
Abstract
Abstract
A top priority of the federal government's Healthy People initiative is to address inequalities and injustices, and to eliminate disparities by race and ethnicity, education, income, and geographic location. Unfortunately, progress toward this goal has been minimal, and low-income and some racial and ethnic minority groups remain more likely to suffer from a variety of diseases and health risks.
Inequalities in the built and social environments underlie many of the socioeconomic and racial and ethnic disparities in health risks and outcomes. Zoning is the primary tool used in the U.S. to control land use; zoning plays a predominant role in creating and maintaining built environments. The reliance on outdated zoning codes has helped contribute to various environmental injustices and inequalities.
Zoning policies have been suggested as one potentially useful tool to make communities more conducive to health, and to more equitably distribute opportunities and risks to health. Effective zoning policy has the potential to not only address the issues of dietary intake, physical activity, and related chronic diseases, but also to ameliorate several other public health problems such as exposure to environmental hazards, intentional and unintentional injury, substance use and abuse, access to health care and health disparities. This article reviews the role of zoning as a determinant of various public health problems such as chronic diseases and health disparities, and as a policy tool to address these public health issues.
Introduction
This article reviews how zoning fosters built environments that lead to health disparities. We present a conceptual framework adapted from Schulz and Northridge's “Social Determinants of Health and Environmental Health Promotion,” 5 that depicts how factors in the built and social environment, including zoning policies, contribute to health and health disparities. We conclude with recommendations for how zoning can be used as a policy tool to address health disparities and a variety of chronic disease risk factors.
The Built Environment and Health Disparities
There is substantial research linking features of the built environment to health behaviors and outcomes such as nutrition, physical activity, obesity and the disproportionate burden of these health risks among certain subpopulations.6–35 There is also substantial evidence of inequities in the built and social environments. Environmental hazards and resources are not equitably distributed by income, race or ethnicity. For example, low-income groups and some racial and ethnic sub-populations reside in neighborhoods with limited access to supermarkets and safe places to exercise, but an abundance of fast-food outlets, corner stores, liquor outlets, convenience stores, and other hazards.35–43
