
Abstract
Abstract
The purpose of this article is to examine the relationship between environmental changes and infectious diseases and their impact on health in environmental justice (EJ) communities. The evolution of EJ science and research is contingent upon an integrated approach that takes into account social processes and environmental changes to address the burden of infectious diseases in EJ communities. We recognize that infectious disease and environmental justice is novel and calls for more research in this area, especially as the focus of public health shifts towards an ecologic and social approach to disease prevention. We attempt to explore in further detail how environmental changes such as urbanization, agriculture, and climate variability could potentially influence pathogen dynamics, vector transmission, host susceptibility, and disease outcomes among environmental justice populations.
Introduction
The relationship between the environment and infectious disease can be traced to the origins of the miasma theory. 2 This theory postulated that “bad, toxic or noxious air,” identifiable by its foul smell, was essentially the cause of disease. It posited that a preventive approach characterized by improved drainage and sewage practices and better sanitation could guard against the transmission or contraction of disease. This theory was subsequently disproved and supplanted by the germ theory, one that postulated that bacteria and viruses, not the foul-smelling air, were culpable in the contraction and transmission of infectious disease.3,4
The germ theory, advocated by traditional environmental health emphasizes a causal approach to disease, and neglects the role the social environment and its determinants play in contributing to infectious disease prevalence. 5 Thus, very little research has focused on the synergies between environmental health and population and individual level social determinants and their influence on infectious disease despite the fact that they (social determinants) drive exposure to environmental hazards and influence health outcomes.6–12
Since the publication of the Toxic Wastes and Race in the United States report, 13 the environmental justice (EJ) movement has drawn attention to the interplay of differential exposure to environmental hazards and social determinants on health outcomes with a wealth of literature demonstrating these relationships especially among EJ communities.14–20 For example, several studies have provided evidence for the role that environmental hazards and social determinants play in driving disparities in cardiovascular disease,22,23 asthma,24–27 congenital anomalies,28–32 diabetes,33,34 and infant mortality35,36 in EJ communities. In spite of the established associations between environmental hazards and social determinants on these health outcomes, little work has been performed to examine similar relationships between these processes and infectious diseases in EJ communities.
Against this backdrop, this article aims to highlight the contribution of social determinants to the prevalence of infectious diseases in EJ communities. We define social determinants as the description of the conditions and environment in which people are born, grow, live, work, and age, including policies, all of which are shaped by the distribution of resources, wealth, and power. 37 We also describe EJ in the context of Global North and Global South populations and define it as not just the equitable development, implementation, and enforcement of environmental policies and ordinances without prejudice, but includes the social transformation of the environment that is aimed at meeting basic human needs and enhancing the overall quality of life.13,38 After much consideration, we suggest an integrated approach, one that takes into account social determinants and environmental changes in addressing the burden of infectious diseases in EJ communities, an important step in the evolution of EJ science and research.
Discussion
Divergence between environmental health and infectious disease epidemiology
Originally intertwined, environmental health and infectious disease science have over the years been studied separately. 39 This separation was due, in part, to the influence of the conservation movement on environmental health following the publication of Rachel Carson's book, Silent Spring, which brought attention to the negative impacts of pesticide use on the environment. 40 The aftermath of this resulted in the establishment of the Environmental Protection Agency (EPA) with the mission of enforcing environmental protection, conducting environmental research, combating environmental pollution, and recommending environmental protection policies. 41
Before the establishment of the EPA, the United States Public Health Service (USPHS) originally oversaw both environmental health programs and infectious disease outbreaks through interventions that focused on sanitation, water and air quality, sewage disposal, and housing.39,42 These interventions utilized a holistic approach to infectious disease, recognizing the role of the environment in facilitating host susceptibility and pathogen exposure in causing infections. However, after the creation of the EPA, the focus of environmental health shifted to toxicology, the effect of chemical agents on human health, and animal and plant life. It viewed infectious disease causatively, from a germ theory perspective, emphasizing individual risk, drug therapy, vaccines, and pesticides with limited attention to the impact of social determinants on disease dynamics. This divergence subsequently led to reductionist approaches in addressing the burden of infectious disease 6 with disadvantaged populations being disparately impacted. 43
Environment and disease
There is significant evidence that illustrates the intricate and synergistic relationship between the environment and infectious disease morbidity, a relationship often perpetuated by environmental changes that drive emerging and re-emerging pathogens.45–49 The environment consists of various risk factors for disease, namely, social, natural, physical, chemical, and biological. 50 The environment's complex link with disease has best been demonstrated in a risk assessment conducted by WHO which found that an estimated 24% of the global disease burden (healthy life years lost) and 23% of all deaths (premature mortality) are attributable to environmental factors. 51 Figure 1 illustrates a diversity of diseases as well as the degree of contribution by environmental factors to their prevalence. 51 Diarrheal diseases had approximately 94% of its disease burden attributable to the environment, 51 thus highlighting how the environment significantly impacts disease.

