
Abstract
Abstract
Asbestos is a natural mineral with observable, repeatable effects that have long been observed and repeated. Despite experiential and scientific evidence illustrating its deleterious impact on human health the worldwide production and consumption of asbestos remains substantial. The objective of the present study is to highlight the global decline and resurgence of asbestos over the period 1960–2011. This history is characterized by the predominance of asbestos in the industrialized countries until 1970, decline thereafter, but the precipitous increase of asbestos consumption in the developing countries, particularly the industrializing middle-income nations. In turn, global asbestos consumption in 2011 approximates that observed in 1960; notwithstanding voluminous evidence illustrating it is associated with asbestosis, lung cancer, and mesothelioma. Further, I highlight the rhetoric of denial consistently employed by the industry to generate uncertainty and sustain the demand for asbestos. The conclusion reiterates the need for environmental justice scholars and activists to consider the transnational movement, or risk transference, of recognized occupational and environmental hazards.
Introduction
T
Global consumption reached a high point around 1980 (Virta 2006) but then declined as government regulations and legal liabilities arose in the industrialized countries. This decline ceased around 2000 and for over a decade the overall production and consumption of asbestos has stabilized. The countries consuming asbestos today are not those doing so three decades ago, however, as it is now primarily utilized in the industrializing middle-income nations.
The objective of the present study is to outline the variable consumption of asbestos from 1960–2011 and highlight those dynamics contributing to its persistence as an industrial and commercial material. Further, I outline the rhetorical strategies of denial employed by the industry that has accompanied continued production and consumption within a context of empirical evidence illustrating its deleterious effects on human health. The conclusion highlights the environmental justice implications of asbestos as a globalizing occupational and environmental hazard.
The Global Resurgence of Asbestos
The advantageous properties of asbestos have been recognized for thousands of years (Alleman and Mossman 1997; Castleman 2005). It is thermal and chemical resistant, strong, and yet flexible; for decades it was considered a “magical” mineral in the industrialized countries (Tweedale 2000). The global asbestos industry arose in the mid-nineteenth century in response to the need for fire resistant and durable materials in heavy industrial production (Lilienfeld 1991; McCulloch 2006). Into the twentieth century the automobile and home construction industries further accelerated production of asbestos-based products.
Evidence of its impact on workers arose in the beginning decades of the twentieth century as reports of a fibrotic lung condition became commonplace (Greenberg 2005; Lilienfeld 1991). “Asbestosis” is characterized by the development of scar-like tissue that progressively obstructs lung functioning. It can cause disability and eventual death (Mossman et al. 1990), and it may precede lung cancer (McCulloch and Tweedale 2008). By the 1940s and 1950s laboratory and epidemiological studies illustrated a link between asbestos and lung cancer (Greenberg 2005; Lilienfeld 1991). Many of the early studies were coordinated by the industry in concert with their corporate insurers and knowledge of its carcinogenic effects was suppressed (Huncharek 1993; Kazan-Allen 2003; Lilienfeld 1991; McCulloch 2006; McCulloch and Tweedale 2008).
The connection between asbestos and lung cancer gained increasing attention in the 1960s and 1970s as independent scientists and physicians began to observe an empirical relationship (Lilienfeld 1991; McCulloch 2006). Researchers later established an association between asbestos and mesothelioma. A cancerous tumor of the cells lining the lungs, heart, and/or the gastrointestinal tract (McCulloch and Tweedale 2008; Mossman et al. 1990), mesothelioma is almost always fatal. There is no known cure and median survival time from initial presentation is 9–12 months (The Lancet 2008). By the 1970s, in turn, the asbestos industry was under scrutiny.
Figure 1 highlights global asbestos consumption from 1960–2011.1 Aggregate demand increased from 1960 until around 1980. As the liabilities of asbestos became increasingly difficult to deny, however, the industrialized countries incrementally restricted asbestos use and global consumption decreased. The drop is particularly notable around 1990. A decade later the decline ceases and from 2000 to 2011 global consumption illustrates a more constant trajectory.