Research linking the built and social environment to health outcomes has been unable to establish causality because individuals choose where to live, and those who are likely to practice certain health behaviors may be more likely to live in neighborhoods that provide opportunities for exercise and healthy eating. However, associations between features of the built environment and health outcomes have been reported even after controlling for self-selection or neighborhood preference, indicating that the environment does have an impact on behavior and health outcomes. 12
A Conceptual Framework: Health Disparities in Context
Schulz and Northridge have proposed a conceptual framework, “The Social Determinants of Health and Environmental Health Promotion,” that describes how various features of the built and social environments contribute to population health and health disparities. 5 In this model, health disparities across a number of different outcomes result from differential access to opportunities, power, resources, and information, combined with differential exposure to risks and stressors. 44
We present a modified version of this conceptual framework in Figure 1. This modified framework separates out the policy context as distinct from, but related to, the built and social environments, and highlights the role of zoning and other community policies in influencing population health and health disparities. This framework is consistent with the hypothesis that inequalities in the built and social environments underlie many of the socioeconomic and racial and ethnic disparities in health risks and outcomes such as diet, physical activity, and obesity.20,35,37,41,45,46 Individuals facing social and economic disadvantage, notably many racial and ethnic subpopulations and low-income individuals, are especially vulnerable to environmental risk factors.23,27,46,47 This differential exposure and vulnerability to risk factors in the built and social environment contributes to numerous health disparities.5,37,46,47
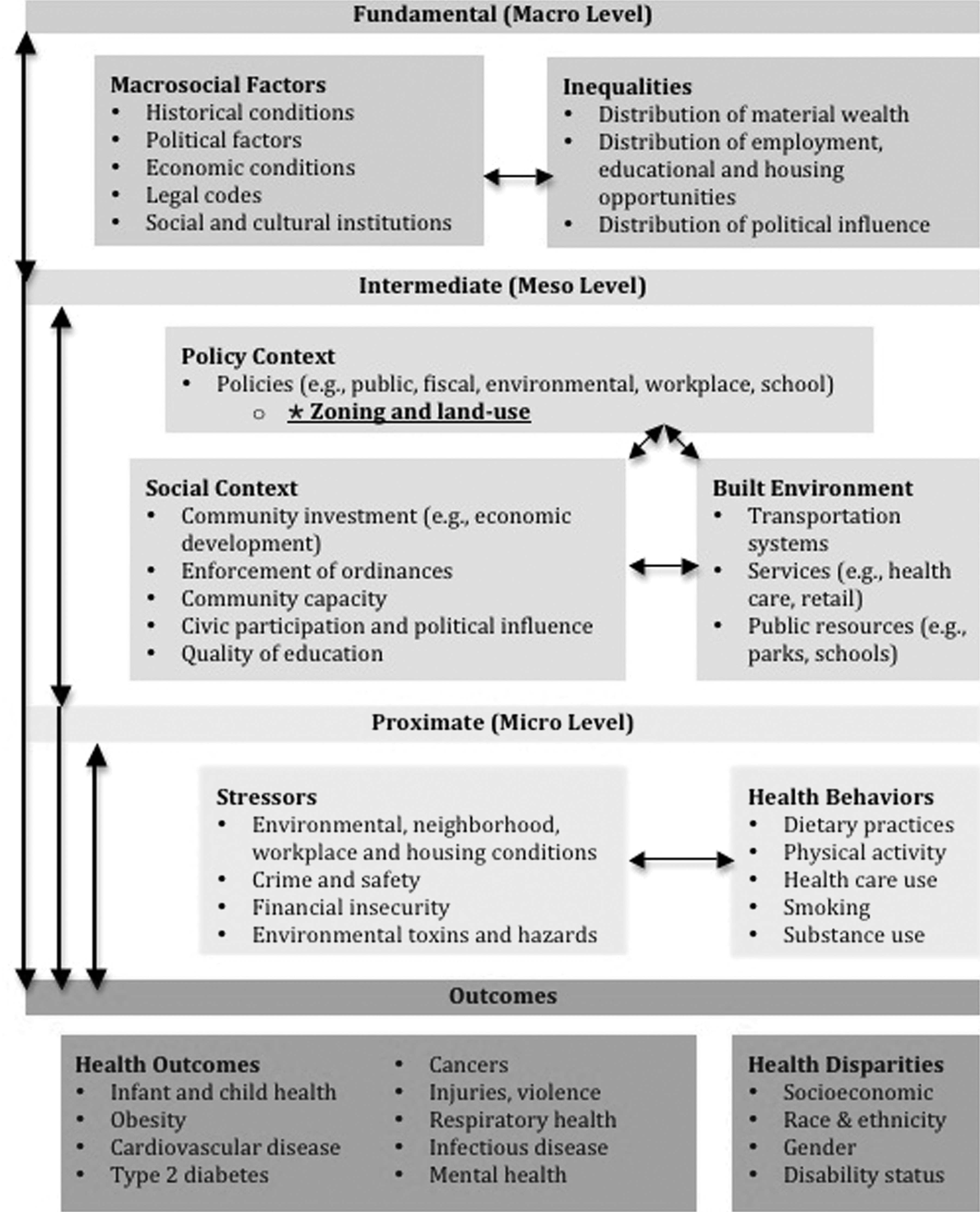
Conceptual framework illustrating how various features of the built and social environments contribute to population health and health disparities. Adapted from Schulz and Northridge. 5
Many researchers have argued that residential segregation is a fundamental cause of health outcomes and disparities because segregation creates inequities in neighborhood socioeconomic status (SES), employment and education opportunities, housing quality, access to social and material resources to promote health, and exposure to risks and hazards.48–51 In a recent analysis, racial disparities in diabetes, obesity, and healthcare utilization were not evident after controlling for the effects of racial segregation; disparities in hypertension were reduced by about one third. 49
Collectively, the research suggests that inequities in the built and social environments underlie disparities in health risks and outcomes.
