and (d) make environmental justice issues more visible among those working in public health and public policy.
Background
Minority groups are disproportionately exposed to a number of environmental toxins, and consequently suffer related health consequences unequally. Latinos, in particular, encounter more environmental hazards than Caucasians, such as garbage dumps or factories in their neighborhoods, and have a greater indoor exposure to asthma triggers, lead poisoning, secondhand smoke, mold, dangerous cleaning chemicals, and pesticides.2–4 The Latino population in southeastern Pennsylvania is no exception.
In 2007 there were approximately half a million Latinos living in Pennsylvania compared with greater than 10 million Caucasians living in the same region. 5 That same year, of the 187,112 pregnant women in Pennsylvania, Latinas had the largest number of pregnancies at a rate of 121.5 per 1,000 of its population in contrast to a rate of 62.6 per 1,000 in the Caucasian population.6–7 This figure does not include any of the estimated 11.9 million undocumented immigrants thought to be living in the United States. 8
Poverty and environmental inequity are closely associated. In 2008, 13.2% of the United States population 9 and an estimated 19% of Philadelphia, Pennsylvania residents 10 were living below the poverty level. Latino children are particularly at risk for living in poverty. In 2008, almost one third (30.6%) of all Latino children under eighteen in the United States lived below the poverty level 9 while 35% of the Latino children in Pennsylvania were classified as poor. 11 They have no voice of their own so they must rely on their parents to represent them in reducing their exposure to indoor health hazards. Parents accomplish this through their appeal for environmental health programs and new environmental laws or policies. However, a lack of English proficiency 12 and limited access to health care 13 may limit their ability to make an impact.
Lead poisoning is an environmentally acquired condition and it can occur from many sources including lead paint, soil, water, and the workplace. Latino children are twice as likely as Caucasian children to have blood lead levels above 10 μg/dL, a level known to negatively affect a child's health. 14 One tenth of all Latino children in the United States have received this diagnosis.
While the American Lung Association of Minnesota 15 found a connection between asthma and genetic factors, evidence shows that environmental factors play a strong role in the onset of asthma.16–18 The Centers for Disease Control and Prevention (CDC) found that while asthma rates were comparable for Caucasian children and Latino children (8% and 9%, respectively), nearly 20% of Puerto Rican children under the age of eighteen had asthma. 21 Puerto Rican children are also twice as likely to be diagnosed with asthma as Caucasian children. Asthma attacks may occur in children when there is exposure to indoor asthma triggers (i.e., mold, dust mites, second-hand smoke, pest problems, and dangerous cleaning chemicals).
Environmental justice is the fair treatment and involvement of all people regarding the development, implementation, and enforcement of environmental laws and policies. 19 In 1994, former President Clinton enacted an executive order to bring environmental justice to minority and low-income groups. Under this order, all federal agencies were mandated to allow both minority and low-income groups a chance to be involved in public and environmental health issues, as well as to make public information pertaining to environmental health readily available to them. The executive order marked clear progress toward the reduction of environmental health hazards among community groups. 20
Significance of healthy homes projects
Several Healthy Homes programs proved effective at alleviating illness related to indoor environmental health issues. The Asthma: Putting on AIRS project in Connecticut reduced dust, humidity, and secondhand smoke levels in the home. Unscheduled asthma-related doctor visits were reduced by nearly 75%, and asthma-related ER visits by 30%. The Southern Rhode Island Area Health Education Center's Healthy Residents, Healthy Homes project also decreased asthma and indoor environmental health issues. Mold was reduced by 12% and pest problems by 3% inside the home, and child reports of asthma symptoms dropped by 11%. 21 The Community Lead Outreach Program by the Sixteenth Street Community Health Center in Milwaukee, Wisconsin also saw positive results. The percentage of children with blood lead levels greater than 10 micrograms/dL fell from 46% to 22% over the course of its study. 22
The purpose of this project was to evaluate (a) the knowledge of Latina women who participated in an educational “Healthy at Home” intervention on environmental hazards in the home and (b) the effect of the program on clients' behavior regarding exposure to home-based environmental hazards.