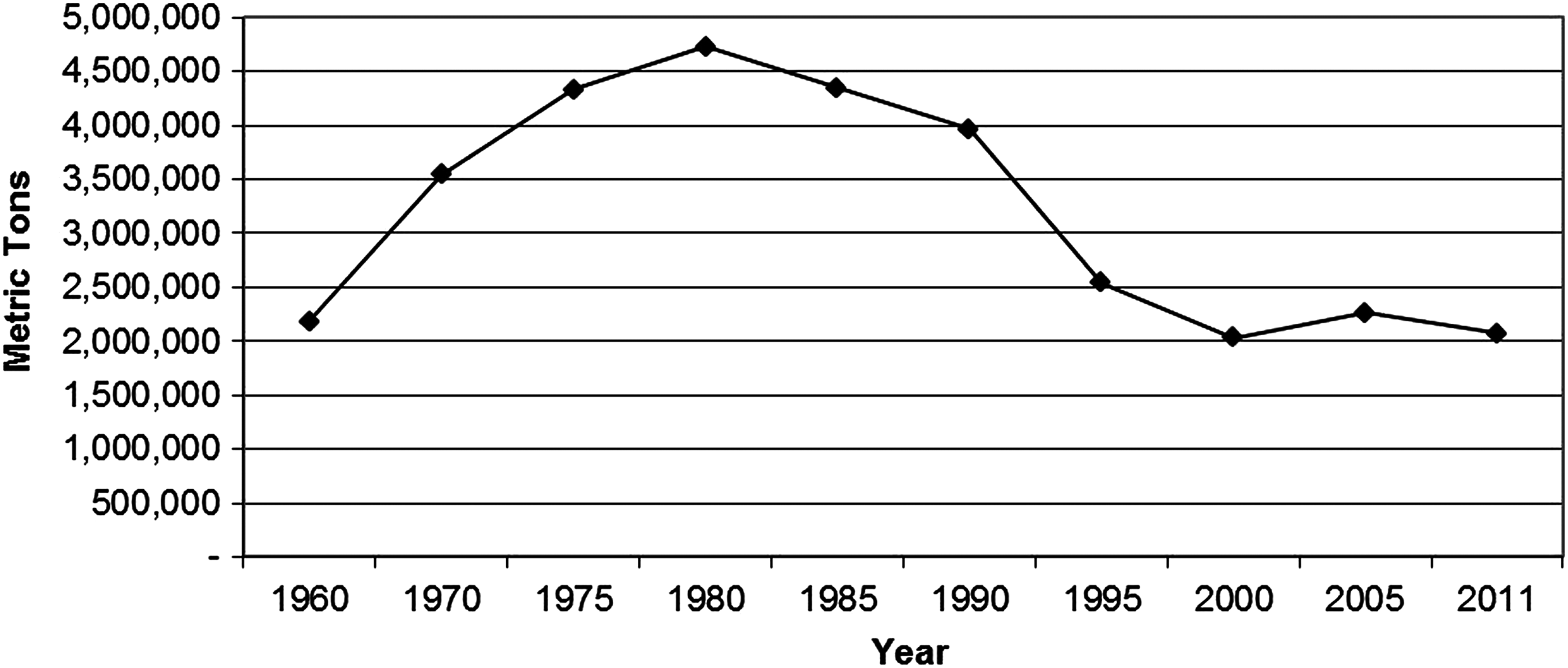
Global asbestos consumption, 1960–2011.