Zoning Policies
Zoning is defined as, “action by the state, or by a city under authority of the state, to control…a) the heights to which buildings may be erected; b) the area of lots that must be left unbuilt upon; and c) the uses to which buildings and lots may be put.”52–54 Zoning is the primary tool used in the U.S. to control land use; zoning determines what kind of buildings or land uses are allowable in specific locations. 55 Zoning plays a predominant role in creating and maintaining built environments. There is a long tradition of using zoning to protect public health, stemming from the state's (and delegated municipalities) police power.a,58,59
Although zoning is rooted in the interest of protecting the public's health and welfare, it has historically been applied to deal with problems of pollution and communicable diseases. 60 To deal with these public health problems, the practice of zoning focused on separating uses: keeping industrial, commercial, and residential areas apart. This practice was effective in mitigating exposure to noxious industrial pollutants and reducing the transmission of communicable diseases. 61 However, this doctrine of separation of uses, or Euclidean zoning, is still the most widely used method of zoning in the U.S., 62 despite the fact that the public health challenges of today are drastically different than a century ago.
Zoning as a Problem
“Ironically, our failure to adapt the land development regulations and transportation facility design standards over time has resulted in the promulgation of health adverse environments as a norm and not the exception.” 63 (p. 214) Many zoning resolutions still in place today date back to decades ago when planners were dealing with a much different society that relied heavily on manufacturing and where the leading causes of death were communicable diseases. Today, the leading causes of death in the U.S. are chronic diseases such as heart disease, stroke, cancer, and diabetes; and behavioral risk factors for these diseases such as smoking, obesity, poor diet, and inactivity are now the most pressing public health issues facing communities.3,64 While planners may have the public's health in mind when zoning to ensure industrial emissions are separated from residential areas, the broader impacts of zoning on behavioral risk factors such as diet, physical activity, and related health conditions have typically not been factored into zoning decisions.59,60
Outdated and archaic zoning codes can serve as barriers to healthy communities by supporting automobile-dependent lifestyles and urban sprawl, and limiting availability of healthy food and opportunities for physical activity, particularly in low-income or disadvantaged neighborhoods.14,15,46,60,65 For example, in part because of urban sprawl, access to healthy food in Baltimore City has declined over several decades as supermarkets fled the city to the adjoining suburbs; 66 this “supermarket flight” has occurred in many other urban areas. 67 Residents therefore need automobiles and other forms of transportation to obtain healthy food, as the local corner stores within walking distance typically do not carry healthy food products.66,67 The reliance on outdated zoning practices in Baltimore City and other urban areas has helped foster the development of unhealthy and unsafe built environments that impede opportunities for physical activity and healthy eating, contributing to rising rates of chronic disease and widening health disparities.10,46,68 These “riskscapes” have been associated with numerous other public health problems such as risk of intentional and unintentional injury, food insecurity, pollution, and associated health risks such as asthma and cancer.22,32,46,63 Moreover, industrial and manufacturing areas are responsible for a high burden of environmental and health risks such as noise, reduced air quality, dumping of hazardous materials and environmental contaminants and pollutants that enter the water or soil. These risks tend to be concentrated disproportionately among poor neighborhoods and communities of color.10,22,43,46,55
Research has suggested that noxious facilities are deliberately sited in disadvantaged neighborhoods, rather than low-income or minority groups moving in to communities fraught with environmental hazards. 43 A longitudinal analysis of the siting of hazardous waste facilities in Michigan between 1950 and 1990 concluded that hazardous facilities followed the “path of least (political) resistance” and were more likely to be sited in poor communities of color; “because of their political and economic vulnerability, low-income and minority neighborhoods are less likely to defeat siting proposals and are more likely to receive proposals deflected from more politically powerful (i.e., affluent, white) areas.”69(p. 619) Similar patterns were evident in East Los Angeles, Commerce, and San Jose, California; Pittsburgh, Pennsylvania; Gary, Indiana; Memphis, Tennessee; and Chicago, Illinois. 69
Often these health risks are considered as separable phenomena, with idiosyncratic issue-specific causes and solutions. However, many health outcomes are linked in that they share a common pattern of environmental and social determinants that tend to disproportionately affect the poor and certain racial and ethnic subpopulations. Zoning, insofar as it determines the built environment, is one such link that ties together various health risks and related disparities. Zoning has been indentified as a cause of socioeconomic and racial segregation,70–73 and segregation fosters health disparities.49,51 A syndemic or systems framework recognizes the common causal pathways that create and maintain health in a broad sense, and attempts to explain and ameliorate the conditions that perpetuate health inequities across myriad risk factors, conditions, and outcomes.74–77 Zoning therefore has profound implications for health disparities and environmental justice, as it has contributed to various inequities in the distribution of environmental risks and resources.
