
Abstract
Abstract
One out of every eight deaths globally is attributable to air pollution and these disproportionately ensue in high population density areas in lower income countries characterized by higher long-term levels of ambient pollution. Yet, our understanding of how population attributes and neighborhood effects jointly influence exposure to e-waste related air pollutants and disease symptoms is limited. Generalized linear models (logit, complementary log-log, negative log-log regressions) were fitted to cross-sectional survey data on 260 e-waste and non e-waste workers in Ghana to assess the relationship between self-reported eye problems, skin burns, breathing difficulty and coughing, and where e-waste workers jointly reside and work. Individuals who were neither e-waste workers nor resident in the contaminated work environment were 74% less likely to report eye problems compared with their counterparts who were resident non e-waste workers. Resident e-waste workers were 84% more likely to report skin burns compared with their counterparts who were resident non e-waste workers. Individuals who had attained tertiary education were 98% less likely to report skin burns compared with their counterparts without any formal education. Resident e-waste workers reported more breathing difficulty (odds ratio [OR] = 3.30, confidence interval [CI]: 1.733–6.267). Unlike gender, age groups were a significant predictor of coughing in both the biosocial and sociocultural models. Individuals in the 21–30 age group (OR = 3.46, CI: 1.717–6.981) likewise those in the 31–40 age group (OR = 3.51, CI: 1.738–7.088) were, respectively, more likely to report coughing compared with individuals below 20 years old, possibly due to longer term exposure. There is some cumulative health disadvantage to individuals who reside in the contaminated environment although they do not necessarily work there suggesting the need for national environmental health policy to target them.
Introduction
In the twenty first century, electrical and electronic waste (e-waste) has become an emerging global environmental health problem. 1 , 2 The United Nations Report 3 projected that by 2017 about 65 million tons of e-waste will be generated annually across the world. E-waste refers to the end-of-life electronic products, including televisions, monitors, computers, audio and stereo equipment, video cameras, fax/photocopy machines and printers, telephones, motherboards, mobile phones, chips, wireless devices, cathode ray tubes, and other peripheral items. 4 These contain harmful chemicals such as brominated flame retardants and classical toxic trace elements such as lead (Pb), Cadmium (Cd), Mercury (Hg), Arsenic (As), and Chromium (Cr). Furthermore, rare trace elements, including antimony (Sb), indium (In), and thallium (Tl), which have recently been a topic of concern because of their environmental, behavioral, and toxic effects, 5 are also present in e-waste.
E-waste recycling is a green industry of emerging importance, especially in low- and middle-income countries where much of this recycling work is performed and where many people's livelihoods depend on this line of work. 1 Significant amounts of e-waste have been exported to developing countries such as China, India, Pakistan, Vietnam, and the Philippines for recycling. 6 Recent restrictions on import and informal recycling of e-waste in Asian countries are expected to shift the e-waste flow further toward destinations in Africa, 7 including Ghana and Nigeria. In both countries, there are limited infrastructure and protocols to safely recycle and dispose of hazardous e-waste, and legislation dealing specifically with their flow and regulations for maintaining the environment and human health are not always effective. 8 , 9
One of the largest e-waste dumps in the world is located at Agbogbloshie in Accra, the capital of Ghana, where heaps of old computers and their accessories that are unusable are continually being dumped without any regard for the hazard that they pose to the environment and to the people living within the environs of the dump site.
E-waste workers at Agbogbloshie manually dismantle and openly burn e-waste materials to recover metals and other valuables contained in e-waste materials. Primitive methods (manual shredding and open burning) to remove plastic insulation from copper cables can release highly toxic chemicals and severely affect the environment and human health if improperly managed. 10 Brigden et al. 11 suggest that individuals working on and living near e-waste sites in Ghana could be exposed to toxic chemicals. In this context, there are many unprotected workers who are exposed to xenobiotics through inhalation, ingestion, and dermal contact, and also residents in the vicinity are at risk.
In contrast to numerous studies available on environmental pollution by e-waste related persistent compounds in developed countries, limited information on human exposure and medium-to-long term health effects in occupational settings is available in most developing countries such as Ghana. Few studies have evaluated disparities in adverse human health outcomes among e-waste workers who live and work in this contaminated environment. Even fewer studies have considered e-waste workers who work there but do not live in the polluted environment and other subgroups of similar demographic attributes who neither live nor work there. The foregoing indicates that the interplay between occupational and personal risk factors among e-waste workers and their non e-waste counterparts has hitherto not been adequately elucidated.
According to Schulte et al., 12 in evaluating occupational risk factors, personal risk factors are often considered as confounders or sources of bias and the full range of occupational risk factors and personal risk factors that affect the health of workers is hardly ever holistically studied. It is therefore necessary to assess whether self-reported adverse human health outcomes systematically varies with where these workers both work and live and whether compositional attributes of the population mediates or attenuates the effect (effect modification).