The protracted decline in aggregate demand outlined in Figure 1 obscures the global reorganization of the industry. Figure 2 illustrates variable consumption between developing and developed countries over the period 1960–2011.2 From 1960–1970 asbestos predominated in the industrialized countries and demand declined tepidly over the next decade before collapsing around 1980. Of particular note is declining consumption in the developed countries in tandem with increasing demand elsewhere. This is, in part, indicative of transnational corporations (TNCs) based in the industrialized countries operating through subsidiaries abroad and taking advantage of lower labor and environmental regulations. Frey refers to “risk transfer” (2003: 317, 2006) in characterizing such movement of hazardous production processes and commodities as TNCs seek a more amenable business context.

Asbestos consumption by developing and developed countries, 1960–2011.
Risk transference was only partially successful, however. Beginning in the 1970s large TNCs gradually abandoned the production of asbestos and asbestos-based products in the developed countries and then later disinvested in such activities in the developing countries as well (McCulloch and Tweedale 2008). Negative publicity made direct risk transference problematic, a reflection of the power of public opinion to circumscribe corporate practices. The export of Canadian asbestos is a notable exception as it has persisted for an extended period (Attaran et al. 2008; Kazan-Allen 2004). Although the export of Canadian asbestos has declined notably since 1980, the Canadian government and domestic asbestos industry has nonetheless consistently worked to thwart national asbestos bans as well as a global ban (Kazan-Allen 2004; La Dou 2004).
Today, asbestos mining, milling, and manufacture are primarily conducted by large national firms and small, disparate private companies in the developing countries (LaDou 2004; McCulloch and Tweedale 2008). Small indigenous firms, McCulloch and Tweedale (2008) note, are typically unregulated and insensitive to bad publicity. They operate within a global economy in which hazardous production is an advantageous niche.
Table 1 outlines the major producers and consumers of asbestos in 2011. The top three consumers worldwide include China, India, and Russia. Of note, both China and Russia are also major producers, with Russia acting as a key exporter to middle and low-income countries. Brazil and Kazakhstan also engage in significant production and consumption in 2011.
Asbestos and the Rhetoric of Denial
Just as a magician diverts attention from one hand onto another, dominant organizations often embark upon rhetorical strategies designed to obscure some material practices while highlighting others (Freudenburg and Alario 2007). Indeed, the global asbestos industry, comprised of an assortment of companies, front-groups, and industry associations, has survived due to concerted efforts to “keep alive the fiction that asbestos can be used safely” (Kazan-Allen 2003; McCulloch 2006: 609). And it has done so despite confronting three emergent crises: asbestosis (1920s), lung cancer (1940s), and mesothelioma (1960s) (McCulloch and Tweedale 2008). Arguably, the rhetoric of denial has long constituted a key strategy employed to obscure the observable biophysical effects of asbestos exposure.
Cohen (2001:3) notes, “Statements of denial are assertions that something did not happen, does not exist, is not true or is not known about.” And he puts forward a typology of denial (1996, 2001), illustrated in Table 2. Each may be invoked sequentially or concurrently.
Table adapted from Cohen (1996).
Literal denial asserts “nothing happened” or “nothing is happening” and is advantageous when there is scant counter-evidence to dispute such claims (Cohen 1996:523). If counter-evidence becomes more readily available literal denial can be implied rather than overtly asserted by working to discredit critics. This generally entails publicly questioning the credibility of accusers and may include efforts to suggest they have a hidden political agenda, are biased, naïve, or subject to manipulation through a third party. Moreover, Cohen refers to “magical denial” to describe those instances when it is asserted something did not or is not happening as it is prohibited by established policy or protocol (Cohen 1996:524).
The asbestos industry has long engaged in literal denial. This is vividly exemplified by the “secret histories” or reports, memos, and studies conducted by the asbestos industry but hidden from the public only to be uncovered through legal discovery processes decades later (Huncharek 1993; Kazan-Allen 2003; Lilienfeld 1991; McCulloch 2006; McCulloch and Tweedale 2008:7). These secret histories highlight the discrepancies between the public assertions of the major players in the industry with their internal understanding of the impacts of asbestos on human health. Moreover, the industry has a long history of attacking those who proffer opinions and/or scientific evidence disputing the safety of asbestos (McCulloch and Tweedale 2007, 2008).