Diseases with the largest environmental contribution. aLead-caused mental retardation is defined in the World Health Organization list of diseases for 2002, accessed at
In order to comprehend the influence of the environment on disease, various approaches have been proposed including eco-social, 52 eco-epidemiology,53,54 and social-ecologic systems. 55 These approaches have all been used in the field of infectious disease epidemiology to provide a framework for epidemiologic research. Several studies have been able to demonstrate the intricate relationship between environmental changes and pathogens.5–7,10–12 They suggest that environmental changes trigger a shift in social, physical, chemical, structural, and ecological factors that could: 1) affect the dynamics of pathogen transmission, 2) increase virulence of pathogens, 3) increase host susceptibility to pathogens via immune compromise, and 4) lead to the mutation of new resistant pathogenic strains.
The consequences of this could potentially increase infectious disease burden and worsen health outcomes, particularly in disadvantaged communities that already have a comparatively elevated disease burden. For example, environmental changes that increase chemical exposure may negatively impact the quality of life, alter climate patterns, overburden a community with industrial and toxic pollutants, or change demographic patterns via migration. Such changes may weaken immune defenses, lead to pathogen mutation or re-emergence, and alter the severity of disease outcomes.7,11,12,56
Though the environment's role in disease transmission has been recognized by the epidemiologic triad, there is still some disconnect as to how environmental variability impacts infectious disease processes. 6 Commonly identified environmental changes that mitigate disease transmission include urbanization, antibiotic abuse, agriculture practices, deforestation, transportation projects, natural disasters, and climate change,5–8,10–12 illustrated by Figure 2. 