
Abstract
Abstract
There are significant disparities in asthma prevalence and management in New York City (NYC). Children living in the low income, largely minority neighborhood of East Harlem are almost 13 times more likely to have an asthma related emergency department visit compared to children on the Upper East Side, an adjacent high income neighborhood. The disparities in asthma prevalence and control are in part attributable to environmental conditions, including housing, which in low-income communities is often poorly maintained, resulting in mold, pests, and other asthma triggers. Controlling Asthma through Home Remediation (CAHR), a program of LSA Family Health Service (LSAFHS), offers remediation and repair, training, and comprehensive case management to East Harlem families that have children with severe and/or persistent asthma and live in NYC Housing Authority (NYCHA) public housing. Preliminary findings, based on pre-post assessments of 60 CAHR children, include statistically significant reductions in nighttime awakenings, emergency department visits, and rescue medication use. There were reductions in daytime asthma symptoms and improvements in household conditions; however, they were not statistically significant. Recognizing the limited reach of individual level services, LSAFHS also advocates for system-wide changes across NYCHA. Citing the Americans with Disabilities Act and its relevance to individuals with asthma, LSAFHS, in partnership with other community-based organizations and public interest attorneys, reached a settlement with NYCHA in 2013 that resulted in policy changes mandating expedited repairs of leaks, mold, and related issues. Monitoring the impact of these changes is ongoing. A hope is for replication of advocacy efforts in other cities.
Introduction
T
The disparities in asthma prevalence and control are in part attributable to indoor and outdoor environmental conditions in low income and minority communities. 7 Housing in low-income communities—including public housing 8 —is often poorly maintained, resulting in mold, pest infestations, and the presence of other asthma triggers. 9 Programs that offer services to ameliorate household environmental conditions, including integrated pest management, cleaning, and home repair to reduce moisture, have shown promising results with respect to reduced asthma symptoms and reduced healthcare use. 10
East Harlem, the target community for the program described in this article, is among NYC's most disadvantaged communities: 31% of the population is living in poverty 11 and 33% of adults do not have a high school diploma. 12 Half of East Harlem residents are Latino and approximately one-third (36%) are black. 13 There are 14,700 public housing units in East Harlem, 14 which represents 33% of the housing in the neighborhood and the highest concentration of public housing in NYC. 15 Federal, state, and city funding for the NYC Housing Authority (NYCHA), which operates NYC's public housing, has been insufficient, leading to increasing annual deficits, service and staff cuts, as well as cancellation of capital improvements. 16 Maintenance is often problematic in NYCHA buildings and pest infestation is common, 17 with research reporting cockroaches in 77% of NYCHA apartments surveyed and evidence of mice in 13%. 18
The Intervention
Overview of direct services
LSA Family Health Service (LSAFHS) has provided home-based environmental services to East Harlem families with children with severe and/or persistent asthma for 16 years. Implemented by community health workers (CHWs) trained in environmental health, these services focus on improved indoor air quality and sustained elimination of household environmental conditions, such as mold, dust, and pest infestations that exacerbate asthma symptoms. Controlling Asthma through Home Remediation (CAHR), a U.S. Department of Housing and Urban Development (HUD) funded demonstration program of LSAFHS, focuses on East Harlem families living in NYCHA housing, offering remediation, education, advocacy, skill building, and hands on experience, with the goal of empowering parents and other caregivers to maintain a household environment with reduced asthma triggers.
Recruitment and eligibility
Families self-referred to CAHR and were recruited through other LSAFHS programs and through community organizations, including Head Start programs, local schools (e.g., through parent coordinators, nurses), the NYC Department of Health and Mental Hygiene, and area medical providers. Families were eligible for participation in the program if they met the following criteria:
• Residence in East Harlem public housing; • Child (age 17 or under) with severe or persistent asthma defined by one of the following over the last year, as reported by the primary caregiver: a) daytime symptoms or use of rescue medications (e.g., Albuterol) for symptom control three or more days per week; b) nighttime awakening three or more nights per month; c) two or more treatment episodes with oral steroids; d) one or more asthma related hospitalizations; e) two or more emergency department visits; • Environmental hazards documented by a CHW: a) pest infestation (e.g., observed cockroaches or rodents, or evidence of their activity); b) mold, excess moisture, and/or leaks (observed by a CHW or documented by a moisture meter); or c) poor ventilation (defined by number and placement of operable windows and/or working ventilation system).
