
Abstract
Abstract
The positive outcomes derived from the implementation of culturally sensitive educational programs in addressing disparities in environmental literacy and health among disadvantaged communities have not been rigorously examined. This report summarizes the results of a community-wide survey completed to test this hypothesis in the Cameron Park Colonia, one of the poorest communities along the Texas-Mexico border. The assessment followed a two-year training program in environmental health provided by community lay health workers using a train-the-trainer approach. Statistical analysis of data obtained from 498 households showed that educational intervention significantly improved residents' knowledge of environmental health and disease, particularly in general health knowledge and behavioral modifications to achieve healthier lifestyles. These findings show that culturally appropriate educational intervention enhanced environmental health literacy among Cameron Park Colonia residents. We advocate for the implementation of culturally sensitive training programs in environmental health in other communities to continue to improve environmental health literacy among Hispanics in the United States and to facilitate creation of self-sustainable models of environmental justice.
Introduction
In 2008, we reported the results of a longitudinal study of Cameron Park that identified asthma and allergies as the most prevalent respiratory diseases affecting adults and children.5 Other diseases affecting this community in higher numbers than the United States population included diabetes, heart disease, and hypertension. Among the documented environmental health problems along the Texas-Mexico borders that may be contributing to environmental illness in Cameron Park are pesticides, heavy metals, and hydrocarbons. Upon completion of a pre-intervention assessment, a two-year environmental educational intervention program was implemented using a “train-the-trainer” model. This model involves education and training of community lay health workers (i.e., promotoras, a Spanish term that describes residents trained to “promote” improvements in public health within their own communities). This model of peer education, partnership building, and grassroots education has been successfully used by many disadvantaged communities worldwide.6 From a cultural and educational perspective, promotoras are trusted individuals within the community who share elements of the same cultural background, economic, and health status.
Environmental education programs can range from distance education programs designed to overcome physical distance barriers between trainers and trainees7 to home-based programs designed to address communication and social barriers.8 Of relevance to disadvantaged communities has been the creation of school-based environmental health education programs,9 or community-based empowerment programs10 to facilitate dissemination of information and promote sustainability of the public health intervention.
A key element is the use of culturally appropriate interventions that empower the residents and that rely on resources within the community to promote sustainability of the intervention. This is true for Hispanics with mounting evidence showing that teaching in their own language and in a culturally appropriate environment overcomes barriers to learning and promote sustained patterns of behavior modification.11
This report summarizes the results of a community-wide survey conducted to determine the impact of a culturally-sensitive, educational intervention on environmental health literacy in the Cameron Park Colonia. The data show that environmental health literacy was significantly improved and support the conclusion that culturally-sensitive training in environmental health can help improve environmental health literacy among Hispanics and facilitate creation of self-sustainable models of environmental justice.
Methods
Study population and sampling
The door-to-door post-intervention survey of 498 households included 2,169 residents; 1,148 of which were adults and 1,021 children less than 18 years of age. Households were identified using a map of the Cameron Park Colonia developed by the research team for random sampling purposes. Interview eligibility required that an adult individual living in a home self–identified as head-of-household. All of the information obtained and reported about the youth was provided by heads of household.
The post-intervention survey was completed face-to-face by the same promotoras that completed the pre-intervention survey.12 Promotoras set up appointments prior to their visits to ensure 100% participation. Given that the same instrument was utilized for pre- and post-educational intervention assessment, perceived threats to validity were addressed by insuring a two-year longitudinal separation between pre- and post-assessment and by random assignment of promotoras to households.
Instrument
A cross-sectional population-based survey instrument was developed and administered door-to-door to residents of the community of Cameron Park.13 The instrument focused on environmental issues defined broadly to include water, indoor and outdoor air, food, lifestyles, household, noise, chemicals, pesticides, stress, working place, and neighborhood. The contents and use of a bilingual survey/instrument were reviewed and approved by the Institutional Board Review. The survey was divided into four sections that included demography, environment, health, and community perceptions with 115 questions. The validity of the instrument used was pilot-tested using a subset of residents and modified accordingly. The survey was administered in the language of stated preference of participants. The variables included background characteristics of individuals, self-reported disease conditions, accessibility to medical care and immunization, and self-reported exposures to environmental factors.