6 Urbanization can lead to modifications in migration patterns that create densely populated urban centers, which ultimately disrupt ecosystems and natural resources and contribute to the transmission of infectious diseases.6,7,45,46,49 Current practices of high antibiotic use in agriculture may also be detrimental to human health. Microbes have the ability to adapt which increases opportunities for the production of antibiotic resistant strains of bacteria and drug-resistant parasites.6,11 The growth of the agriculture industry and evolving practices of crop and animal management, including fertilizer and biocide use, and use of genetically modified organisms has created new opportunities for Escherichia coli related diseases to occur. 6 Irrigation practices reduce water availability for other uses and increase breeding sites for disease vectors. 45 Deforestation serves as a catalyst to promote pathogen-vector-host interaction as the boundary between human and animal habitats becomes less distinguishable. 49 Advances in the transportation industry, such as construction of new roads and modern air travel, have served as a mechanism to mobilize diseases to some of the most remote regions of the world.6,45 Climatic changes alter the environment in such a way that it produces extreme weather events and disrupts ecosystems, allowing infectious diseases to spread across multiple geographies.6,7,10,12,56
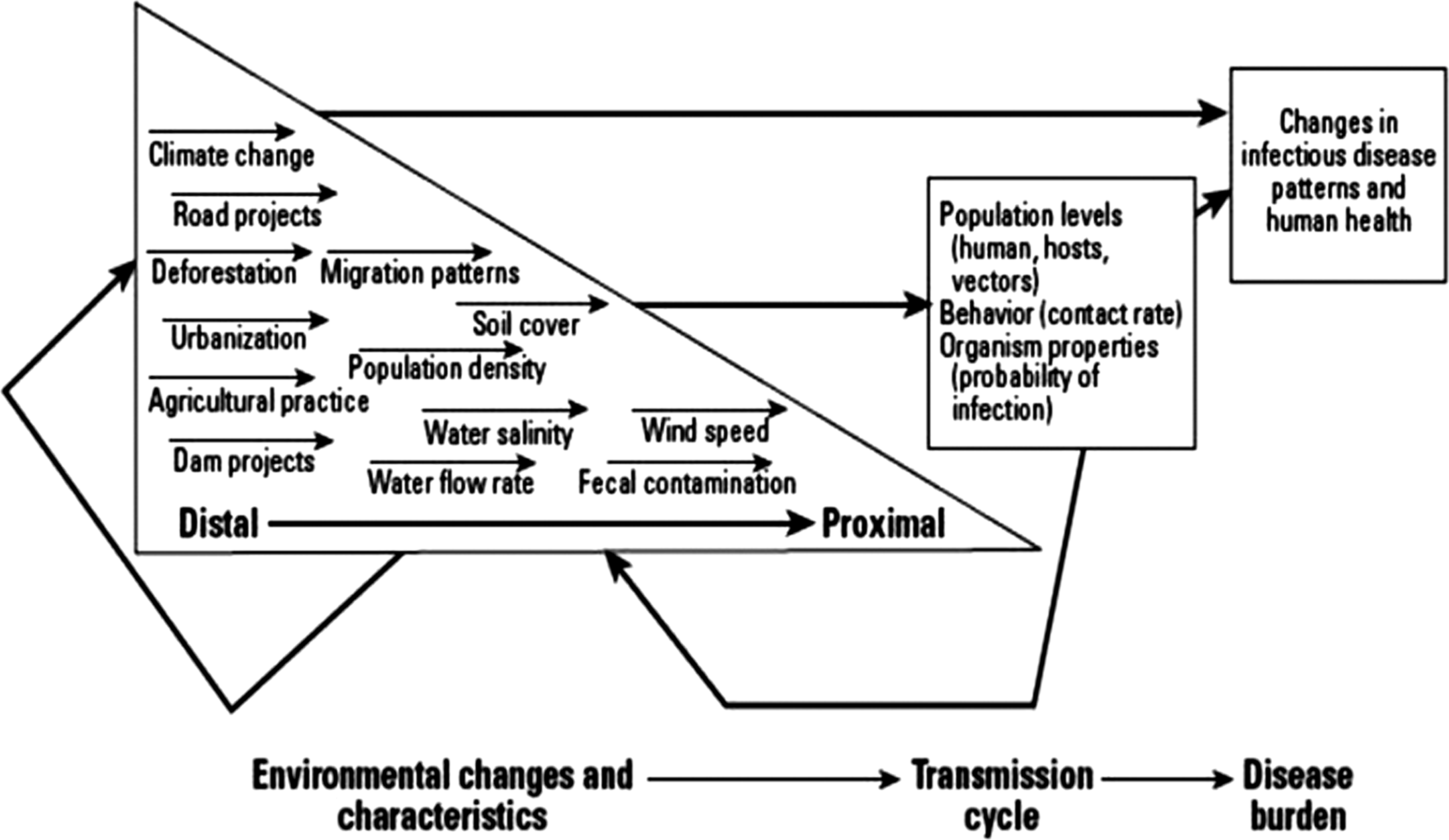
Environmental determinants of infectious disease (EnvID) framework.
Environmental justice, vulnerability, and disadvantaged populations
Even with recent advances in understanding the contribution of environmental factors to the prevalence of infectious disease, little work has been done to critically examine the role that environmental injustice, vulnerability, and disadvantage play in the prevalence of infectious diseases in at-risk and underserved populations.
Cassel (1976), in his work, recognized the role of vulnerability in the onset of infectious disease particularly among disadvantaged populations. 57 He described vulnerabilities as those factors that can increase host susceptibility to an infectious agent, thus resulting in clinical disease or worsening clinical disease as an outcome. Cassel further contends that the social environment is complicit in compromising host resistance and he identifies marginal status in society, social disorganization, and dominance hierarchies as factors responsible for the disparate burden of disease borne by underserved and disadvantaged populations. These factors also known as vulnerabilities have become crucial in influencing disease outcomes, nowhere more than in EJ communities.