Failure to update archaic zoning codes that promote environmental injustices may in fact be illegal. Executive Order 12898, signed in 1994, stipulates that, “no group of people, including a racial, ethnic, or a socioeconomic group, should bear a disproportionate share of the negative environmental consequences resulting from industrial, municipal, and commercial operations or the execution of federal, state, local, and tribal programs and policies.” 78 Unfortunately, many (if not most) municipalities across the U.S. may be in violation of this executive order, as the continued reliance on outdated zoning codes and practices perpetuates inequalities in the built environments. Although land-use decisions are legally required to be race-neutral, they represent a form of institutionalized racism whereby certain groups bear a disproportionate burden of environmental risks and hazards. 69 Communities with wealth and political power are able to influence the zoning process to prevent undesirable uses from being sited within a particular location.48,50 This process applies not only to hazardous waste facilities, but also to other types of land uses such as tobacco retailers, alcohol outlets, and fast food or carryouts. 48 For example, wealthy and predominantly white areas such as the Upper East Side in Manhattan or the town of Calistoga, California have been able to ban fast food outlets from opening. 48 By contrast, segregated, low-income communities of color often lack similar access to political influence and power and therefore are unable to prevent noxious land uses.50,55 Several predominantly Black communities have attempted to prevent the siting of fast food restaurants and lost. 48
Although the elimination of health disparities has been a national priority for decades, progress has been limited. Here, zoning may play a role as well. Schulz and Northbridge point out that informational interventions, such as providing communities with information about type 2 diabetes management or healthy eating, may in fact exacerbate disparities, because more advantaged groups are better able to utilize this information due to better access to resources. 5 Disadvantaged groups, such as low-income or some racial and ethnic subpopulations, are unable to act on health promotion information due to restricted access to resources such as health care facilities, healthy food, physical activity spaces, or transportation. Public health campaigns that rely on education, information, or social marketing may worsen existing health disparities without concomitant changes to the built and social environments. Zoning is one way by which these environmental inequalities and barriers are perpetuated, rendering many public health campaigns not only ineffective for communities lacking access to various health resources, but also potentially deleterious with respect to health disparities.