Train-the-trainer model of education
The train-the-trainer model involved training of promotoras in environmental health, safety, interview skills, medical ethics, and confidentiality. The curriculum included basic scientific principles of environmental health, toxicology and public health, nutrition, pesticides, occupational safety, and genetic susceptibility. Environmental education was provided face-to-face twice a month for eight months and certificates of completion were awarded. The level of instruction was at the middle school level to facilitate education of individuals with varying educational backgrounds.
Intervention
Community-level education took place in the residents' homes, local churches, and community centers where residents gathered often for social events, education, medical, and social services. A door-to-door interview was used for data acquisition after completion of the educational intervention. After completion of the consent form, promotoras asked questions and completed questionnaires. Participants were always offered the opportunity to open responses, and all responses were recorded immediately in writing.
Data analyses
Disease and environmental exposure frequencies were determined using the Intercooled Stata 7.0 statistical analysis package and SAS. Environmental risk factors of disease were identified using Fisher's exact test, and logistic regression techniques to evaluate the significance of association, and calculate odds ratios and 95% confidence intervals, respectively. Disease conditions were self-defined on the basis of perceived departures from self-reported health or physician diagnoses. Fisher's exact test does not rely on normality assumptions and uses an exact distribution instead of a normal approximation that replaces the .2 test when expected frequencies are less than five. The null-hypothesis of the Fisher's exact test was that there is no relationship between any two categories. Thus, every possible arrangement of observations in their respective cells is equally likely and assumed that the column totals are fixed.
The p-value was computed by calculating the number of possible arrangements of observations that produce tables that are more extreme than the observed, and dividing by the total number of possible arrangements of the observations Z test. This Z test statistic formula is used to compare the proportion from two groups in order to determine if they are significantly different from one another. It is assumed that the sample represents a random sample of the relevant population and does not require the two groups to have the same number of respondents.
Results
Demographic profile
The average age of heads of household was 50.58 years, with 79.92% identifying their gender as male. The average spouse age was 45.36 years. The majority of residents were born in Mexico with incidences of 81.05% and 80.31% for males and females, respectively. In contrast, the majority of children living in the community were born in the United States (80.15%). Most spouses and household heads were Spanish-only speakers (67.34% and 77.92%, respectively), and had less than a ninth grade education (66.67% and 64.47%, respectively).
Environmental health community profile
The majority of homes in the Cameron Park Colonia had electricity and public water supply, with the main drinking water source identified as either an inside tap or a bottled water supply. A total of 69.28% of the residents paid to have garbage removed by a private hauler, while 26.27% regularly self-hauled garbage to either a landfill or a community waste collection station. Approximately 5% of the residents either burned or buried their garbage on a regular basis, with two homes indicating disposing of garbage in the yard behind the home. Thirty-seven percent of homes reported living within one-quarter mile of a junk yard, 22.2% reported living within one-quarter mile of a car radiator repair shop, 15.3% reported living within one-quarter mile of a dry cleaning business, and 3.0% reported living within one-quarter mile of crop fields. Citrus fruits, sorghum, cotton, wheat, and corn were the most common crops grown near the Cameron Park community, with 75.5% of the households reporting pesticide exposure, either associated with home proximity to a crop field with known pesticide application via dusting planes, or pesticide use in the home or garden, or direct contact with pesticides. The majority of Cameron Park residents received primary health care at either a private physician's office (82.9%), or through a health department clinic (18.9%). Further, 78.5% obtained health care for the family solely in the United States. Smoking tobacco products was reported by 21.24% of heads of household, while only 4.27% of the spouses indicated smoking. Smoking tobacco products among child members of the families was reported by 3.15% of the responders.