Interpretive denial affirms “what happened is really something else” (Cohen 1996:522). It thus seeks to proffer an alternate explanation for something that cannot be denied outright. As Cohen observes, it often entails admission of basic facts but denial of the substantive meaning ascribed therein by oppositional claims. Lung cancer is a predominant expression of asbestos exposure, for example, but other things contribute to lung cancer, particularly smoking. Historically this has provided the asbestos industry with the opportunity, the discursive space, to engage in interpretive denial by blaming tobacco, and thus individual workers, for their lung cancer (Michaels 2008). Combined with the latency period between asbestos exposure and confirmation of disease, which can range from 10–40 years (McCulloch and Tweedale 2008), the multi-variant etiology of lung cancer is advantageous in terms of sowing uncertainty relative to even the most rigorous of scientific studies implicating asbestos.3
Mesothelioma as a disease distinctive to asbestos exposure, however, eventually undercut the salience of industry invocations of interpretive denial. Rarely observed except in relation to asbestos exposure (McCulloch and Tweedale 2008), mesothelioma is difficult to sustainably deny in a literal or interpretive manner. Relatively low levels of exposure, moreover, can eventuate in disease (McCulloch 2006; McCulloch and Tweedale 2008). Mesothelioma is not only more difficult to deny but blurs the boundaries between asbestos as an occupational hazard and an ambient environmental threat (McCulloch 2006).
Implicatory denial stresses “what happened is justified,” and is generally buttressed by the claim of necessity such that the issue or event in question is argued to have occurred more by circumstance or extant forces beyond control than by choice alone (Cohen 1996:522). Cohen notes implicatory denial is frequently combined with the claim of uniqueness such that the activity or event is asserted to have occurred in a context so anomalous that normal standards of judgment are therefore not applicable. Partial acknowledgement consists of limited admission of mistakes or wrong-doing in tandem with assertions such errors were limited to past practices, unrepresentative of overall and/or current practice, and have been corrected.
Literal and interpretive denial persist, but a prevailing rhetorical strategy employed today is partial acknowledgement of past mistakes due to reliance upon particular types of asbestos in tandem with the identification of chrysotile asbestos as a safe alternative under “controlled use conditions.” Six minerals are included under the label “asbestos” and further categorized into two sub-groups: amphiboles and serpentine (Virta 2006). The amphiboles include: amosite, tremolite, crocidolite, actinolite, and anthophyllite. The only variety in the serpentine group is chrysotile. The amphiboles are stronger and stiffer and thus more dangerous to human health (Alleman and Mossman 1997). Chrysotile is softer, more flexible, and exhibits lower biopersistence such that it is dissolved or expelled from the human body more readily (Alleman and Mossman 1997).
Virtually all of the asbestos consumed in the world today is chrysotile (Virta 2006). The Asbestos Institute, a high-profile Canadian non-profit organization, argues chrysotile is “among the least hazardous of industrial fibres” (The Asbestos Institute n.d.: 2).4 A recent industry pamphlet states (Chrysotile Institute 2008:1):
Today, distinction has to be made between chrysotile and the amphiboles varieties of asbestos. Numerous and exhaustive studies provide robust data and underscore the major difference in health risks between chrysotile and amphiboles. With the application of control measures, high-density products and the use of uncontaminated chrysotile fibres, there is no significant health risk for workers, the environment or the general public.
That chrysotile is safe under controlled use conditions or that controlled use conditions approximates the manner whereby chrysotile is utilized in the developing countries are assertions increasingly under assault.5 Research illustrates chrysotile is linked to pulmonary fibrosis and lung cancer (Harrison et al. 1999; LaDou 2004; Landrigan et al.1999), even at low levels of exposure (Joshi and Gupta 2005; WHO 2006). Some researchers argue the association is less robust than that observed with amphibole fibers (Mossman et al. 1990; Yarborough 2006). Others argue that although the link may be weaker there is nevertheless an observable association between chrysotile and mesothelioma (Joshi and Gupta 2005; LaDou 2004; Landrigan et al. 1999; WHO 2006).