Schulte 13 and Loeppke 14 argue that finding effect modification is significant because inability to do so may culminate in misconstruction of exposure–disease relationships and to inefficiencies, including erroneous targeting, in developing interventions. Therefore, the first objective of this study was to evaluate whether occupational and residential status (resident e-waste workers, resident non e-waste workers, nonresident e-waste workers, nonresident non e-waste workers) jointly influence self-reported experiences of disease symptoms. The second objective was to assess how the relationships between occupational and residential status and reported disease symptoms were mediated or attenuated by population composition (biosocial and sociocultural attributes) of e-waste workers and their non e-waste counterparts. This observational study will potentially inform the enforcement of policy on environmental health and safety practices within the e-waste occupational setting in Ghana.
Risky Occupational Behavior and Risk Evaluation
Several theories have been proposed to explain how people evaluate risk and why they continually work in risky occupational environments. Understanding risk and how it is perceived is a crucial step toward creating programs and campaigns to raise awareness and make communities and workplaces safer. It has been suggested that factors that affect risk perception and tolerance can be categorized as macro-, meso-, or microlevel attributes. These levels refer to factors that are structural or institutional in nature (macro), at a peer-to-peer or community level (meso), or at an individual psychological level (micro). 15 , 16 Macrolevel theories of risk perception in occupational settings point to the need to go beyond mere psychological analyses of individual risk perception and take into account broader social, cultural, and environmental explanations of risk behavior. 17
Workers employed by an organization with a positive safety culture—an environment with high emphasis on safe work procedures and commitment to employee health and safety—were less likely to take risks than workers employed by an organization without a positive safety culture. 18
A related research study 19 found that workers exposed themselves to more risks and were less likely to comply with safety rules when they rated the safety climate of their organization poorly. At the meso-level, peer or community influences how people perceive and tolerate risk. 20 Less experienced e-waste workers may fail to wear personal protective equipment because they observe that their more experienced counterparts seldom wear personal protective equipment. In this context, Choudhry and Fang 20 observed similar effects of peer pressure in subcontracted workers who chose not to wear personal protective equipment to avoid teasing and harassment from coworkers. In such instances, both new and experienced workers may consider failure to wear personal protective equipment as acceptable or low risk. In addition, in workplaces, new employees may start taking unsafe shortcuts while performing job tasks because other more seasoned employees are doing so.16, 21
At the microlevel, an individual's level of knowledge regarding a situation influences the risk perception and risk tolerance. In this context, those who are less informed of a situation are less likely to take risks, while those with more knowledge are more likely to have higher levels of risk tolerance. 22 However, this refers only to the individual's own perception of knowledge, which may not be an actual objective assessment. For instance, Huang et al. 23 found that survey participants with a perceived higher knowledge of ecological hazards tended to have a higher risk tolerance for those hazards than those who professed to have little to no knowledge of ecological hazards. Workers in a chemical plant were opposed to wearing personal protective equipment because they believed that they already had an appropriate perception of risk. 24
The feeling of personal control over a situation can lessen anxiety and cause a worker to become more relaxed toward engaging in unsafe behaviors. 25 , 26 On the basis of the foregoing, understanding the subtle ways in which sociological and psychological forces interact to encourage or suppress risk-taking behavior could aid significantly in creating messages and programs to make communities and workplaces safer.
Hitherto, safety and health of workers in occupational settings were concerned merely with the prevention of occupational injuries and illnesses. Lately, however, its trajectory has shifted to a more holistic notion geared toward the overall protection of workers' health, the maintenance of their working capacity, and the improvement of the working environment in a manner that promotes safer and healthier workplaces. 27 , 28 Workplace inputs and outcomes are intrinsically linked. Therefore, workplace inputs (e.g., the use of rudimentary equipment and unsafe tools) that do not foster a congenial and safe working environment will necessarily affect the workplace outcomes (e.g., respiratory ill health and injuries).
The socioeconomic structure (nature and scope) of the e-waste economy, including demographic conditions, the industrial or service-oriented nature of markets, and the technological frontier, is an essential aspect for determining the state of workplace inputs and the exposure of different risk groups of employees to them. 27 Exposure to work-related risk factors is, in turn, one of the main determinants of health and safety outcomes, such as the absence behavior of employees (partly mediated by their job satisfaction), the incidence of work accidents, and the occurrence of occupational diseases. 29 , 30 The preceding provides the context within which this study should be understood.
Materials and Methods
Study area
The study area is the Agbogbloshie scrap yard, which is located along the banks of the Odaw River and the Korle Lagoon northwest of the Central Business District of the national capital between latitudes 5° 32′ 30″N and 5° 33′ 30″N and longitude 0° 13′ 30″W (Fig. 1). The Agbogbloshie scrap yard covers an expanse of about 6.2 hectares and has an estimated population of 40,000 inhabitants who are mainly Ghanaians and other foreign nationals from West Africa. The indigenous ethnic group within the city and the area is Ga; however, Oteng-Ababio 31 indicates that most of the inhabitants or workers within the area are migrants from the northern part of Ghana.