Environmental health literacy
Environmental health literacy of Cameron Park Colonia residents was evaluated before and after environmental health education intervention. Significant improvements in literacy were found among residents after educational intervention, most notably in the areas of pesticide-related exposures, water-related diseases, and smoking-related diseases. Analysis of knowledge gained regarding pesticide exposures showed significant improvements in 12 different areas, most notably, the need to change clothes post-application and recognition of nausea, vomiting, and salivation as significant side effects of pesticide intoxication in humans (Figure 1). Educational intervention significantly improved knowledge related to water pollution among colonia residents (Figure 2). This was evidenced in all categories examined, and most remarkable in terms of understanding of the linkages between hepatitis, gastroenteritis, dysentery, and improvements in water quality.
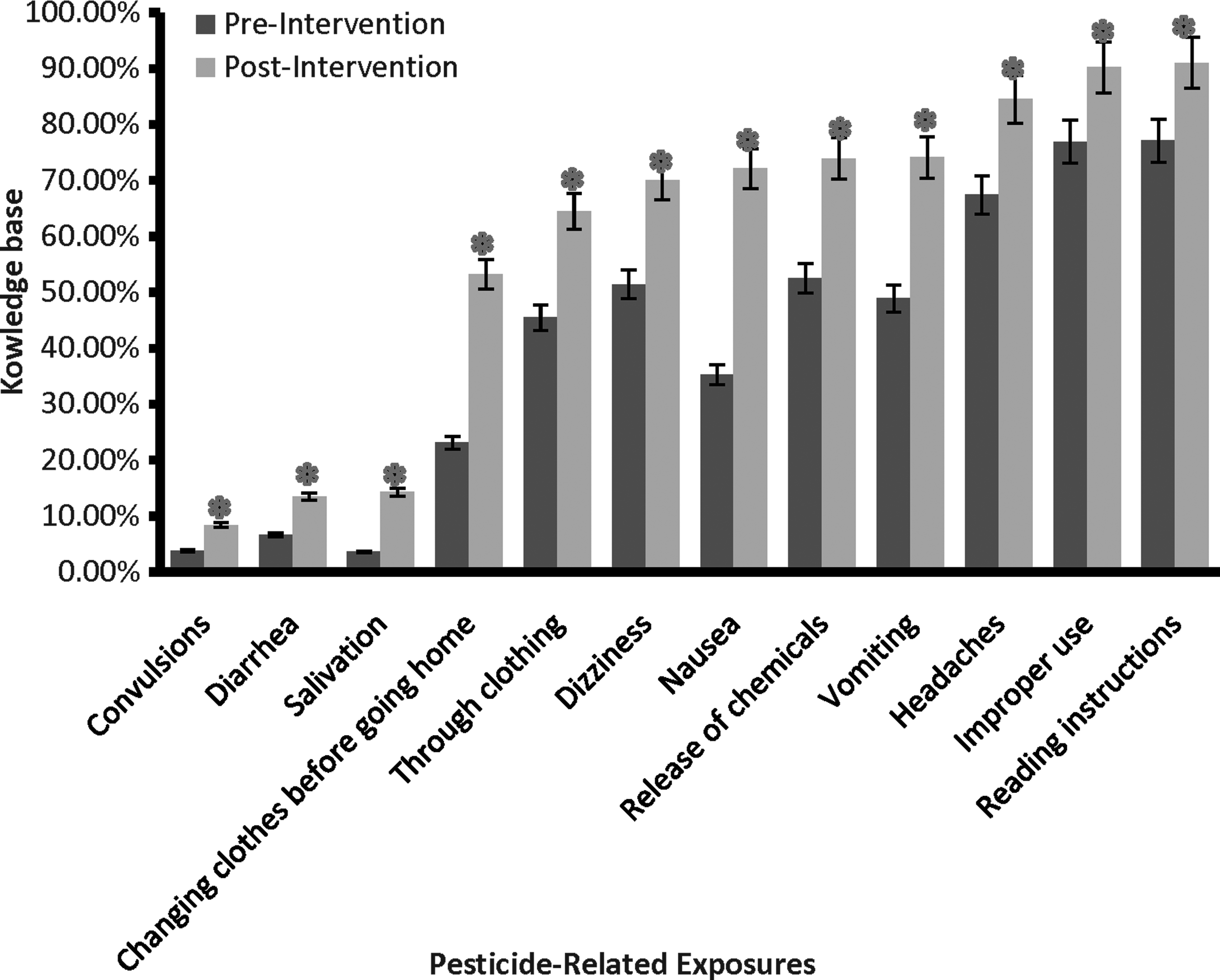
Knowledge of pesticide exposures among Cameron Park Colonia residents before and after environmental health education intervention.