Intervention activities
The intervention began with a comprehensive in-home health and housing assessment documenting the severity of the child's asthma and the presence of household triggers. The comprehensive assessment provided baseline data for the evaluation (as described below) and for treatment planning and service delivery, including identification of immediate health and safety risks. Consistent with recommendations regarding integrated environmental services, assessments considered a range of health and safety risks. However, the main focus was on the identification of common household asthma triggers including: infestation of cockroaches, rodents, and dust mites; poor indoor air quality resulting from cigarette smoke and/or inadequate air ventilation; mold; structural problems including holes in walls, peeling paint, and crumbling plaster; inadequate household hygiene, including clutter; household chemicals, including harsh cleaning products and pesticides; pets; and stuffed toys.
Upon completion of the initial home assessment, the CHWs developed an individualized remediation plan to address health hazards and to define the work needed to ameliorate them. At least one member of the household received hands-on training focused on recognition and safe elimination of household hazards; other family members received more general information. Specific intervention and training activities included: integrated pest management (IPM) services; specialized cleaning; reduction in mold conditions, including fungicidal protective coating where appropriate; education regarding reduced exposure to second-hand smoke; referrals to outside environmental investigators/technologists; and referrals to medical case management and appropriate social service programs. Recognizing that some low-income families may lack the resources to buy the supplies and equipment needed to sustain environmental improvements, CAHR offered equipment loans, including HEPA-filtered vacuums and air cleaners, as well as free dust mite proof mattresses, box springs, and pillow covers; exhaust fans and/or air cleaners; cleaning supplies; and food storage containers. In addition, if housing repairs were beyond the capacity of the CHWs, they assisted families with filing complaints with the appropriate NYCHA offices and advocating for repairs, including accompanying residents to meetings with NYCHA management officials.
The majority (approximately 80%) of intervention services were provided within three months of the initial assessment; however, participating households were visited and re-assessed at six and twelve months, so as to reinforce training provided, address issues that may have arisen, and gather data needed to assess the durability of effects.
Evaluation
Design
CAHR direct services are being evaluated by the New York Academy of Medicine (NYAM) using a mixed-method pre-post design that focuses on household environmental conditions, child health status and health care use, and caregiver comfort with management of his/her child's asthma. Data are collected for the evaluation using baseline and follow-up caregiver surveys, caregiver qualitative interviews (with a limited sample), and CHW observation of housing conditions. Specific domains and measures include but are not limited to:
• Sociodemographics: child's age, gender, race/ethnicity, caregiver education, household composition • Health and health care use: days with asthma symptoms, nighttime awakenings due to asthma symptoms, days rescue medications used, hospitalizations and emergency room (ER) or urgent care visits for asthma symptoms, missed school, caregiver missed work • Household conditions: dust on surfaces, household clutter, mold, mice and cockroaches • Caregiver concern and confidence regarding child's asthma control
The evaluation protocol was approved by the NYAM Institutional Review Board. Parents of enrolled children provided informed consent and received $20 for completion of each baseline assessment, follow-up assessment, and qualitative interview.
Statistical methods
Descriptive statistics were generated to characterize the demographic characteristics of enrolled children and their caregivers at baseline. Because our analysis includes only those children for whom annual follow-up data are available, we assessed for retention bias by comparing characteristics of this group to characteristics of the larger group of children enrolled for at least 10 months using chi square and student's t-tests for categorical and continuous variables, respectively. After dichotomizing ratings of household conditions (moderate or severe versus mild or none), we assessed changes in CHW ratings of household conditions from baseline to one year using McNemar's test. For health indicators, the Wilcoxon matched-pair signed rank test was used for analysis of absolute change in number of occurrences.
Statistical significance was based on a threshold of p < 0.05. All data management and analyses were conducted using SAS version 9.3 (Cary, NC).
Evaluation findings to date
LSAFHS enrolled 152 children into the CAHR program. At the time of writing, 116 had been enrolled for a minimum of 10 months and were therefore eligible for an annual follow-up assessment (conducted 10–15 months post baseline). Of these, annual follow-up assessments had been completed for 60 children (52%), representing 41 households (see Table 1 for demographic characteristics of the full sample and those with annual follow-up assessments). The majority of children without follow-up assessments are near the beginning of the 10–15 month window at the time of writing; the follow-up rate is, therefore, expected to increase significantly. To date, qualitative interviews have been competed by 12 caregivers.
As of September 30, 2014.
Slightly over half (51.32%) of enrolled children were boys; the mean age was 8.34 years. They were primarily African American (34.87%) or Latino (48.68%). Close to 40% of caregivers had not graduated from high school. The average household size was 4.93. Approximately 17% of households lived on the first floor of their buildings, and 18.42% lived on the top floor—suggesting specific maintenance issues at these locations. African American participants enrolled for at least 10 months were more likely to complete the annual follow-up than were Latinos. Otherwise, the groups were similar (data not shown).
