
Abstract
Abstract
Starting in the 2000s, the U.S. energy system entered a period of rapid transition, with a marked decline in coal extraction, a boom in domestic oil and gas production, and increased deployment of renewable sources. Economically marginalized rural populations tend to have less access to health services than their metropolitan counterparts and stand to make significant gains from this energy transition. However, during the 2010–2015 period, several rural hospitals closed. In this analysis, we ask how the energy transition effects the likelihood of rural hospital closure. Models suggest that expanding energy production does not reduce the chances of a hospital closure, raising important questions of energy justice.
Introduction
R
Historically, rural populations were typically healthier than urban populations. 6 , 7 By the 1980s, a rural mortality penalty emerged, wherein rural residents typically had shorter lifespans than their urban and suburban counterparts 8 , 9 , 10 , 11 —this gap is more pronounced for rural areas that specialize in resource extraction. 12 , 13 More troublingly, recent research documents declining life expectancy among whites without a college education, especially those in rural areas that had shed manufacturing employment. 14 , 15 Rural hospital closure may exacerbate these trends, as residents may have longer commutes for care 16 and hospital closure may increase poverty and reduce income in the host community, 17 , 18 in addition to deleterious health impacts. Indeed, many rural areas of the United States are classified as health professional shortage areas, wherein there is a lack of needed medical professional and facilities. 19 , 20
Although the reasons for these regional divergences are complex, a central challenge facing rural areas is the provision of health services. Indeed, 105 rural hospitals closed from 2005 to 2015. 21 Rural hospital closures between 2013 and 2014 have left 1.7 million people without access to acute medical services. 22 Hospitals that serve low-income rural areas are at greater risks of closure. 23
The purpose of this article is to understand how shifts in traditional rural livelihoods wrought by the ongoing energy transition have affected rural hospital closure. In doing so, we ask how the growth of unconventional oil and gas, wind power, and the decline in the coal sector from 2000 to 2010 impacted rural hospital closure from 2010 to 2015, using county-level data. As such, this analysis is a response to Healy and Barry's recent call to investigate the “upstream” energy justice implications of the energy transition. 24 The next section describes our data and analysis.
Data, Measures, and Methods
Dependent variables
Our dependent variable is a binary indicator of whether a county experienced a rural hospital closure from 2010 to 2015—these data are compiled by the Sheps Center for Health Services Research at the University of North Carolina. 25 For our purposes, a hospital is counted as closed if it has ended in-patient services. Some of the closed hospitals may still offer some outpatient or long-term services. We link hospital closures to their host county for our unit of analysis, counties are a common unit of account in geographic and administrative data. Only one county—Gibson County, GA—had two hospital closures. Given that all other counties had only a single closure (or no closure at all), our dependent variable is a binary indicator wherein counties that experienced a hospital closure are coded as “1” and others are scored as “0.” Figure 1 displays the spatial distribution of rural counties with a hospital closure.