Even if chrysotile is safer this is not necessarily synonymous with safe, but the future of the global asbestos industry now hinges on the “chrysotile defense” (McCulloch and Tweedale 2008:119). It is the latest turn in the scientific and political contestation over asbestos that has been ongoing for over a century.
Conclusion
Cumulative deaths due to asbestos are estimated to exceed five million and could reach ten million given current rates of consumption (Castleman 2005; LaDou 2004). More than 50 countries have banned or restricted asbestos use (Kazan-Allen 2013). Further, the ILO and WHO have adopted resolutions defining all types of asbestos as carcinogenic and calling for a global ban (Takala 2002; WHO 2006). And yet, the worldwide production of asbestos remains substantial.
The present study illustrates that as asbestos consumption over the period 1960–2011 rose and then declined precipitously in the industrialized countries its presence increased dramatically in the developing countries. In the wake of experiential and scientific documentation of its deleterious effects the industry reorganized and rebounded. Indeed, more than half of the asbestos fiber consumed during the twentieth century occurred after 1975 (Virta 2006)—a period in which the effects on human health were already voluminously documented (McCulloch and Tweedale 2008). The United States, and other industrialized countries, are still confronting the legacy of asbestos-related disease, and the material remains imbedded within the built environment (Bowker 2003; Brodeur 1985). This includes asbestos-contaminated insulation that remains within millions of American homes (Bowker 2003). The global revitalization of asbestos production, moreover, also presents numerous challenges in terms of occupational and environmental health in the developing countries. It has the potential to prefigure a significant expansion of asbestos-related disease into the twenty-first century (McCulloch and Tweedale 2008).
The rhetoric of denial has long constituted a key strategy employed to inhibit regulation. As McCulloch and Tweedale (2008:275) note, “The most striking feature of the asbestos tragedy—and the most poignant—is that there has never been any shortage of information.” The industry excels at manufacturing uncertainty, however, where none plausibly exists. Denial is arguably often employed by organizations confronting resistance to their production of occupational and environmental contaminants. Cohen's (1996, 2001) typology not only characterizes the history of asbestos but is an important framework salient to future research concerned with a number of environmental justice issues.
The history of asbestos is another example illustrating, as Rosner and Markowitz observe (1991), that popular and professional recognition of industrial disease is not simply the consequence of advances in medical research and knowledge but also broader social, political, and economic forces. Asbestos is also another example highlighting that the environmental justice movement must confront the dynamics shaping the transnational movement of occupational and environmental contaminants (Faber 2008; Pellow 2007). It is but one hazard regulated within a majority of industrialized countries only to reappear elsewhere in the global economy. But asbestos, as LaDou (2004) notes, is now one of the most ubiquitous contaminants in the world.
Alleman and Mossman (1997) suggest efforts to eradicate asbestos use are misguided as projected future rates of asbestos-related mortality are lower than other prominent risks, particularly smoking and drug and alcohol abuse. This is a notable critique but confronting asbestos-related disease does not necessarily preclude meaningful social action directed towards addressing other pressing social and environmental problems nor are the estimated 90,000–100,000 asbestos-related deaths worldwide each year (Takala 2002; WHO 2006) a non-significant occurrence.