At baseline, most households had moderate to severe cockroach infestations (60.98%) and household clutter (60.98%); dust, mold, and mice were less common (43.90%, 43.90%, and 26.83%, respectively). At the annual follow-up assessment there was a statistically significant improvement in evidence of clutter. There were observable improvements in other conditions, although they were not statistically significant (see Figure 1). There were a number of improvements in health indicators at the annual follow-up assessment, including decreased nighttime awakening, use of rescue medication, prescribed oral steroids, and asthma-related emergency department or urgent care visits (all p < 0.001) (see Table 2).
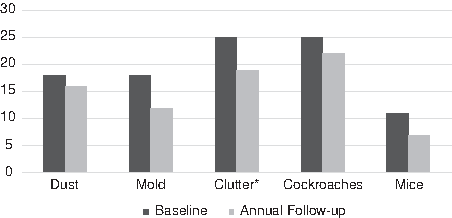
Number of households with moderate or severe conditions observed by community health worker (n = 41). *p < .05 in analysis using McNemar's test.
Based on Wilcoxon matched-pairsigned rank test. SD, standard deviation; ER, emergency room.
Results from qualitative interviews were consistent with survey findings; caregivers described decreased asthma symptoms and improved housing conditions. In addition, participants described improved knowledge of asthma triggers and cleaning practices.
I learned about using different detergents so it won't trigger the asthma. I stopped using the air fresheners. (mother of a 10-year-old)
I had a leak in my bedroom. [The CAHR staff] noticed that there was some mold, and they were able to scrape the painting off in my bedroom closet, and they fixed that. As far as my bathroom, they noticed some mold. They were able to get the Housing people to come in and paint over it. They were really helpful with certain things, especially when it came to my kids, because my son has severe asthma. (mother of a 5-year-old)
They expressed satisfaction with the program and appreciation of CHW efforts:
I was naïve when I started the program and I actually didn't want it. I was more like, you know, “That's a waste of my time, just people in my life.” But I'm glad it happened, you know. I grew up, I realized that this was something that was worth it, and it's such great people to have. It really is. They really work hard, they help you, and they get the job done. (mother of a 6-year-old)
Advocacy
In addition to its direct services to enrolled families, CAHR staff—working in collaboration with affected families—address the need for systemic change in regulation, enforcement, and funding related to housing maintenance and repair through advocacy aimed at improved policies and practices across NYCHA developments.
These activities are consistent with LSAFHS's overall mission to provide opportunities for enhancing self-esteem, knowledge, socialization, and community-building; to increase understanding of the root causes of poverty; and to advocate for social justice.
Since 2001, LSAFHS has worked with Manhattan Together, a part of the Metro Industrial Areas Fund (IAF), a community organizing group representing local networks of faith and community-based organizations, to address housing conditions in NYCHA— at a systemic level—that remained unresolved despite the remediation efforts feasible through CAHR and resident complaints to the Housing Authority. This advocacy has addressed egregious and unsafe conditions within apartments (e.g., leaks resulting from structural issues, faulty ventilation, pest infestation), in the common areas of buildings (e.g., broken elevators), and on public housing grounds and bordering streets.
Early advocacy efforts involved the compilation of extensive complaint lists and quarterly meetings with NYCHA maintenance officials. This process expedited the repair of hundreds of apartments and resulted in system-wide changes, including the development of a call center that facilitated a significantly more efficient and effective system for scheduling and completing repairs. However, there were diminishing returns over time, suggesting the need for a new approach. CAHR staff and Manhattan Together members began to meet with attorneys from the Natural Resources Defense Council (NRDC) and the National Center for Law and Economic Justice (NCLEJ).
NRDC and NCLEJ filed a legal complaint against NYCHA, employing the Americans with Disability Act (ADA), which includes protection for people with asthma and breathing disabilities. The complaint alleged that NYCHA was violating the civil rights of people with these conditions, utilizing a legal strategy that had not been pursued in federal court previously. The complaint focused on leaks, excessive moisture, ventilation issues, and mold, because the scientific literature clearly connected damp indoor spaces and mold to the aggravation of asthma symptoms. 19 (See Figure 2 for photographs of NYCHA apartments.)

Housing conditions prior to intervention.