In EJ communities, vulnerability factors include characteristics, individual level and/or community level, that moderate the effect of environmental hazards on the community with attendant health impacts. Prior work has shown that disadvantaged and vulnerable populations reside in communities that are disproportionately exposed to chemical and social stressors that contribute to poor environmental quality and environmental health disparities.14–21,58–61 The combination of chemical and social stressors lead to the production of high risk settings classified as riskscapes58–60 or unhealthy community ecosystems 21 characterized by infrastructure disparities,62–65 unhealthy land uses,14,17, 19,58,60,66,67 inequities in planning and zoning,68,69 neighborhood poverty,14,70 and residential overcrowding.14,70 Chronic exposure to these stressors increases allostatic load which leads to organ wear and tear, hypertension, and compromised immune function characterized by an impaired ability to repel pathogens.14,71 For example, a study revealed increased rates of respiratory infections among individuals with higher self-rated levels of stress despite controlling for allergies and other factors. 72 In addition, chemical stressors in the form of environmental pollutants have been known to have direct noxious effects on human health, particularly the immune system via compromising host defenses against infectious agents. 73 In concert, these stressors increase the vulnerability of a population to negative health outcomes. Cumulatively, the impact of these stressors leads to negative health consequences for EJ populations.71,72
Environmental justice, social environment, and infectious disease
Yen and Syme describe the social environment as the neighborhoods in which we live, our workplaces, and the policies we create to order our lives. 38 The importance of the social environment to health cannot be over-emphasized as it can influence health outcomes independent of individual risk factors. 38
Besides disproportionately hosting pollution-intensive facilities, studies have shown that the social environment in communities impacted by environmental injustice is characterized by poverty,16,19 segregation,20,59 and an overall poor quality of the environment.60,66 The quality of the environment is related to the rule of law, ordinances, and characteristics of the physical environment. 38 In EJ communities, the social environment is characterized by crime, 14 violence, 74 disregard of environmental policies and ordinances, 14 failing water and sewage facilities,75,76 proximity to polluted air and water sources, 70 economic disinvestment, 77 and poor living conditions; 11 all factors known to drive negative health outcomes and disease dynamics.14,18,20
In consonance with underlying vulnerabilities, an unhealthy social environment and environmental injustice have contributed to the resurgence of infectious disease which may disproportionately affect low-income and disadvantaged persons. For example, dilapidated housing conditions present in EJ communities are a source of mold and mildew and harbor vectors such as rats and cockroaches that transmit pathogens,78,79 while poor living conditions provide conducive conditions for the transmission of tuberculosis and other respiratory infections.80,81
Disparities also exist in the availability of safe water and sewer services to poor EJ neighborhoods because of a failure to install up-to-code sewer and water infrastructure, which result in polluted water supplies with an increased fecal microbial load.75,76,82,83 Additionally, sewage and leachate from landfills, disproportionately sited in EJ communities, potentially provide a source for enteric pathogens resulting in diarrheal diseases. 84 Furthermore, inequitable land planning and development and local environmental health policies also play a role as some studies have shown that underserved residents in EJ communities access and utilize water supplies not in compliance with environmental laws and safe standards for drinking.75,76,82,83
These disparities in the social environment can mediate the transmission, incidence, and prevalence of pathogens. Table 1 illustrates the distribution of waterborne-disease outbreaks in the United States associated with drinking water by etiologic agent and type of water source for 2005–2006. 85 All 518 cases of waterborne-disease were due to contaminated ground water and surface water which demonstrates how poor water and sewer infrastructure can allow populations to become more vulnerable to waterborne-diseases.
WBDOs with deficiencies 1–4 and 13 (i.e., surface water contamination, ground water contamination, water treatment deficiency, distribution system contamination, and untreated chemical contamination of water source) were used for analysis.
Multiple etiologic agent types (bacteria, parasite, virus, and/or chemical/toxin) identified.
Norovirus suspected based on incubation period, symptoms, and duration of illness.
From the aforementioned, it is clear that the twin burdens of poor social conditions and environmental hazards, characteristic of EJ communities, play a role in influencing pathogen transmission, pathogen virulence, as well as host susceptibility and response to pathogens. In the following sections, we will attempt to elucidate the effects of urbanization, agriculture, and climate change, all implicated in infectious agent transmission, on the burden of infectious disease in EJ populations and communities.
Urbanization
Urbanization, defined as a process that involves an increase in number of people and the emergence of cities,86,87 has been identified as one of the most important environmental factors influencing the emergence of infectious diseases. 88 The urbanization process is accompanied by factors such as economic segregation, 89 industrialization,86,90 environmental hazards and pollution, 86 and population mobility86,90 with disadvantaged populations most likely to face the brunt of this differential burden. 86 Economic segregation facilitated by urbanization, leads to concentration of disadvantage and poverty within communities that manifest as infrastructure disparities and economic blight, characteristics that may be associated with sanitation and have been shown to be influential in infectious disease transmission.