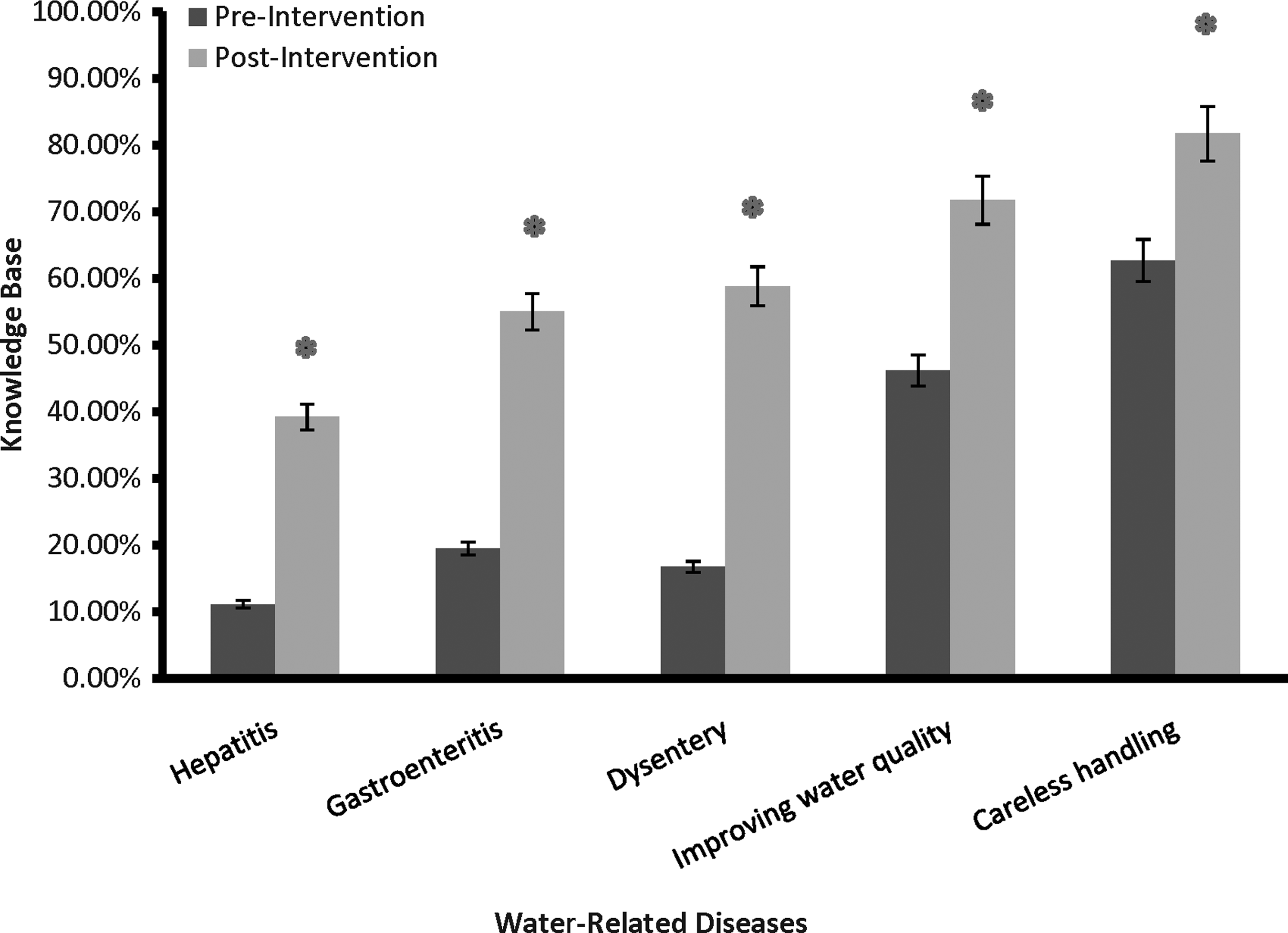
Knowledge of water pollution among Cameron Park Colonia residents before and after environmental health education intervention.