Maternity Care Coalition
Maternity Care Coalition (MCC) is a private non-profit organization in Philadelphia that works with individuals, families, health care providers, and the community to improve maternal and child health and well-being. Maternity Care Coalition's signature program is the MOMobile
Methods
Data was collected using a cross-sectional survey administered at two points in time. Latina women participating in the “Healthy at Home” program were surveyed at the first home visit (the “bucket visit”) by community health workers and six months following program completion. MCC recruited 73 families via their MOMobile program to participate in the “Healthy at Home” environmental outreach program. Participants included pregnant or newly parenting women from the Latina MOMobile in North Philadelphia referred to MCC through street outreach, community agencies, health care institutions, and former clients. Informed consent was signed in either English or Spanish at the time of the first home visit. The MCC Research Review Committee and the Internal Review Board at Arcadia University approved the study.
Questionnaires were designed to collect information on the women's knowledge of the four topic areas of intervention—asthma, lead poisoning, tobacco smoke pollution, and dangerous household cleaning products. Data was organized to assess (a) the extent to which the identified environmental hazard was a problem in that home, (b) knowledge of and attitudes toward each of the hazards, and (c) changes in behavior taken to mitigate the effect of each hazard in the home. The questionnaires were translated into Spanish and were administered by the Latina MOMobile Advocates during a home visit. All of the questions for the pre- and post-tests were pre-screened by public health professionals for content validity and Advocates were trained on interviewing techniques and the delivery of each question.
MCC Advocates associated with the Latina MOMobile received training on asthma education and prevention, including integrated pest management, lead poisoning prevention, nicotine and tobacco smoke pollution, and household product safety. Following training, Advocates scheduled a “Healthy at Home” visit with each new MOMobile client and administered the pre-test. The Advocate conducted a simple hazards assessment, selected and reviewed educational materials with each woman regarding the particular hazards found in their home, and gave each client a bucket of gifts, including non-toxic cleaning supplies and impermeable pillow covers. A post-test was administered during a follow-up visit approximately six months after their initial home visit.
Results
Results from the 73 clients who completed the pre-test showed that the majority were Latina (n = 64, 88%) with a median age of 22. Twenty clients (27%) were pregnant with their first child. Most (n = 50, 68%) rented their homes and 68 of the homes (95%) pre-dated the ban on lead in residential paint manufacture. Additionally, over half of the women (28, 58%) reported at least one smoker in the household (Table 1).
The home visits included a referral component so that immediate action could be taken when necessary. Following the initial home visit, 10 (13%) referrals were made to the Asthma Call Center (an asthma clearinghouse and continuity-of-care center managed by the Health Promotion Council of Philadelphia); 14 (19%) to pediatricians for lead testing of child blood lead levels; and 13 (18%) to the City of Philadelphia's Childhood Lead Poisoning Prevention Program for lead testing in the home.
Forty-nine clients completed the post-test for a 67% retention rate. Six month follow-up data showed that 24 clients (49%) responded yes to being asked if anyone in the home had ever been diagnosed with asthma while 7 (14%) reported that their child had been to an emergency room within the past six months because of asthma (Table 2).
Knowledge scores revealed a high level of baseline knowledge in each content area (Figure 1). On average, the women received approximately 80% for both the pre- and post-test asthma sections. They received a slightly lower score with a mean of 71% for the pre- and post-test lead poisoning sections. Smoking appeared to have the highest mean scores reaching 81% with the pre-test but slightly decreasing to 78% with the post-test. Finally, the women's mean scores on their knowledge of dangerous cleaning chemicals shifted from 74% in the pre-test to 77% in the post-test. Since the women achieved high scores on the initial pre-test, they may have already been aware of some of the hazards associated with each indoor environmental health issue.