As alluded to earlier, residential overcrowding and deteriorating housing conditions, a feature associated with urbanization, has been associated with respiratory infections and the re-emergence of mycobacterium tuberculi in the U.S., the pathogen that causes tuberculosis while mycotoxins released by mold can cause respiratory infections.78,79 Also, vectors such as rats and cockroaches, prevalent in these neighborhoods, are known to be both mechanical and biological carriers of pathogens that can cause numerous infectious diseases including salmonella,91,92 lassa fever,93,94 and leptospirosis.95,96
In the same vein, poor sanitary conditions associated with urbanization have led to an increased incidence of water-borne enteric pathogens.6,49 Contamination of these water sources provides a conduit for the transmission of enteric pathogens such as salmonella typhi, Escherischia coli, giardia lamblia, cholera vibrio, cryptosporidium, and ascaris lumbricoides. 97 Similarly, solid waste from landfills, air pollutants from heavy traffic, and toxic chemical facilities in close proximity to these communities have been known to contaminate water supplies and air, providing sources of gastro-intestinal and respiratory infectious diseases respectively.70,98
Another impact of urbanization is encroachment into wildlife habitats, eliminating the edge effect, and inadvertently increasing the frequency of man's contact with wildlife. This increased exposure facilitates the transmission of zoonotic infections with deleterious health consequences. 45 For example, Borrelia burgdorferi, the pathogen causing Lyme disease, is transmitted by a tick found on wild deer and was contracted by humans as a result of increased frequency of contact between animals and humas. 99 Since the first case was identified, Lyme disease has become the most important arthropod-borne disease 100 and has been known to result in cardiac abnormalities, 101 arthritis, and paralysis. 102 Another example illustrating the elimination of the edge effect and increased frequency of contact with wildlife is the location of piggeries close to the forest which facilitated the transmission of the Nipah virus to low-income employees and pig farmers from fruit bats in Malaysia.46,103 These two processes represent a disruption of the ecosystem and as a result, differentially expose disadvantaged and low-income populations to these pathogens. 104
Finally, a less discussed concept in examining the social determinants of health and urbanization emphasizes the types and characteristics of social relationships/networks among people within a community and how they influence disease outcomes. They include social capital and collective efficacy and have been known to significantly influence health.105,106
Social capital has been defined as the features of an organization such as civic participation, norms of reciprocity, and trust in others that facilitate cooperation for mutual benefit105,107 while collective efficacy is defined as mutual trust and willingness to intervene for the common good. 108 Communities with high levels of collective efficacy and social capital reflect strong ties among members and minimal internal conflict. In concert, they act to buffer communities from external stressors and insults, which EJ communities are prone to, and create an ambience of empowerment within these communities. Furthermore, communities with high levels of collective efficacy and social capital also have an increased ability for collective action to control and order their environment as well as protect themselves from environmental hazards and community infrastructure dilapidation. 109
However with urbanization and its attendant migratory flux and concentrated poverty, social capital and collective efficacy decline, leading to disempowerment of EJ communities.110,111 This disempowerment occurs at the community and individual levels and facilitates the promotion and acceptance of maladaptive behaviors and infrastructure decline. In addition, disempowered communities may be unable to resist the disproportionate hosting of toxic waste facilities in their neighborhood and become disproportionately exposed to these facilities and their chemical emissions. 109 Ultimately the effects of these processes contribute to providing a prime milieu for the proliferation and transmission of pathogens.
Agriculture
The influence that the environment has on the emergence and resurgence of infectious disease is facilitated through multiple transmission systems between human-hosts, agents, and the environment. 6 Increases in agricultural development have narrowed the gap between human-hosts, agents, and environmental interactions. For example, the rise of concentrated animal feeding operations (CAFOs) has created ideal conditions for the spread of infectious diseases. The movement towards CAFOs has allowed farmers to achieve economies of scale by raising livestock in confinement at high densities with minimal land use. 112 A major problem surrounding overcrowded swine facilities is that the surplus of animals creates sizeable amounts of wastes composed of pathogenic microbes and nitrates. 112 Although farmers mostly rely on lagoons to store and treat animal wastes, potential contamination of water sources may occur if the lagoon breaks or wastewater seeps into surrounding soil or ground water. 112 Human exposure to these contaminants may result in the transmission of Erysiopelotthrix rhusiopathiae, Yersinia enterocolitica, Salmonella, Streptococcus suis, hepatitis E virus, Leptospira, Brucella, and influenza virus. 112
Studies conducted in North Carolina found that communities most disproportionately burdened by swine CAFO and related hazards were low-income, economically distressed, and disadvantaged areas heavily dependent on groundwater.113,114 These vulnerable communities near swine CAFOs were equally burdened by airborne emissions from confinement houses, waste lagoons, and spray fields that contain ammonia, hydrogen sulfide, volatile organic compounds (VOCs), dusts, and endotoxins.113,114 Airborne emissions may cause respiratory dysfunction, negatively affect quality of life, and inhibit immune function which makes these populations especially vulnerable to disease.113,114 Moreover, disease burden may be intensified in these communities due to their low wages, lack of access to medical care, and poor nutritional options.113,114 A study on the Mississippi swine industry also showed that industrial swine operations were more concentrated in low-income counties with high proportions of racial and ethnic minorities. 115
Antimicrobial agents found in animal waste may be used therapeutically to decrease the spread of infectious disease between animals, but are often used non-therapeutically to promote growth and improve feed conversion ratios. 116 The use of low dose antibiotics for prolonged intervals may actually foster resistance because instead of the bacteria being killed it selects for more resistant strains. 116 Exposure to antibiotic resistant organisms such as Cyclospora, Escherichia coli, Salmonella, Campylobacter, Enterococcus, and Staphylococcus is disconcerting because there may be no effective treatments to combat these infections. Without effective treatments to combat infection, having a healthy immune system can be the difference between life and death after exposure to infectious disease agents.