Although outdated zoning policies can contribute to unhealthy and unequal built and social environments, more effective zoning has tremendous potential to positively impact health and reduce health disparities. Importantly, the built environment is, “especially subject to policy manipulation…and these types of interventions may have the greatest potential benefit for improved population health and well-being.” 44 (p. 560)
Zoning as a Policy Solution
Zoning is a policy tool with tremendous potential to address a broad swath of public health problems at the community level.53,54,58,79,80 Zoning has the potential to not only address the issues of disparities in diet, physical activity, and related diseases, but also to ameliorate several other public health problems such as exposure to environmental hazards, intentional and unintentional injury, substance use and abuse, and access to resources such as health care. Zoning has implications for many interventions that have been proposed or implemented in order to address several public health priorities such as chronic diseases or health disparities:
• Supporting urban farms and agriculture, community gardens, or farmers markets by allowing for these uses in certain areas. • Bringing supermarkets to underserved areas or food deserts by removing zoning barriers (e.g., lot size requirements) or providing other incentives. • Using conditional use permits to: require corner stores or grocery stores to stock a certain proportion of shelf-space with healthy food products; restrict food outlets from offering high-calorie, low-nutrient foods within a specified distance of a school; or prohibit the distribution of toys or other child-targeted promotional materials at restaurants unless food meets specified nutritional standards. • Encouraging active transportation (i.e., walking or biking) through complete streets, sidewalks, bike paths, and street connectivity. • Facilitating access to open spaces, parks, and playgrounds for active play. • Limiting availability of liquor or tobacco retail outlets within a certain distance of child-centered spaces (e.g., schools, recreation centers, playgrounds). • Mitigating the effects of climate change by increasing tree canopy, green space, and access to public transportation. • Reducing traffic to decrease pollution and other hazards such as injuries. • Increasing access to health care facilities. • More equitably distributing resources to address health disparities by race and ethnicity or income. • Creating or preserving mixed-use and mixed-income neighborhoods.
There is a long tradition of using zoning to protect public health and welfare. Zoning policies have been used to effectively restrict alcohol outlets in many communities, with the rationale that there is substantial evidence of a correlation between the availability of alcohol and subsequent alcohol-related health problems and other adverse consequences.54,79 There are several places that have restricted the availability of alcohol in a community, often by prohibiting operation of retailers within a minimum distance of a school or church. 58 Recently, planners and public health practitioners have begun to collaborate in order to better utilize zoning as a potential tool to facilitate health and health behaviors such as diet and physical activity. 81 Many local governments have used zoning to limit the number of restaurants and convenience stores in specified areas, to provide incentives to stores providing healthy foods or to open in a given locality, or to facilitate physical activity through modification of the built environment.53,54,79,80
For example, TransForm Baltimore is an initiative to rewrite Baltimore City's zoning code in order to address current public health concerns such as lack of walkable spaces or access to healthy food. 82 Recommendations in TransForm Baltimore include: a) increase green space; b) zone for mixed land use to increase equitable and convenient distribution of services (e.g., grocery stores, pharmacies, schools, physical activity spaces); and c) separate healthy and unhealthy uses (i.e., ensure “unhealthy” structures such as certain food outlets or liquor stores are not near schools). The plan also seeks to ensure that all residents are within 1.5 miles of quality groceries and neighborhood services, create a complete bikeway system, implement traffic-calming strategies, improve parks and open spaces, implement “Safe Routes to School” programs, and improve pedestrian and bike access to schools. 83
Although health is well within the appropriate purview of zoning code modifications, it is common for zoning policies to be passed with the stated purposes of reducing street congestion, improving livability or neighborhood “character.”53,54,84 The “Health in All Policies” strategy calls for all public policies to be assessed in terms of their potential impact on population health, recognizing that “nearly all social determinants of health fall outside the direct control of the health sector.” 85 (p. 325) There are several principles of “Health in All Policies” that are relevant to zoning: creating alliances and partnerships recognizing mutual interests; ensuring joint and transparent decision-making; engaging stakeholders and pooling perspectives and intellectual resources; encouraging experimentation and innovation; and integrating social, economic and environmental goals. 86
Consistent with the “Health in All Policies” approach, public health practitioners need to capitalize on potential partnerships across disciplines and interests. For example, individuals interested in obesity, injuries, substance use, physical activity, diet, climate change, and environmental health all have something to gain from more effective zoning policies. Coalition building can be helpful in creating support for policy change and in strengthening potential policies by incorporating many different viewpoints and interests. In the process, the potential benefits of zoning changes are amplified across many different disciplines and health outcomes.