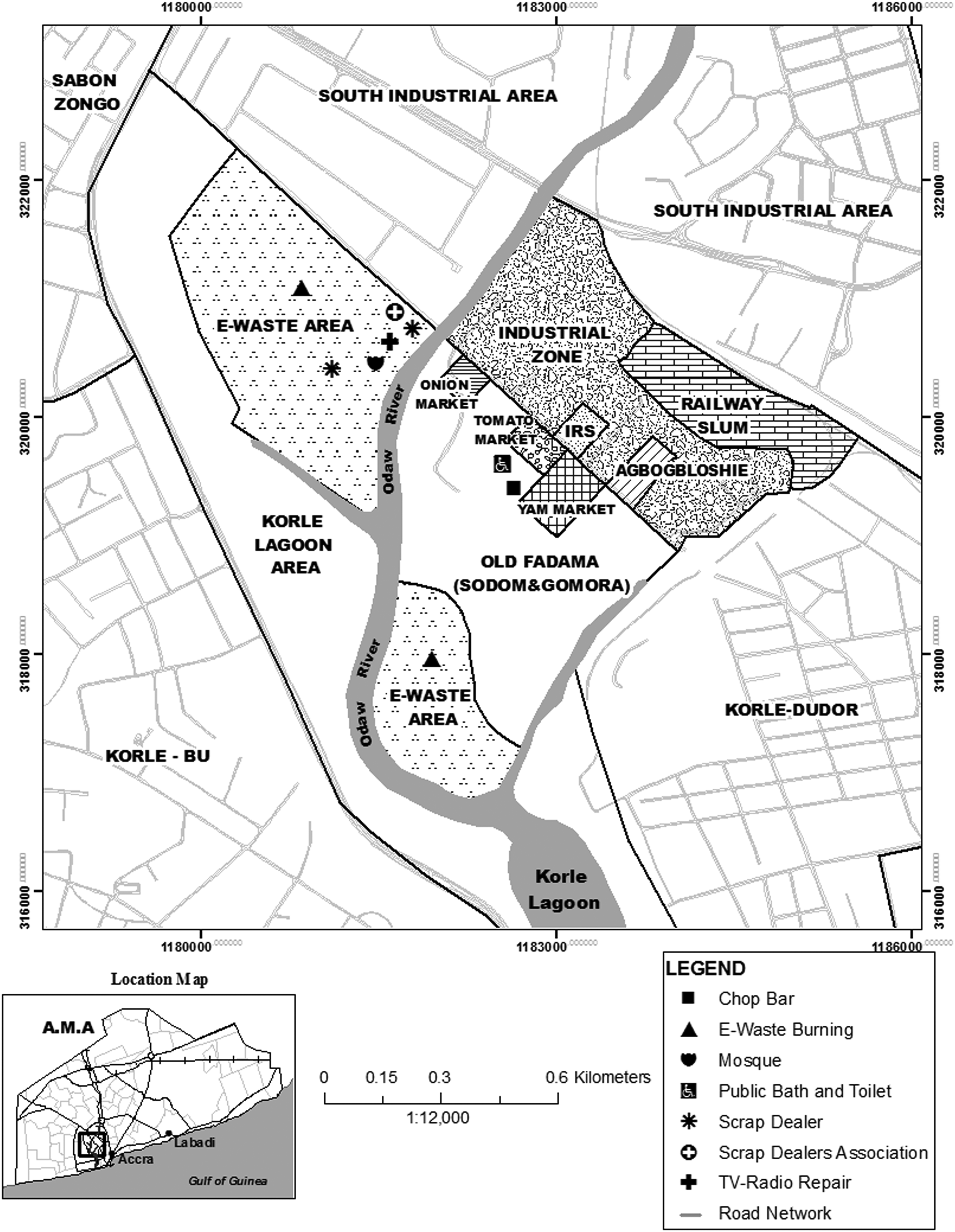
Map of Agbogbloshie, Ghana (Source: Oteng-Ababio 31 ).
Despite the varied age groups within the Agbogbloshie scrap yard, the workforce is mostly young between 15 and 35 years, and children as young as 8 years are involved in the e-waste activities. The target population was those working on e-waste and also food sellers and hawkers at the Agbogbloshie scrap yard. It was estimated that there were about 500 e-waste workers based on interaction with the e-waste workers. Observations made during fieldwork in this study showed that there were no school facilities at the Agbogbloshie scrap yard and its immediate environs. Some workers live in the worksite environment with their families in wooden structures. Others live 100 m across the Odaw River in the informal settlement called Sodom and Gomorrah. 32 It is ironic that this contaminated occupational and residential setting is known as Sodom and Gomorrah.
Data collection and sampling procedure
Based on a population of 500, confidence level of 95%, margin of error of 5%, and response distribution of 50%, a minimum sample size of 218 was considered to be adequate for the study. The random sample was drawn from the adult population composed of e-waste and non e-waste workers who were 18 years or older and either resident or nonresident in the Agbogbloshie community at the time of the survey (January and March 2017). A total of 260 participants were involved in the survey. Of the lot, 140 were resident e-waste workers, 60 were resident non e-waste workers, and another 60 were nonresident non e-waste workers.