Bioaerosols, particles that contain endotoxins, bacteria, and fungi, are also found in swine facilities and are known to produce significant adverse respiratory health effects in swine CAFO workers. 112 A study conducted by G. Ko et al. found that the mean concentration of endotoxins released from swine CAFOs downwind were much higher than those released upwind, which has adverse health effects on neighboring communities. 117 Moreover, excessive amounts of nitrates found in animal wastes at CAFOs seep into groundwater and may cause reproductive health effects such as central nervous system developmental defects and miscarriages. 112 The populations that are disproportionately exposed to these environmental hazards are low-income and minorities who reside near the CAFOs and individuals that are heavily dependent on groundwater increasing their risk of exposure to infectious disease agents.
The environmental impact of CAFOs has social ramifications as well. These communities possess limited political and economic resources to mitigate the problem, and become victims of dominant racial and class hierarchies.112–115 This leads to a concentration of disadvantage and environmental risks. Furthermore, the potential health impacts related to CAFOs become more alarming when one considers that these communities represent foci for poverty, decaying or absent infrastructure and services, wide-ranging vulnerabilities, and co-morbidities.
As humans continue to rely heavily on the agricultural industry, the need to address how modern farming methods impact health has become more apparent. Due to differential burden and exposure of some racial/ethnic and class populations to pollution that stems from farming practices, researchers would be remiss not to focus on the environmental injustice component. Addressing social conditions will become increasingly important in minimizing disease transmission and eliminating health disparities in communities that host agricultural operations.
Climate change
The Intergovernmental Panel on Climate Change (IPCC) reports that human activities such as the combustion of fossil fuels and rapid deforestation have triggered climate change. 118 The impact of climate change on health has also been documented. 119 Specific to infectious diseases, climatic changes will adversely affect the incidence, transmission patterns, and geographic range of vector-borne diseases such as malaria, dengue fever, yellow fever, viral encephalitis, schistosomiasis, leishmaniasis, Lyme disease, and onchoceriasis. 119 The impact of climate change on disease burden is largely dependent upon social, economic, and environmental factors that will have regional variations, allowing some populations to be more vulnerable to disease than others.120,121
The IPCC predicts that there will be a 1.4–5.8 degree increase in the world's average temperature by 2100 in response to atmospheric greenhouse gas (GHG) emissions. 118 While developed countries have contributed the largest portions of GHG emissions, the least responsible and most vulnerable populations to global warming will likely suffer the greatest disease outcomes.121,122 These climatic estimates have already begun to surface in the environment as the distribution and seasonal transmission of malaria continue to increase. 120 The vector and parasite that facilitate malaria transmission are sensitive to temperature which may cause malaria to emerge in new geographic regions that were once protected by lower temperatures. Rising temperatures may also prolong the breeding season in mosquitoes which may create more opportunities for disease transmission among humans.120,121,122 Table 2 illustrates predicted changes in the pattern and distribution of infectious diseases in the event of altered weather pattern and climatic changes. 123
Top three entries are population-prorated projections, based on 1989 estimates.
WHO, 1994.
Michael and Bundy, 1995.
WHO, 1994.
Ranque, personal communication.
Annual incidence of visceral leishmaniasis; annual incidence of cutaneous leishmaniasis is 1–1.5 million cases/yr (PAHO, 1994).
WHO, 1995.