Not only do public health researchers and practitioners with different interests need to all be engaged in the planning process, but also communities and other stakeholders need to be engaged as well. Communities need to be aware of the rationale behind zoning decisions and be involved in the decision-making process to the extent possible. Before policies are implemented to restrict a certain type of outlet in a given area, or to build a bike path, or to bring a supermarket to a particular neighborhood, communities should be consulted. If residents have no interest in biking, then perhaps those resources would be better directed toward more pedestrian-friendly strategies. Or perhaps residents would prefer to incentivize small grocers and corner stores to stock healthier items as opposed to bringing in a large chain supermarket.
Every possible effort should be made to assess the distribution of benefits and harms of public policies, including zoning, and to ensure that these are equitably distributed across the population. Existing zoning codes should be examined with a special focus on how current rules may contribute to environmental injustices and health disparities. Remediating these inequities should be a priority. Special efforts need to be made to engage underserved, disenfranchised populations and communities in the decision-making process.
Conclusions
When applied effectively and creatively, zoning can be used to address dozens of public health priorities simultaneously, consistent with a syndemic or systems framework. The focus needs to shift from targeting individual diseases and health risks to the underlying ties that bind those disease and health risks together.74–77 Adopting a syndemic or systems perspective would help to avoid unintended consequences by simultaneously considering multiple outcomes and the various ways in which policies or programs may be developed to positively impact population health more completely, comprehensively, effectively, and equitably.75,87 For example, policies to create bike paths need to be developed with an understanding of how these changes may impact residents' risk of injury, or the likelihood of this policy benefitting low-income populations. One way to better integrate public health and planning is to conduct health impact assessments (HIA), to assess the potential health impacts of planning activities.63,88 A recent HIA of Baltimore City's zoning code rewrite reported several ways in which the changes could positively impact residents' health. 89 By increasing access to supermarkets and farmers markets, creating more mixed-use and walkable neighborhoods, and relying on traffic- and crime-mitigating design strategies, the zoning code rewrite could reduce crime and improve resident health outcomes such as physical activity, diet, obesity, and related diseases. 89
Zoning is only one policy tool among many, and is not without its drawbacks. There is a tremendous body of literature to document the existence of environmental inequities and health disparities; 90 and research linking these inequities in the environment to health disparities is accumulating. However, the efficacy of zoning as a policy intervention to reduce health disparities is largely unknown. At present, there is some empirical evidence that changing the built and social environment can improve health and health disparities,91–96 but the effectiveness of zoning policies has not been demonstrated. More research is needed to document the effectiveness, cost, and sustainability of systemic, community interventions such as zoning in improving population health outcomes and reducing health disparities.
The precautionary principle dictates that lack of evidence demonstrating the effectiveness of zoning to address health disparities and various public health problems should not be a barrier to action. “When problems urgently demand solutions, waiting for a high degree of scientific certainty may be inappropriate and may even exacerbate risk of harm.” 63 (p. 217) The reliance on outdated zoning practices and codes has contributed to the creation of built and social environments that pose numerous risks to health and foster disparities. Although evidence-based decision making should be pursued when possible, the public health risks associated with preserving the status quo should serve as an impetus for action, even in the face of scientific uncertainty surrounding the impact of zoning code changes.
Zoning has tremendous potential as a policy tool to transform the environment in order to simultaneously address multiple determinants of health in a cost-effective and sustainable way, as well as redressing substantial socioeconomic and racial and ethnic disparities in health, but much research needs to be done to evaluate the effectiveness, cost, and feasibility of such efforts. Evaluation is critical to any future policy interventions, in order to build the evidence base for what works, as well as determine the most cost-effective methods to redress health disparities and improve health on a population scale.
Footnotes
Author Disclosure
The authors have no conflicts of interest or financial ties to disclose. This research was supported in part by the Johns Hopkins Center for a Livable Future Eating for the Future Fellowship program.
a
Zoning policies restricting certain types of retail (e.g., fast food) have been challenged in court on several occasions. Generally, the zoning laws have withheld scrutiny, so long as the policies are reasonably or rationally related to the public's health, safety, morals, or general welfare.54,56 The Supreme Court has confirmed that zoning to promote public health is a legitimate exercise of a state's police power.53,54,57