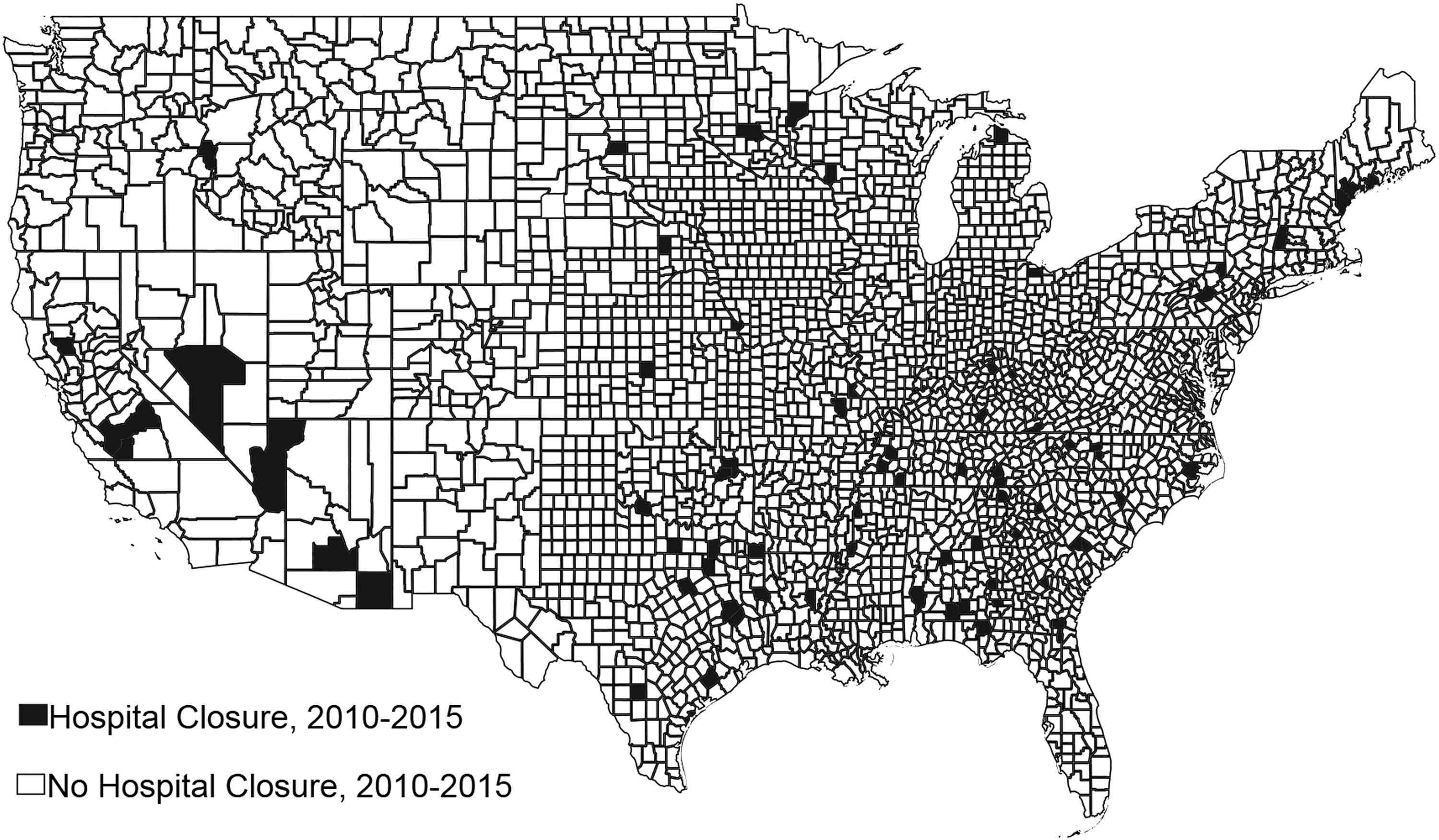
Rural hospital closures in the contiguous United States, 2010–2015. Created with Stata/IC 15. Source: Sheps Center at the University of North Carolina.
Predictors
Energy production
We rely on the U.S. Dairy Association (USDA's) comprehensive, national oil and gas production data set from the USDA's Economic Research Service (USDA ERS). 26 This county-level data set covers the 2000–2011 period, the period wherein unconventional oil and gas extraction methods created a boom in domestic production. We expect some degree of temporal lag between the oil and gas boom and rural hospital closure. That is, it is unlikely that a sudden boom in production will create the conditions to allow a rural hospital to continue operations. However, it is plausible that long-run oil and gas production might generate the conditions—population growth, tax revenue, and economic development—that might make hospital closure less likely.
Both oil and gas production are extremely skewed. Only one-third of all counties had oil or gas production during the 2000–2011 period, meaning that most counties have a score of 0 on both variables. A common method to correct skewed variables is log transformation, but this method results in missing data when predictors have a true zero. To address this problem and avoid dropping cases, we took the square root of both variables and implemented a method described by Hosmer and Lemeshow by creating binary variables to indicate whether a county had oil and gas production. 27 That is, our models include both a square root transformed interval-level predictor for oil and gas production and a binary indicator of whether the county hosted any oil and gas production.
For wind energy, we accessed a shape file developed by U.S. Geological Service researchers. 28 From this shape file, we used the geoinpoly user-written program in Stata 15 29 to generate a count of active wind turbines within the borders of each county from 2000 to 2010. A limitation of these data is that, for about 9% of turbines, the year that it became active is unknown. We assumed that these turbines were active over the 2000–2010 period, although it is possible some came online after 2010. We suspect, but cannot confirm, that missing or inaccurate data are probably more common in the older regions of the data set because it was constructed from historical documents. As with other predictors, this variable was extremely skewed—56% of counties did not host any wind turbines, whereas some counties had thousands. We again took the square root of this variable and created a binary variable for counties that had wind turbines and those that did not. Both the binary indicator and the square rooted count are included in our regression models described hereunder.
As we noted previously, the ongoing transitions in the U.S. energy system have led to a significant decline in the coal sector, a traditional economic livelihood in parts of the rural United States. We accessed data from the Energy Information Agency to identify counties that had experienced the shuttering of a coal mine from 2000 to 2010. 30 For our purpose, any mine that went from active status (e.g., producing coal and workers employed) and transitioned to nonproducing is counted as “closed.” We use a binary indicator wherein 0 represents county did not experience a coal mine closure and 1 represents mine closure. Descriptive statistics for all variables are displayed in Table 1.
Note: BEA, Bureau of Economic Analysis; EIA, Energy Information Agency; SD, standard deviation; sqrt, square root; USDA ERS, U.S. Dairy Association Economic Research Service.