Extreme weather events resulting in heavy precipitation may cause human and animal waste to permeate waterways and drinking water sources, which in turn, may lead to increases in vector and waterborne disease outbreaks.119,121,122 For example, six years of drought followed by heavy rains in 1993 was believed to have increased the deer mouse population 10-fold; hence contributing to the spread of Hantavirus. 124 Furthermore, droughts may cause significant decreases in water supplies which hinder sanitation practices. Consequently, poor sanitation practices may increase the prevalence of waterborne disease outbreaks due to fecal contaminated water systems.121,122 Similarly, increases in ambient temperature can cause an increase in the virulence of infectious agents. For example, Legionella, the pathogen causing Legionnaires' disease thrives in warm water. 125 Figure 3 represents the number of waterborne-disease outbreaks associated with drinking water in the United States from 1971–2006. 85 From 2001–2006 when Legionnaires' disease was added to the surveillance system, it has become the single most common cause of waterborne-disease outbreaks. 85
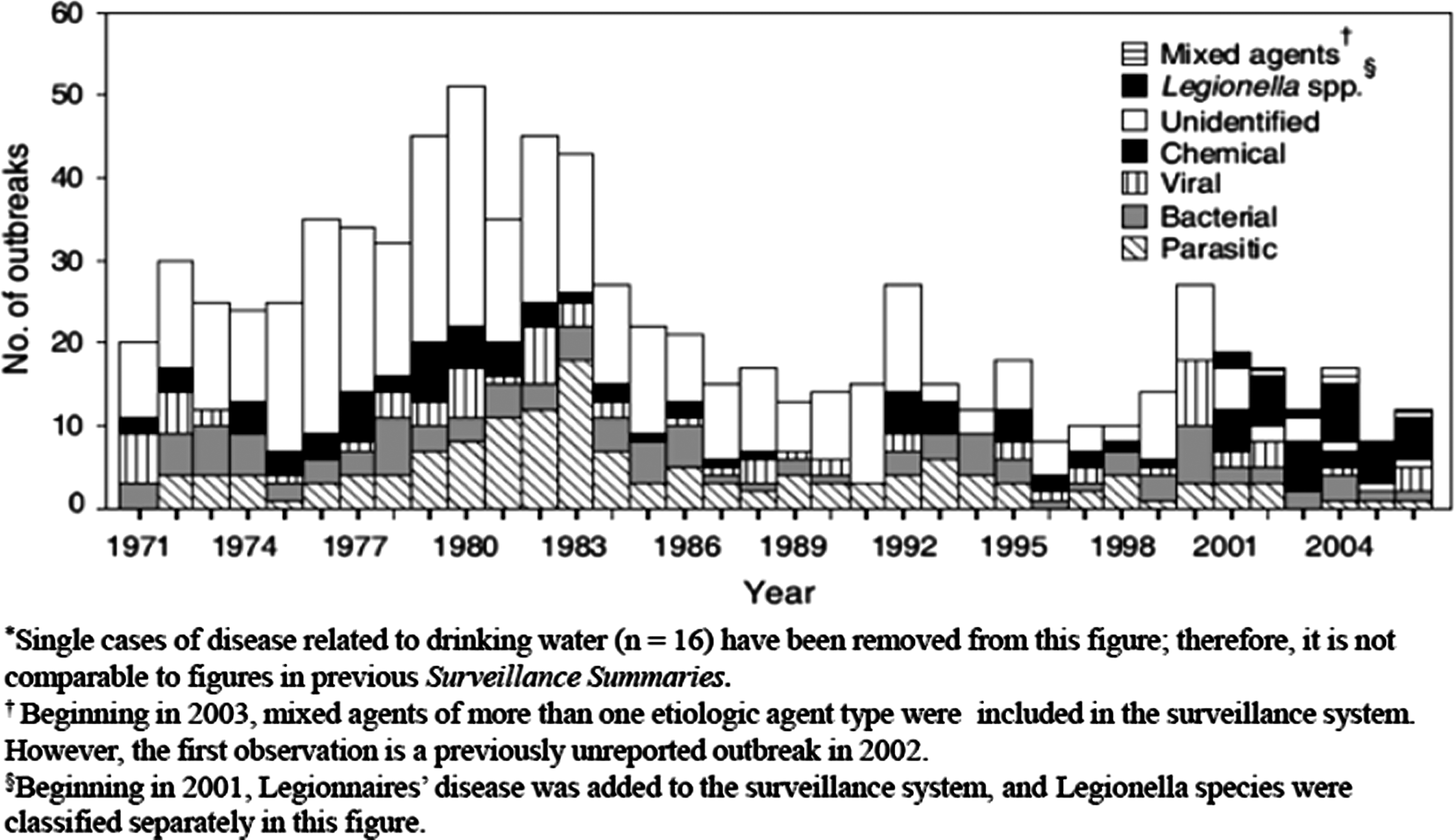
Number of waterborne-disease outbreaks associated with drinking water (n=814), by year and etiologic agent—United States, 1971–2006.