Lastly, the impact of the education intervention on understanding of smoking-related diseases and their connection to overall health was remarkable (Figure 3). This was most significant in terms of understanding the linkages between smoking and low birth weight and premature birth, and exposure to second-hand smoke.
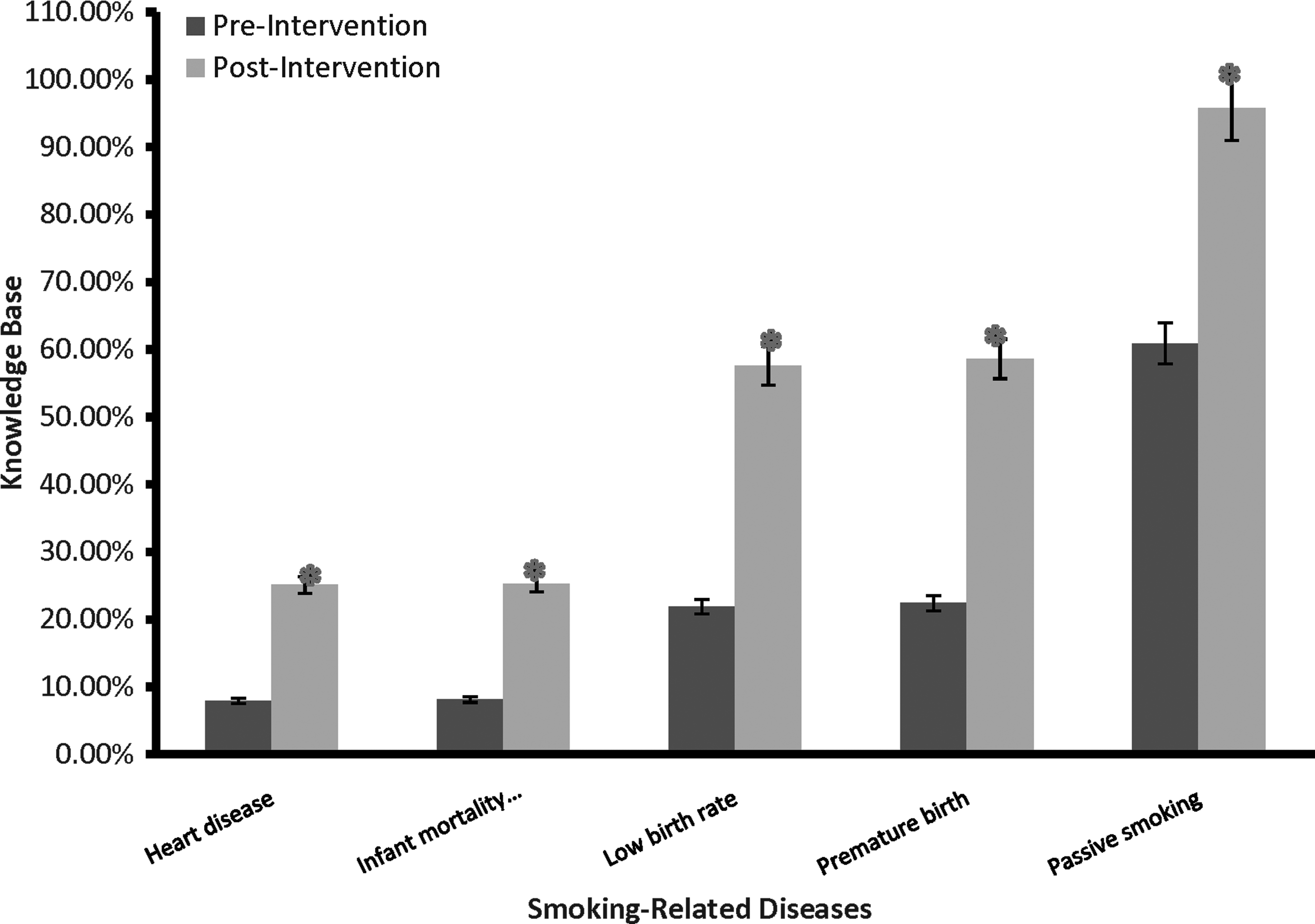
Knowledge of smoking-related diseases among Cameron Park Colonia residents before and after environmental health education intervention.