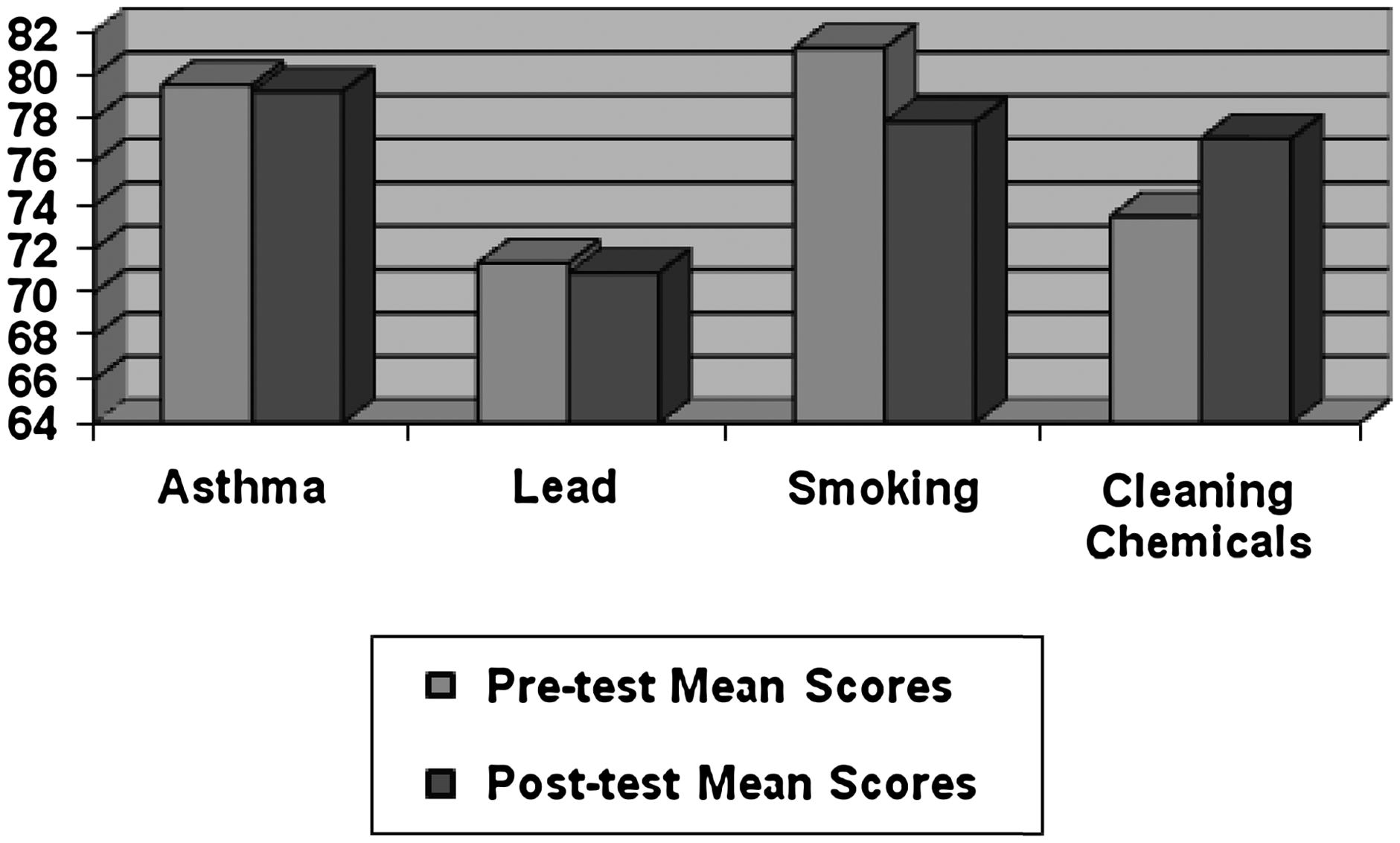
Healthy at Home Pre-test and Post-test Knowledge Mean Scores for Asthma, Lead Poisoning, Smoking, and Dangerous Cleaning Chemicals.
Wilcoxon tests were conducted to evaluate changes in knowledge in the four content areas (asthma, lead poisoning, household cleaning chemical use, and smoking) and behaviors related to the educational intervention. Significant changes were seen in knowledge and behaviors regarding asthma and lead (Table 3).
Discussion
The MCC “Healthy at Home” intervention tested the efficacy of an educational and behavioral intervention related to asthma, tobacco smoke pollution, dangerous cleaning chemicals, and lead poisoning. Information retention levels for asthma and lead poisoning significantly increased from the pre-test to post-test. This suggests the education the women received improved their understanding regarding (a) the relationship between Vitamin C and asthma, (b) food sources of Vitamin C, (c) the ease of tracking lead into the house from the yard, and (d) the mechanism by which lead is absorbed in the stomach. Vitamin C has proven effective at reducing asthma symptoms while increasing lung function.23–24 Additionally, as many as 96% of asthma sufferers in one study were found to be deficient in Vitamin C, 25 and in another study 26 the deficiency was considered a risk factor for asthma. Additional studies have educated parents regarding sources of lead poisoning and how exposure to and intake of lead can be reduced.27–30
Behavior changes among program participants were also seen for several indoor environmental health factors in this study (taking measures to eliminate pests, dusting with damp cloths, and cooking with cold water). The EPA 31 determined that fewer than thirty percent of individuals with asthma take the necessary steps to reduce asthma triggers. Numerous studies in the past have focused on eliminating just one asthma trigger or lead exposure.32–36 These significant findings support the necessity for more programs like MCC's “Healthy at Home” educational intervention with an emphasis on reducing multiple asthma triggers and lead exposure at the same time.