A community in Winneba in the central region of Ghana was selected as the control location for two reasons. First, there is no e-waste burning in the community. Second, the community members in the control location are closely related to residents of Agbogbloshie in terms of culture, ethnicity, dominant religion, and age distribution. This suggests that combustion of e-waste was the main distinguishing feature between the two communities. This is necessary to limit the influence of confounding factors in the study. Tests of content validity, internal consistency, and reliability of the instrument were ascertained before commencement of the study. There were two types of questionnaire—one for e-waste workers and one for all other groups (i.e., resident non e-waste workers and nonresident non e-waste workers).
Measures
Outcome variables
Four response variables namely eye problems, skins burns, breathing difficulty, and coughing were considered in this study. In the context of this study, eye problems include watery eyes, eye irritation, and eye infection. For each disease symptom, respondents were asked whether they had experienced it in the past 1 month or not. The dichotomous response was coded as 0 (for no) or coded as 1 (for yes).
Predictors
Variable selection or model specification methods for this study were based on theoretical relevance and sequential regression analysis. In addition, the selection and sequence of entry of the predictor variables in the regression models were informed by parsimony, model fit, theoretical relevance, and previous experience. The main predictor was residential occupational status, a composite variable of residential status (resident, nonresident) and worker status (e-waste worker, non e-waste worker). Ordinarily, this automatically yields four mutually exclusive groups—resident e-waste workers, resident non e-waste workers, nonresident e-waste workers, and nonresident non e-waste workers. However, one of the four cells (nonresident e-waste workers) was empty. Therefore, three mutually exclusive groups were obtained (resident e-waste workers, resident non e-waste workers, nonresident non e-waste workers) and used throughout the univariate, bivariate, and multivariate analyses. It is well documented that disease varies systematically with compositional factors (biosocial and sociocultural factors). For this reason, compositional factors were accounted by including them in the regression models. These include gender, age, religion, and educational attainment.31, 33 , 34 , 35 Typically, the literature reports three key biosocial factors—age, gender/sex, and ethnicity/race that systematically vary with exposure to environmental hazards. Besides age and sex, ethnicity was measured in this study, but it was dropped because there was little variability in its distribution and it had limited explanatory power when it was originally included in the regression models. Educational attainment was included because it was assumed that highly educated people would be taking more precautions to reduce their risk of exposure to the hazard.
Furthermore, anecdotal evidence suggests that most of the highly educated e-waste workers are not directly involved in the burning of e-waste, but are either supervisors or employers of the less educated individuals engaged in e-waste activities. This made it interesting to assess whether self-reported adverse health outcomes systematically varied with educational attainment of e-waste workers. Years of experience and income of e-waste workers were also measured and originally included in the regression models. However, both variables were dropped either because of multicollinearity (i.e., experience and age) or limited explanatory power (i.e., income).
Data and statistical analyses
Data were analyzed using the IBM SPSS version 20 and Stata version 13 software. Data analyses included univariate, bivariate, and multivariate statistics. The relationships between disease symptoms (eye problems, skins burns, breathing difficulty, coughing) and residential–occupational status of e-waste workers were determined using generalized linear models (GLMs). The GLM simplifies regression by allowing the linear model to be related to the response variable through a link function and by allowing the magnitude of the variance of each measurement to be a function of its predicted value.
For analytical purposes, the joint effect of worker status (e-waste or non e-waste worker) and residential location (resident or nonresident) on the likelihood of reporting each of the four disease symptoms was estimated using exponentiated coefficients—odds ratios (ORs). The OR = 1 implies that higher values of the predictor do not affect the odds of reporting a specific disease symptom; OR >1 implies that higher values of the predictor are associated with higher odds of reporting the disease symptom, and OR <1 implies that higher values of the predictor are associated with lower odds of reporting the disease symptom. Under the assumption of a binary response (no = 0, yes = 1) to each of the disease symptoms, there are a number of probable options: the logit model, probit model, complementary log-log model, and negative log-log model depending on the link function of the GLM. Both logit and probit link functions have the same property, which is link
In this study, only one outcome variable satisfied this property of symmetry—that is those who reported eye problems (52% yes, 48% no). When the number of affirmative and negative responses is asymmetric in the [0, 1] interval, as in the case of three outcome variables in this study, a complementary log-log link function or negative log-log link is appropriate depending on the distribution. 37 , 38 Sixty-two percent of respondents reported coughing while the rest did not. The complementary log-log model, which takes into account the fact that affirmative responses are more probable, gives a better representation and was therefore used for the analysis of the relationship between the odds of reporting coughing and theoretically relevant variables. Skin burns (38% yes, 62% no) and breathing difficulty (42%, 58% no) both signify asymmetry in the distribution of reported disease symptoms, with no as more probable responses. Therefore, parameter estimates for both disease symptoms were established by binary negative log-log regression (a GLM), which was adjusted for the remaining independent variables included in the regression models.