Controls
The 2010 Affordable Care Act (ACA) is the most consequential change in healthcare policy in recent U.S. history. Importantly, the ACA expanded Medicaid coverage for low-income families, causing an economic infusion into underserved rural areas. Thus, we include a binary indicator for whether a state expanded Medicaid coverage as part of the ACA. We include poverty rates, median income, and average earnings per job, population (measured in 1000s of persons), and population density (1000s of persons per square mile), all averaged over the 2000–2010 period. These data were provided by the USDA ERS and Bureau of Economic Analysis, respectively. 31 , 32
Analysis
After merging the data described previously, our final data set contains 2922 counties throughout the contiguous United States. Given the binary nature (and spare distribution) of our dependent variable, we employ logistic regression through the firth logistic estimator. This estimator produces less biased parameter estimates than the standard logistic regression estimator when data are sparsely distributed. 33 , 34 We complement the firth logistic model with a spatially lagged linear probability model (LPM) and decompose these effects into their direct and spill-over components.
Firth logistic models
In Table 2 we provide log-odds coefficients, standard errors, and model fit diagnostics for our firth logistic models. The model includes all energy production variables, as well as county socioeconomic variables and our indicator of Medicaid expansion. Energy production appears to have mostly null effects on the likelihood of hospital closure—oil production, gas production, and coal mine closure do not approach statistical significance. The lone exception is wind power—as the number of wind turbines within 100 miles of a county centroid increases, that county is less likely to experience a hospital level closure. Counties with greater population density are more likely to have a closure, and counties in states that expanded Medicaid coverage are more likely to retain their hospitals. In model 2, we dropped the predictors that were not statistically significant in model 1. Although the coefficients for the retained predictors are roughly similar, the model fit statistics (i.e., Akaike information criterion, Bayesian Information Criteria, and McKelvey and Zavoina R2) have all been damaged, suggesting that the excluded predictors did somewhat improve model fit.
Note: *p < 0.05; **p < 0.01, All continuous predictors are county averages from 2000 to 2010.
AIC, Akaike information criterion; BIC, Bayesian Information Criteria; SE, standard error.
Spatial linear probability model
Direct, spill-over, and total effects derived from the spatial LPM are displayed in Table 3. This model uses a spatial contiguity matrix that assumes a first-order spatial autocorrelation in the error term and allows for neighboring counties (whether sharing a border or vertex) to influence one another. In general, this model has reproduced the null results of the firth logistic model—none of our energy production variables reach statistical significance, and all have substantively small coefficients. As population density increases, a hospital closure becomes slightly more likely and rural hospitals are more likely to survive in states that expanded Medicaid coverage.
Note: n = 2922. Model uses a contiguity matrix that assumes that neighboring counties influence each other and the error term has first order spatial autocorrelation. p < 0.01, All continuous predictors are county averages from 2000 to 2010.
Robustness checks and diagnostics
After estimating our models, we performed a series of robustness checks. First, we implemented alternative transformations of oil and gas production, including a cube root transformation and splitting each variable into quartiles. These new variables produced similar null results. We also reran our models for subset of counties based on the rural–urban continuum codes provided by the USDA ERS. 35 The modest to null effects of energy production were reproduced, even when excluding urban counties. Multicollinearity was assessed through variance inflation factors, none of which exceeded 4, indicating that multicollinearity is not a problem in our models.
Discussion
The consequences of the ongoing energy transition for the health and well-being of rural communities are not fully understood, despite claims that alternative energy sources and unconventional oil and gas will be a boon for these communities. In this article, we considered the problem of rural hospital closure and asked how the energy transition is linked to rural hospital closure using county-level data. As such, we examine the upstream energy justice impacts of energy transition on rural areas. We find very limited evidence that changes in energy production have a substantively important impact on the likelihood of rural hospital closure.
These results reveal two important implications for upstream energy justice in economically marginalized rural areas. Considering unconventional oil and gas extraction, several articles suggest that it does increase modestly earnings and reduce poverty in host communities. 36 , 37 Still, unconventional oil and gas extraction may not address more structural problems—such as the availability of health services—in these areas. One possible reason for the null effect of unconventional oil and gas extraction relates to the transient nature of the workforce. 38 Broadly, this research points to the need for rural communities undergoing oil and gas booms to implement policies to capture the economic windfalls of this new energy source. Furthermore, our models imply that the closure of coal mines does not necessarily damage the provision of health services in host communities. Counties that host coal mines tend to experience slower economic growth. 39 , 40 Hence, the loss of a coal mine may not translate into reduced health services as coal mining may be an economic detriment to communities. In sum, our analysis suggests that the oil and gas boom, the increasing deployment of renewable sources, and the decline of coal have not significantly altered the distribution of rural hospitals, suggesting that health services in rural areas are not benefitting from the energy transition.
Importantly, our models indicate that expansion of Medicaid under the ACA slowed the rate of hospital closures. In the end, federal policy and state policies may be more relevant for rural hospital viability than local economic conditions. Moving forward, we suggest that much more research is needed to understand the energy justice consequences of the current energy transition. Marginalized rural communities have historically provided the U.S. energy system with key raw material inputs and served as “sacrifice zones” to power urban and suburban areas. 41 , 42 Energy transitions can exacerbate, ameliorate, or alternatively perpetuate the well-being disparities between rural and metropolitan places.
Footnotes
Author Disclosure Statement
No competing financial interests exist.