Within the context of the linkage between the environment and diseases, one of the most significant impacts of the intervention was evidenced by increased appreciation of resources available to obtain information on the environment. Another key area of focus related to knowledge of what to do for protection when handling chemicals and water pollution. A positive impact of community-wide public health intervention was detected not only in terms of general knowledge base, but also on how the knowledge was implemented to achieve healthier life styles. The impact of the educational intervention on knowledge related to birth defects and folic acid, occupational health, and general health literacy is summarized in Table 1.
Values are only shown for indices found to be statistically significant at the 0.05 level. It should be noted that while some of these indices only improved marginally, significant differences were still found when comparing the pre- and post-intervention findings.
Discussion
Culturally sensitive engagement, outreach, and educational programs have been proposed as essential elements for the development and implementation of strategies to address the environmental health challenges faced by minorities and disadvantaged communities. The evidence presented here supports this view and shows that environmental health literacy was significantly improved among residents of the Cameron Park Colonia using a culturally sensitive educational program. This approach can serve to overcome the negative health impacts posed by environmental factors among residents of communities that face ethnic, economic, and/or environmental disparities. The improvements in environmental health literacy realized may positively impact other aspects of health as they relate to access, engagement, and communication within the health care system by residents of Cameron Park. This is significant given that low health literacy continues to be a threat to the health and well-being of Americans, and the need for the U.S. health care system to better match the needs of individuals to the information and services available to them. It should be noted that the epidemiologic component of our investigation relied on self-reports of disease measured using the same instrument during the pre- and post-intervention phases. As such, the biases introduced by magnified fear or recall bias may have influenced the findings. This possibility was deemed unlikely given the remarkable consistency in incidence rates for all chronic diseases reported.
Training of community residents can be complementary to concerted efforts to engage health care professionals in combating environmental issues.14 As such, a two-pronged approach that relies on community residents working in partnership with the systems of public health and local government is needed to minimize well-recognized gradients in disease outcomes. Heslop et al. have shown that the neighborhood socioeconomic status predicts non-cardiovascular mortality in cardiac patients with access to universal health care.15 In their study, lower socioeconomic status was tightly correlated with employment and education and interestingly, vulnerability to non-cardiovascular chronic disease mortality was independent of public health care access.
These findings strongly implicate community contributions to health outcomes and suggest that educational programs can help to combat socioeconomic constraints that otherwise impact negatively health outcomes. This interpretation is consistent with recent studies showing that low parental education is independently associated with children's environmental tobacco smoke exposures at home and in cars.16 Cecchi suggested the need for information, knowledge, and know-how is inseparable from that of other tools or regulatory measures required for decision making.17 A recent study of perception of environmental health risks related to living in the vicinity of communal waste incineration plants has shown that lack of sufficient information about incinerator activity lead to increased frequency of complaints by community residents.18
Future evaluations in Cameron Park should focus on disease incidence rates and improvement in health indicators to determine if educational intervention translates into improvements of health and quality of life, as well as reductions in disease prevalence or shifts in disease outcome.