The regression models in this study were built under the assumption of independence of subjects, but the cross-sectional survey has a hierarchical structure with respondents nested within survey clusters, which could potentially bias the standard errors (SE). STATA 13 (StataCorp, College Station, TX) SE, which has the capacity to address this problem, was used by imposing on the models a “cluster” variable, that is, the identification numbers of respondents at the cluster level. This, in turn, adjusted the SE producing statistically robust parameter estimates.
Ethical statement
The study design was approved by the University of Cape Coast Institutional Review Board (IRB). A priori permission was sought from identifiable leaders in the communities, and the purpose and details of the study were explained to them. Both oral and written consent were obtained from each participant before the study. Participants were neither coerced nor financially induced to take part in this study. They were informed that the information provided will contribute to the overall knowledge about the effects of e-waste on their health.
Results
The results of the distribution of resident e-waste workers, resident non e-waste workers, nonresident non e-waste workers by sociodemographic attributes (gender, age, marital status, education, household size and religion), as well as the distribution of reported health symptoms based on joint occupational and residential status, are presented in this section. Contextual differences in significant predictors of reported health symptoms and the outputs of the multivariate logit, complementary log-log, and negative log-log regression models are also presented in this section.
Demographic profile of e-waste and non e-waste workers
Cramér's V was used to determine the magnitude of effect sizes of the relationships between categorical variables. There were statistically significant differences in occupational type and residential status between the proportions of e-waste workers and their non e-waste counterparts by gender (
Demographic Profile of Respondents (n = 260)
Rows sum up to 100%.
Based on χ 2 statistics, and in terms of proportions, there were associations between the occupation and place of residence of respondents and the frequency of reporting eye problems, skin burns, breathing difficulty, and coughing (Table 2). However, based on the magnitude of Cramér's V, none of the associations was strong. It is obvious from Table 2 that non e-waste workers who were also not resident in the contaminated work environment reported the least number of eye problems, skin burns, breathing difficulty, and coughing. Resident e-waste workers reported the highest frequency of skin burns and breathing difficulty, whereas resident non e-waste workers reported the highest frequency of eye problems and coughing. The foregoing suggests that there is some cumulative health disadvantage to individuals who only reside in the e-waste contaminated environment although they do not necessarily work there.
Distribution of Health Symptoms Based on Occupational–Residential Status (n = 260)
Rows sum up to 100%.
Multivariate Statistical Analyses
The likelihood of e-waste workers to report four adverse health outcomes (eye problems, skin burns, breathing difficulty, and coughing) was considered in GLMs at the multivariate level. The place of residence and work of respondents were jointly considered as the key independent variable to predict the likelihood of reporting each of the four outcome variables by the e-waste and non e-waste workers.
Likelihood of e-waste workers and their counterparts to report eye problems
Resident e-waste workers were 102% more likely to report that they had experienced eye problems compared with their counterparts who were resident non e-waste workers (Table 3). However, individuals who were neither e-waste workers nor resident in the contaminated work environment were 64% less likely to report eye problems compared with their counterparts who were resident non e-waste workers.
Multivariate Logit Regression Model Predicting the Experience of Eye Problems by E-Waste Workers
Bold font indicates significant ORs.
OR, odds ratio; SE, standard errors.
When biosocial factors were taken into account (Table 3), the relationship between resident e-waste workers and experience of eye problems was not robust and disappeared indicating that age and gender mediate this relationship. However, gender was not a significant predictor of eye problems in either the biosocial or sociocultural model. Individuals who were neither e-waste workers nor resident in the contaminated work environment were 74% less likely to report eye problems in the biosocial model compared with their counterparts who were resident non e-waste workers. Individuals in the 21–30 age group were far more likely (OR = 6.26, p < 0.01) to report eye problems compared with those in the less than 20 years group. Similarly, individuals in the 31–40 age groups were far more likely (OR = 8.74, p < 0.001) to report having experienced eye problems compared with individuals within the age group below 20 years. The magnitudes of the OR for reporting eye problems within the 41–50 and 51–60 year groups are analogous to the preceding trends although to varying levels of statistical significance. These trends persisted even when sociocultural attributes of the e-waste workers such as educational attainment and religion were accounted for (Table 3). The relationship between the joint effect of compositional and environmental attributes and likelihood of reporting eye problems disappeared completely when biosocial and sociocultural factors were taken into account. None of the categories of educational attainment was a significant predictor of self-reported eye problems except tertiary education (Table 3). Individuals who had attained tertiary education were far less likely to report eye problems compared with their counterpart without any formal education.
Likelihood of e-waste workers and their counterparts to report skin burns
Resident e-waste workers were 84% more likely to report experience of skin burns compared with their counterparts who were resident non e-waste workers (Table 4). In contrast, individuals who were neither e-waste workers nor resident in the contaminated work environment were 54% less likely to report skin burns compared with their counterparts who were resident non e-waste workers.
Multivariate Negative Log-Log Regression Model Predicting the Experience of Skin Burns By E-Waste Workers
Bold font indicates significant ORs.