Vulnerability also influences the effects of climatic changes on health outcomes, particularly infectious diseases. Race and ethnicity should be considered when determining the degree of social vulnerability to climate change due to the inequitable access to salutogenic resources as well as the economic and political marginalization that is often associated with racial/ethnic disparities. 126
Research has shown that age may also influence vulnerability to climate change, particularly among infants and toddlers and the elderly. For example, infants and toddlers are more susceptible to the effects of climate change because they may not be able to withstand fluctuating temperatures and their immune systems might not be fully developed to counter pathogens they might be exposed to. 127 The elderly are also vulnerable because they are less mobile and unable to respond to weather warnings, in addition to already having a weakened immune system and other co-morbid conditions such as cardiovascular disease or respiratory illnesses. 127
Socioeconomic status is another factor influencing vulnerability to climate because wealth is a determinant of an individual's or community's resiliency to the effects of climate change. 126 Generally, the more economically stable will have better access to community resources for recovery as well as better access to care. 126 Health insurance tends to act as a buffer to the harmful effects of climate change, however, low-income populations are less likely to have health insurance and as a result become more vulnerable to climate change and other environmental issues. 126 When linking diseases with climate change, the Interagency Working Group on Climate Change and Health found that pregnant women and the elderly are generally more susceptible to heat and weather related illness and death, vector-borne and zoonotic diseases, and waterborne and food-borne illnesses. 128 Economically distressed individuals and low-income populations living in the inner city are often more susceptible to respiratory allergic diseases and asthma which are aggravated by climate change. More specifically, low-income populations may be disproportionately affected by climate change due to their lack of access to proper medical care. 128
In summation, infectious disease health disparities are exacerbated by climate change when vulnerable populations have limited resources and means, inadequate public health and sanitation infrastructure to address related negative health outcomes. Until the social determinants associated with infectious disease transmission are confronted, the world's most vulnerable populations will continue to be disproportionately affected by a changing environment.
Conclusion
Despite advances in the treatment and cures for many infectious diseases, infectious agents and pathogens continue to disproportionately affect socially and environmentally marginalized populations. Herein lies the limitation of the germ theory, a theory that is entirely premised on the notion of a causative pathogen and an infectious disease. The germ theory fails to recognize the role of social determinants of health, behavior, host susceptibility and vulnerability in influencing infectious disease outcome. It emphasizes a monolithic approach to infectious disease control aimed at targeting the pathogen. This approach has at best had limited results, in comparison to other approaches that have included addressing both the infectious agents and implicated social determinants.75,76,82,83
From the foregoing, it is clear that environmental change, social determinants, and infectious diseases are inextricably linked and that this relationship contributes to the emergence of new infectious diseases and re-emergence of other infectious diseases (e.g., Escherichia coli, Salmonella enteriditis, hantavirus, nipah virus, Borrelia burgdorferi, avian influenza virus, West Nile virus).46,75,76,103,123 The dichotomy between infectious disease research and environmental health has not helped in addressing this trend. We contend that there is an urgent need for a move from the current reductionist approach to infectious disease that predominantly focuses on the germ theory approach to infectious disease to one that recognizes and incorporates the role of disproportionate burden and exposure as well as social, physical, and chemical processes in the environment and their influence on pathogen dynamics, vector transmission, host susceptibility and disease outcomes among environmental justice populations.
Future public health action aimed at addressing infectious disease should include a holistic approach, one that aims at addressing the dichotomy between clinical disease and their socio-environmental determinants. This could be done through a community-based participatory research (CBPR) approach, where collaborations and partnerships between academic institutions and governmental agencies are formed with local community-based organizations. This approach recognizes the role of the community and solicits its participation, builds community capital, engenders community buy-in and empowerment, all factors that are vital in stimulating community response to addressing the social determinants of infectious disease in EJ populations.
An example of the effectiveness and success of this approach is the collaborative effort between the West End Revitalization Association (WERA), the University of North Carolina at Chapel Hill, and the University of South Carolina which has helped to address water and sewer infrastructure disparities, microbial water quality issues, and inequitable land use planning and development in low-income and underserved regions of Mebane, NC.75,76,82,83 Due to this collaborative effort, water tests showed high levels of pathogens and fecal microbes such as Enterococcus, fecal coliforms, Escherichia coli, and coliphages in drinking water supplies and turbidity levels that exceeded safety standards. This collaborative effort led to first-time installation of sewer and water infrastructure for several households with a reduction in the incidence of water-related gastro-intestinal infections.
Again, pursuant to the success of the partnership between WERA, University of North Carolina at Chapel Hill, and University of South Carolina, we advocate for similar style collaborative efforts in addressing social determinants of infectious disease. Finally, we recognize that the study of infectious disease in EJ communities is novel and call for more research in this area, especially as the focus of public health shifts towards a social and environmental approach towards disease prevention.