Footnotes
Acknowledgments
This work was supported in part by P30-ES09106 and P30-ES014443. We gratefully acknowledge our collaboration with Dr. Marlynn May and the Promotoras who dedicated countless hours to improve their communities.
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclose.
1
I.N. Ramos, M. May, K.S. Ramos, “Environmental Health Training of Promotoras in Colonias Along the Texas-Mexico Border,” American Journal Public Health 91 (Apr 2001): 568–570.
2
U.S. Census, 2002. Vital & Health Statistics, series 2, number 135.
3
Cameron Park Cdp, Texas. CityMelt.com. <
4
Ibid.
5
I.N. Ramos, L.B. Davis, Q. He, M. May, K.S. Ramos, “Environmental risk factors of disease in the Cameron Park Colonia, a Hispanic community along the Texas-Mexico border.” Journal of Immigrant and Minority Health 10 (Aug. 2008):345–351.
6
World Health Organization. 2008. <
7
M.L. Fleming, J. Easton, “Building environmental educators' evaluation capacity through distance education,” Evaluation Program Planning 33 (May 2010): 172–177.
8
J. Postma, C. Karr, G. Kieckhefer, “Community Health Workers and Environmental Interventions for Children with Asthma: A Systematic Review,” Journal of Asthma 46 (Jan 2009): 564–76.
9
C.C. Johnson, L. Myera, L.S. Webber, N.W. Boris, H. He, D. Brewer, “A School-Based Environmental Intervention To Reduce Smoking Among High School Students: The Acadiana Coalition of Teens Against Tobacco (ACTT),” International Journal Environmental Research Public Health 6 (Apr 2009): 1298–316.
10
D. Swendeman, I. Basu, S. Das, S. Jana, M.J. Rotheram-Borus, “Empowering Sex Workers in India to Reduce Vulnerability to HIV and Sexually Transmitted Diseases,” Sociology Science Medicine 69 (Oct 2009): 1157–1166.
11
S. Foster-Cox, T. Mangadu, B. Jacques, A. Corona, “The Effectiveness of the Promotora (Community Health Worker) Model of Intervention for Improving Pesticide Safety in US/Mexico Border Homes,” California Journal of Health Promotion 5 (2007): 62–75.
12
I.N. Ramos, L.B. Davis, Q. He, M. May, K.S. Ramos, “Environmental Risk Factors of Disease in the Cameron Park Colonia, a Hispanic Community Along the Texas-Mexico Border,” Journal of Immigrant Minority Health 10 (Aug 2008): 345–351.
13
I.N. Ramos, M. May, K.S. Ramos, “Environmental Health Training of Promotoras in Colonias Along the Texas-Mexico Border,” American Journal of Public Health 91 (Apr 2001): 568–570.
14
M. Donohoe, “Roles and responsibilities of health care professionals in combating environmental degradation and social injustice: education and activism,” Monash Bioethics Review 27 (Jan–Apr 2008): 65–82.
15
C.L. Heslop, G.E. Miller, J.S. Hill, “Neighborhood socioeconomics status predicts non-cardiovascular mortality in cardiac patients with access to universal health care,” PLoS ONE 4 (Jan 2009): 4120.
16
G. Bolte, H. Fromme, “Socioeconomic Determinants of Children's Environmental Tobacco Smoke Exposure and Family's Home Smoking Policy,” European Journal of Public Health 19 (Jan 2009): 52–58.
17
C. Cecchi, “The Role of Information in Public Health Decision-Making,” Sante Publique 20 (Jul–Aug 2008): 387–394.
18
A. Poznanska, P. Gorynski, J. Stokwiszewski, B. Wojtyniak, “Perception of Environmental Health Risks Related to Living in the Vicinity of Communal Waste Incineration Plant,” Przegl Epidemiology 62(4) (2008): 829–838.