The direction and magnitude of the odds of reporting skin burns persisted when age and gender of the respondents were controlled in the biosocial model. Resident e-waste workers were more likely (OR = 1.69, p < 0.05) to report having experienced skin burns compared to those who were resident non e-waste workers. However, individuals who were neither e-waste workers nor resident in the contaminated work environment were less likely to report skin burns (OR = 0.36, p < 0.0001) compared with their counterparts who were resident non e-waste workers. Gender was not a significant predictor of skin burns in both the biosocial and sociocultural models (Table 4). Except the 51–60 age groups, all categories of age were significant predictors of self-reported skin burns. Individuals in the 21–30 age group were more likely (OR = 2.09, p < 0.01) likewise those in the 31–40 age group were more likely (OR = 3.81, p < 0.0001) to report that they had experienced skin burns compared with individuals below 20 years old. In addition, individuals in the 41–50 age groups were 123% more likely to report that they had experienced skin burns compared with their counterparts under 20 years old (Table 4).
The higher odds of resident e-waste workers to report skin burns disappeared completely in the sociocultural model suggesting that in addition to biosocial factors, sociocultural attributes mediate the relationship between residential–occupational status and the likelihood of reporting skin burns (Table 4). The relationship between the 41 and 50 age groups and reporting of skin burns disappeared in the sociocultural model unlike the 21–30 age groups and 31–40 age groups which persisted. Individuals who had attained tertiary education were 98% less likely to report skin burns compared with their counterpart without any formal education.
Likelihood of e-waste workers and their counterparts to report breathing difficulty
Resident e-waste workers had higher odds of reporting breathing difficulty (OR = 3.30, p < 0.0001) compared with their counterparts who were resident non e-waste workers (Table 5). This is in sharp contrast with individuals who were neither e-waste workers nor resident in the contaminated work environment who were far less likely to report breathing difficulty (OR = 0.24, p < 0.01) compared with their counterparts who were resident non e-waste workers.
Multivariate Negative Log-Log Regression Model Predicting the Experience of Breathing Difficulty by E-Waste Workers
Bold font indicates significant ORs.
When biosocial factors were taken into account (Table 5), the relationship between resident e-waste workers and experience of breathing difficulty was robust and persisted. However, gender was not a significant predictor of breathing difficulty in either the biosocial or sociocultural model. Individuals who were neither e-waste workers nor resident in the contaminated work environment were less likely to report breathing difficulty in the biosocial model (OR = 0.12, p < 0.01) compared with their counterparts who were resident non e-waste workers. There was no relationship between nonresident non e-waste workers and breathing difficulty in the sociocultural model. Except the 31–40 age groups, in the biosocial model, none of the age categories was a significant predictor of self-reported breathing difficulty. In the sociocultural model, resident e-waste workers were more likely to report breathing difficulty (OR = 2.92, p < 0.05) compared with their counterparts who were resident non e-waste workers. Apart from the 21 to 30 age groups, none of the age categories was a significant predictor of self-reported breathing difficulty in the sociocultural model. Interestingly, none of the educational attainment categories was a significant predictor of the likelihood of reporting breathing difficulty unlike what was observed in the self-reported eye problems and skin burn regression models.
Likelihood of e-waste workers and their counterparts to report coughing
Interestingly, there was no relationship between where e-waste and non e-waste workers live and work and their likelihood of reporting of coughing (Table 6).
Multivariate Complementary Log-Log Regression Model Predicting the Experience of Coughing by E-Waste Workers
Bold font indicates significant ORs.
Unlike gender, age groups were a significant predictor of self-reported coughing in both the biosocial and sociocultural models. Individuals in the 21–30 age group (OR = 3.46, p < 0.01) likewise those in the 31–40 age group (OR = 3.51, p < 0.0001) were, respectively, more likely to report that they had experienced coughing compared with individuals below 20 years old. In addition, individuals in the 41–50 age groups were far more likely to report that they had experienced coughing compared with their counterparts under 20 years old.
Discussion
This study set out to assess the magnitude of the relationship between where individuals live and work and self-reported experiences of disease symptoms. On the whole, it is evident that for each of the four adverse health outcomes (eye problems, skin burns, breathing difficulty, coughing), the order of magnitude of the effect in decreasing order is as follows: resident e-waste workers > resident non e-waste workers > nonresident non e-waste workers. There is some health disadvantage to individuals who only reside in the e-waste contaminated environment although they do not necessarily work there. It is well documented that occupation influences health outcomes 39 , 40 , 41 , 42 ; likewise place of residence and neighborhood. 43 , 44 , 45 However, only few studies have considered the joint effect of occupation and residential neighborhood on adverse health outcomes especially in developing country contexts.