Today, asbestos is primarily utilized in cement construction materials where it is included as an inexpensive filler to increase tensile strength (Virta 2005, 2006). And while the asbestos industry in Canada, Russia, Brazil, and elsewhere continues to assert chrysotile can be used safely under controlled use conditions the norm in the developing countries is primarily the uncontrolled use of asbestos in manufacturing and construction, irrespective of prevailing laws and regulations (Castleman 2005). The promotion of chrysotile includes industry sponsored conferences, the generation of printed materials extolling the virtues of chrysotile, as well as unilateral lobbying with developing country governments.6 According to a study by the British Broadcasting Corporation (BBC) and the International Consortium of Investigative Journalists (ICIJ), since the mid-1980s a global assemblage of pro-industry organizations and trade associations has invested $100 million in public and private money to expand the market for chrysotile and chrysotile-based products (ICIJ 2010). Arguably, this effort is misguided as there is now an array of commercially available materials that are viable substitutes for asbestos (Castleman 2005; Harrison et al. 1999; Landrigan et al. 1999), although generally more economically expensive.
The relative weighing of the costs and benefits of asbestos has for too long focused on its short-term advantages as a cheap and durable construction material but insufficiently considered the long-term effects on human health. And public health resources are typically devoted to “downstream” issues or in reference to problem-solving interventions designed to address various, and shifting, concerns (McKinlay 1981). The more enduring problems, however, exist “upstream” in terms of the social context in which segments of a population are characterized by differential exposure to risk (McKinlay 1981). The challenge, then, is to better recognize the manner in which “societies shape patterns of disease” (Link and Phelan 1996: 471).
The environmental justice movement has arguably contributed to greater recognition of the upstream and disproportionate, inequitable exposure to occupational and environmental risks confronting particular segments of a population. The global reorganization and revitalization of asbestos, however, illustrates the enduring struggles that persist, even in the context of observable, repeated deleterious effects on human health and well-being.
Footnotes
Author Disclosure Statement
The author has no conflicts of interest or financial ties to disclose.
Appendix
| Developed (N=28) | Chile | Namibia |
| Australia | China | Nepal |
| Austria | Colombia | Nicaragua |
| Belgium | Congo, Dem. Republic | Niger |
| Canada | Costa Rica | Nigeria |
| Denmark | Croatia | Oman |
| Finland | Cuba | Pakistan |
| France | Czech Republic | Panama |
| Germany | Dominican Republic | Paraguay |
| Greece | Ecuador | Peru |
| Iceland | Egypt | Philippines |
| Ireland | El Salvador | Poland |
| Israel | Estonia | Romania |
| Italy | Georgia | Russia |
| Japan | Germany, East | Saudi Arabia |
| Korea, South | Ghana | Senegal |
| Kuwait | Guatemala | Serbia & Montenegro |
| Netherlands | Guinea | Sierra Leone |
| New Zealand | Haiti | Slovakia |
| Norway | Honduras | South Africa |
| Portugal | Hungary | Soviet Union |
| Portugal | India | Sri Lanka |
| Slovenia | Indonesia | Sudan |
| Spain | Iran | Swaziland |
| Sweden | Iraq | Syria |
| Switzerland | Jamaica | Tajikistan |
| United Arab Emirates | Kazakhstan | Tanzania |
| United Kingdom | Kenya | Thailand |
| United States | Korea, North | Togo |
| Developing (N=100) | Kyrgyzstan | Tunisia |
| Albania | Latvia | Turkey |
| Algeria | Lebanon | Turkmenistan |
| Angola | Libya | Uganda |
| Argentina | Lithuania | Ukraine |
| Azerbaijan | Macedonia | Uruguay |
| Bangladesh | Malawi | Uzbekistan |
| Belarus | Malaysia | Venezuela |
| Benin | Mauritius | Vietnam |
| Bolivia | Mexico | Yemen |
| Bosnia & Herzegovina | Moldova | Yugoslavia |
| Botswana | Mongolia | Zambia |
| Brazil | Morocco | Zimbabwe |
| Bulgaria | Mozambique | |
| Burundi | Myanmar |
Designation based on gross national income per capita (US$) in 2005 as indicated by the World Bank (2006). “Developed” includes all countries designated as high income. “Developing” includes low, lower middle, and upper middle income countries.