Overall, the increased knowledge and behavioral changes that women in MCC's “Healthy at Home” program made were similar to those made by parents of inner-city African-American and Latino youth who participated in one of two programs conducted by the National Cooperative Inner City Study (NCICS) 37 and the Seattle-King County Healthy Homes Project. 20 The children in both of these programs were already diagnosed with asthma and placed in a control or intervention group in one study, or a low or high intensity intervention group in the second study. Their caretakers were educated about several indoor asthma triggers (cockroaches, dust mites, cigarette smoke) and given supplies. With the increased knowledge, the caretakers became more proactive and decreased asthma triggers, which in turn lowered asthma-related illness and hospitalization. MCC's “Healthy at Home” program was designed for both families with children who had asthma and lead poisoning and those who were at risk for acquiring them. The goal was to reduce the exposure early thus preventing the development of asthma and lead poisoning.
Cooking with cold water to reduce lead exposure, eliminating pests, and dusting with a damp cloth were noteworthy behavior changes. Cold water cooking has lower lead levels than hot water and is recommended by several government organizations.38–39 These behaviors represent simple cost-effective changes that constitute a high return on investment through an educational intervention.
Other programs have used help from outside sources to effect change. The Lead + Asthma Project 40 is a similar program that provides education for parents and gives a hazard assessment along with an indoor environmental hazard intervention such as plumbing repair, ventilation improvement, and asthma trigger reduction techniques. Cost effectiveness needs to be considered when reaching out to a larger population since it may be difficult to implement behavior changes with financial implications for low-income populations. 41
Limitations
Although information retention levels for asthma and lead poisoning significantly increased from the pre-test to post-test, factors may have played a role in limiting the amount of information conveyed. These include the comprehensiveness of the curriculum provided by the program and distractions while taking the post-test due to child care responsibilities. Additionally, interviewer bias could have had an impact on the results of the post-test. Although Advocates participated in training regarding interviewer techniques and delivery of questions, Advocates would restate a question when necessary so that participants fully understood its meaning. Misunderstanding the meaning of a question may have caused variation in test responses. Even though the Advocates previously visited the women on home visits, some women were initially skeptical of the interview questions and what was required of them. However, the interview process was thoroughly explained to all of the women beforehand and they were reassured that there would be no identifying information linking them to their interview responses.
Public Health Implications
The importance of social capital among minority communities, specifically the role of trust and social networks, has been discussed in the literature. 42 The level of trust Latina women have in their doctors, police, political leaders, and community affect whether they seek medical care or trust government and community programs designed specifically for them. It is important to use neighborhood-based health educators since they can better relate and empathize with the women seeking care and are able to speak their language. Understanding different levels of trust may help explain how willing Latina women are to take a risk and follow the advice given by the Advocates along with their perception of environmental justice within their community. Once positive behavior changes are made by the mothers and results observed, lifelong behaviors can be established. The role of lay health community workers or Advocates is significant and can lay the foundation for positive behavior change through a bond of trust. 43
Future research should be conducted to (a) better understand the links between knowledge and behavior change in Latino populations; (b) better tailor health education messages for this population; (c) capitalize upon the potential social capital within the Latino community to reach out to isolated groups, such as pregnant, low-income, urban women; and (d) make environmental justice issues more visible among those working in public health and public policy.
Results suggest that an in-home educational intervention with a demonstration of effective techniques may be one of the easiest ways to improve Latina women's indoor environmental health because the intervention is simple and feasible for low-income households. By addressing healthy housing and protection from indoor environmental hazards, we enable individuals living in high-risk surroundings to move one step closer to environmental justice.
Footnotes
Acknowledgments
We would like to acknowledge Maternity Care Coalition and the Research Committee who assisted in the development of the survey tool. We are grateful to the Latina MOMobile staff, including Maria Rosa, Jenny Perez, and Carmen Geraldo (Latina Advocates) who administered the questionnaires, did follow-up to collect data, provided help throughout the study and reviewed the Spanish-English questionnaires. We want to acknowledge the Latina MOMobile clients who graciously invited us into their homes to provide “Healthy Home” education, evaluate the impact of the education, and take part in interviews pertaining to environmental justice. Finally, we wish to thank the Office of Minority Health of the U.S. Department of Health and Human Services for their funding in this project.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.