More often than not, the consequence of work-related health risks on the health and safety of people is analyzed separately according to the effect of (1) physical agents (e.g., noise, vibration, radiation, and temperature), (2) chemical agents (e.g., asbestos, lead, and pesticides), (3) ergonomic conditions (e.g., inconvenient work postures and lifting of heavy materials), (4) working time arrangements (long and irregular workdays, shifts, and night work), and (5) workplace violence (harassment and discrimination).27,29,30
This approach has failed to elicit a nuanced understanding of the cumulative effect of physical, chemical, and ergonomic conditions and other factors on the health and safety of workers. This makes it imperative to need to carefully consider the determinants of multifactorial risks, such as the combined exposure to elements of the work environment and neighborhood risk factors. 46 , 47 The distinction between “where people work,” that is, economic sector, and “what they do,” that is, occupation, is important in exposure characterization. For example, within the e-waste recycling subsector there are people, who work as dismantlers, but also people who work as metrologists (measure the weight of scrap metals), hawkers, or food vendors. Given that the role of environmental factors in shaping human health is fundamental, place-based and neighborhood issues are of essential significance to addressing health questions. A plethora of place-based factors influence health. These include physical circumstances (e.g., altitude, temperature regimes, and air pollutants), social context (e.g., social networks and perception of risk behaviors), and economic conditions (e.g., poverty, urbanicity, and quality of nutrition).47, 48 , 49 Since place-based/neighborhood influences are myriad and dynamic, and because people are mobile, understanding the health impacts of where people live is one of the most challenging, yet important, contemporary environmental health problems. 45
There were no systematic differences between males and females regarding the likelihood of reporting of eye problems, skin burns, breathing difficulty, or coughing. Most of the e-waste workers were male, whereas the food vendors and sellers in the work environment were female indicating that the e-waste sector in Ghana is male dominated and by extension, gender differentiated. Gender segregation in employment has two aspects: horizontal segregation, meaning that women and men do not work in the same sectors, and vertical segregation whereby, within the same sector, women and men do not hold the same type of positions. 50 With regard to new and emerging risks, the increased participation of women in the workforce has increased their exposure to hazardous substances, especially carcinogenic, mutagenic, and reprotoxic substances (e.g., from working with electronic components). 50
According to EU OSHA 50 , the main endogenous factors which put female workers at higher risks of developing work-related health problems or of suffering from occupational accidents are associated to women's biological differences with men, particularly with regard to their reproductive and sexual functions and to their physical strength. Pregnancies and breastfeeding, menstruation, menopause, fertility, and sexual and reproductive functioning are relevant factors in the occupational safety and health of female workers. Poor working conditions can contribute to a range of health issues for women associated with pregnancy and the period after giving birth, including tiredness and fatigue, pain and discomfort, back problems, postural problems, swollen legs, nausea, blood pressure changes, and stress. 51
Older resident e-waste workers reported more eye problems, skin burns, breathing difficulty, or coughing than their younger counterparts (those below 20 years). Older workers are more likely to have worked in this contaminated work environment for much longer than their younger counterparts. Therefore, they are more likely to have been exposed to the smoke and soot that characteristically defines e-waste work environment, and the natural process of aging could increase vulnerability to eye problems. One noteworthy issue was that both young and old e-waste workers did not use any personal protective equipment in this occupational setting. Young workers are unique because they lack experience and maturity regarding their particular occupation, including the safety and health risks associated with it. 52
Young workers typically consider that they are physically healthier and stronger than older workers, which explains why they are less reluctant to work in high-risk sectors and are more risk-taking in their occupation. 52 However, carrying out physically demanding tasks often requires training, experience, and knowledge of the tools (such as dismantling technology) and can be easier for an older worker with 10 years experience than for a 20 year old. 53 Young workers are more likely to be exposed to high risk agents than older workers, as the latter tend to adopt a more cautious attitude toward their health and safety. However, the cumulative duration of exposure over time implies that older e-waste workers begin to manifest symptoms such as eye problems, skin burns, breathing difficulty, or coughing as observed in this study. Recognizing and understanding the relationships between health hazards in occupational settings and development of disease in workers are challenging for many methodological and practical reasons.
Many occupational diseases and disorders are chronic, meaning that they take several years of exposure to manifest. Most are multifactorial in origin, so that nonoccupational risk factors may also play an important role in causing or exacerbating them. Exposures may not be completely identified, and they may change well before the disease becomes apparent. The numbers of workers exposed may be insufficient for any relationship to be “established” statistically or even suspected. Moreover, evidence supporting the role of work and personal risk factors in the health of working people is frequently underused in developing interventions. 12
Individuals who had attained tertiary education were far less likely to report eye problems and skin burns although they did not systematically differ from less educated groups regarding the experience of breathing difficulty and coughing. Most of the highly educated e-waste workers were not directly involved in the burning of e-waste but were either the supervisors or employers of the less educated cohort. It is therefore unsurprising that they reported fewer health problems. However, there are other important moderating factors. Education changes the way individuals behave and the choices they make but so do ethnicity and gender. Specific historical or social contexts will also moderate the behaviors and the effects of education on health. These moderating effects may apply to all of the elements of the regression models so that a single model is inadequate to the task of describing the effects of education for all individuals in all social, historical, and cultural circumstances.