By the fall of 2012, NRDC and NCLEJ enlisted a certified industrial hygienist to assess apartments and provide recommendations that could be used in a Request for Accommodation. NYCHA tenant files were requested, many interviews were conducted, and the tenants' doctors were contacted to provide letters describing their health conditions. In December 2012, a press conference was held and Requests for Accommodation were announced on behalf of six NYCHA tenants whose uncorrected conditions jeopardized their health. 20 In December 2013, the coalition had reached an agreement with NYCHA to settle the ADA claim. In April 2014, the United States District Court for the Southern District of New York approved the negotiated class action settlement in Baez v. New York City Housing Authority (No. 13 CIV 8916). 21
The basic terms of the settlement are that: 1) the plaintiffs named in the claim will represent the class of people living in NYCHA with asthma, 2) NYCHA will implement a new mold and moisture policy with specific timetables, 3) NYCHA will modify its forms and informational materials related to disabilities and mold to better inform residents of their rights and of NYCHA procedures, 4) NYCHA will periodically report to the NRDC and NCLEJ its progress on eliminating mold and moisture, and 5) the court will enforce the settlement for at least 30 months. NYCHA must also have supervisors inspect mold and moisture work, train NYCHA staff on the new policies, and develop a pilot to use moisture meters or other devices to identify leaks in walls.
Because the new mold policy applies to all buildings, the settlement affects all NYCHA residents (a number exceeding 400,000), whether or not they have asthma. The new policy commits NYCHA to abate flooding within 24 hours, dry standing water within 48 hours, fix simple repairs (i.e., repairs that can be done by a maintenance worker such as unclogging vents, fixing windows, and fixing simple sink leaks) within seven days, and fix complex repairs within 15 days (i.e., repairs that require specialized trade workers to trace the source of a leak in the walls of multiple apartments). Residents with asthma will have a variety of ways to inform NYCHA about their health. If they want to request an accommodation, they are required to provide letters from a physician describing the condition. Examples of reasonable accommodation include the right to use supplemental air conditioning, a temporary relocation during repairs, or a permanent transfer if the repair requires a capital improvement.
Discussion
The CAHR approach is distinct from common asthma intervention models focused on the household environment in its broad and holistic approach, offering both education and remediation to engaged families, as well advocacy to affect conditions at the level of the building and the Housing Authority. Preliminary evaluation data for the family-level interventions are promising, in that they show significantly reduced nighttime awakenings, medication use, emergency care, and hospitalizations. Fewer daytime awakenings and absences from school were also reported, although the differences were not statistically significant. Though the sample size for the qualitative interviews remains small (n = 12, to date), findings are consistent with the assessment data and suggest changes in knowledge, behavior, and housing conditions, resulting from intervention activities.
The unprecedented success of the legal action is noteworthy. Health care providers rarely have the time or expertise for legal recourse, but their intimate knowledge of issues facing low income and minority populations, as well as the trust built with their clients, may make them ideal partners in such efforts. The collective effort could not have been achieved without the support and advice of experienced community organizers, volunteer leaders, and the relationships that Metro IAF developed over the years with the media and with public interest law firms, such as NRDC.
A number of limitations regarding findings reported should be mentioned. The evaluation data is preliminary and represents outcomes from just a portion of the enrolled families. In addition, findings regarding housing conditions are self-reported and/or based on observational data, rather than more objective measures of environmental conditions. Findings regarding health and health care use among enrolled children are also based on self-report and may be affected by factors that were not clearly addressed in the evaluation, such as a change in medications or medical services. Finally, the implications of the settlement with NYCHA are not yet known, as practice change often lags significantly behind policy change—particularly when financial resources are scarce. For Baez v. NYCHA to be a success, tenants and the organizations that work with them need to monitor implementation and hold the Housing Authority accountable.
Conclusion
There is significant evidence regarding the effectiveness of household interventions, including remediation and integrated pest management, on childhood asthma control. However, questions remain regarding intervention model and components most likely to lead to sustained improvements. In addition, there is a need for greater reach, as the population level impact of family-focused interventions is likely inadequate. Combining direct services with advocacy, as in the CAHR model, facilitates change at multiple levels and expanded impact. Such efforts require the collaboration of CHWs, community organizers, and advocates, as well as tenants willing to testify to the inadequacies in their household environment.
Going forward, it is important to document outcomes—including those sustained over time—in family focused interventions, so that the most effective models may be promulgated. Monitoring and evaluation of policy changes, like those adapted by NYCHA, is also key to ensure that implementation and impact are consistent with objectives of the settlement.
Footnotes
Acknowledgments
CAHR was funded by a grant from the U.S. Department of Housing and Urban Development. We greatly appreciate their support. We would like to thank CAHR participants for their engagement in this effort. We would also like to thank our HUD Program Officer, J. Kofi Berko PhD, as well as the members of our advisory board, all of whom provided invaluable guidance, David Evans PhD, Rachel Mane MSW, and Randall Sell ScD.
Author Disclosure Statement
The authors have no known conflicts of interest or financial ties to disclose.