Education impacts on health because individuals exist in multiple multilayered and interacting context; each of these contexts is a domain of social relations and environmental health; and education impacts on each factor in each context at each level.47, 54 We must distinguish between education as a context and education as a process because the two elements of education have different types of implication for health. Some of the benefits and/or risks of education for health result from the membership or participation in a learning institution, others from the explicit experience of the process of learning. For instance, attainment of tertiary education may not necessarily mean that an individual is knowledgeable in the practical dimensions of e-waste value chain. An individual who has primary education but longer years of experience as an e-waste worker may be very knowledgeable because of the longstanding engagement in the e-waste sector. In this context, it is also pertinent to emphasize that there are important experiences of learning that do not take place within educational settings, key examples of which are learning in the workplace and peer learning as in peer–peer interaction.
The enactment of legislation and inspection of workplaces has been the conventional mechanism of facilitating health and safety in occupational settings and ensuring compliance with health and safety standards. This mechanism has hitherto been effective in addressing a variety of occupational hazards in developed countries unlike in developing countries due to a number of reasons. When it comes to the burden of e-waste, several developing countries in Asia and Africa that lack proper systems for recycling and disposal are experiencing increasing problems; first because consumption of electronics is increasing most within these countries at present, and second because e-waste is exported from the rich world to developing nations that lack the capacity and regulations to handle this waste in a responsible manner. Third, the informality of the e-waste sector implies that in most cases production takes place in workers homes or precarious work environments prone to serious health hazards such as harmful dust, chemicals, noise, and heat. It is formidable to inspect such workplaces owing to the large numbers and wide distribution. Moreover, the e-waste sector in developing countries is an industry within which inspection-based systems are either nonexistent or insufficient. This makes it imperative to develop other systems to safeguard the health of e-waste workers. Furthermore, health problems linked to occupation have steadily risen in type and magnitude and have culminated or exacerbated diseases owing to exposure to several risk factors, only one of which is the work environment. For example, chronic obstructive pulmonary disease is fundamentally caused by smoking; however, it may be aggravated by dusts and gases in the workplace.
Study limitations
As in any empirical investigation, this study has limitations in relation to study design and analysis. The cross-sectional nature of the study design precludes statements of causality. Another limitation is related to data collection and the unit of analysis. The data for this study were collected at an individual level, and the empirical tests of the hypotheses were conducted on self-reported survey data. The use of individual-level data can be problematic because it characteristically examines exposures and responses of individuals, which limits their power, and suggests that much could be learned from contextual comparisons. Group-level or contextual data, which examine exposures and responses of aggregates or clusters of individuals, such as locales, may be needed to complement the individual-level data in this study. Despite the precise measurement of constructs in this study, the subjective assessment (i.e., the use of e-waste worker reports of disease symptoms) represents only an estimate of adverse health outcomes, which might be subject to recall bias. Thus, inclusion of multisource data such as objective assessments (i.e., actual medical records) could lessen this risk and add to the findings of this study. Owing to these limitations, a priori steps were taken to reduce these biases in the design of the study by selecting the most valid and reliable measures, protecting respondent anonymity and reducing evaluation apprehension, and improving items in the instrument to eliminate ambiguity.
Conclusion
E-waste, or electronic waste, describes end-of-life electrical goods such as computers, televisions, printers, and mobile phones. Each year between 20 and 50 million tons of e-waste is generated worldwide. Due to the crude recycling process, many pollutants, such as persistent organic pollutants and heavy metals, are released from e-waste, which can easily accumulate in the human body through the inhalation of contaminated air. E-waste connected health risks may result from direct contact with harmful materials such as lead, cadmium, chromium, brominated flame retardants, or polychlorinated biphenyls, from inhalation of toxic fumes, as well as from accumulation of chemicals in soil, water, and food. In addition to its hazardous components, being processed, e-waste can give rise to a number of toxic by-products likely to affect human health. Furthermore, recycling activities such as dismantling of electrical equipment may potentially bear an increased risk of injury. In this study, we assessed adverse health outcomes (eye problems, skin burns, breathing difficulty, and coughing) reported by e-waste workers who live and work in the contaminated occupational environment, e-waste workers who do not reside there but work there, and individuals who neither work nor live there. In all cases, e-waste workers who reside and work in the contaminated work environment reported higher frequencies of eye problems, skin burns, breathing difficulty, and coughing. This relationship was robust and persisted even when biosocial (age and gender) and sociocultural attributes (marital status, years of experience, religion, household size, and education) were taken into account.
The relationships between the set of predictors and each of the adverse health outcomes were complex indicating the need to take into consideration how physical, chemical, and ergonomic conditions and other factors influence the health and safety of e-waste workers. The ultimate goal of this consideration and by extension any clean air policy is to develop strategies to reduce the risk of adverse effects on human health and the environment as a whole caused by ambient air pollution. Almost all the e-waste workers had no personal protective equipment and were totally exposed to the chemical contaminants, as well as smoke and heat. In this context, risk reduction strategies are and will continue to be powerful tools in promoting good health for e-waste workers. The development of such strategies requires not only qualitative but also quantitative knowledge on the most relevant adverse effects.
Footnotes
Author Disclosure Statement
No competing financial interests exist.