
Abstract
The COVID-19 pandemic has underscored how underlying disparities in environmental and health conditions exacerbate vulnerability during public health emergencies in low-income and communities of color. Neglected epidemics—high rates of pollution, chronic disease, and racial and socioeconomic health disparities—have continued amid persistent systemic racism and declining investment in public health. Recognized too late due to shortcomings in public health data tracking, COVID-19 has surged through vulnerable communities. Improved public health tracking is critical for informing the country's recovery from COVID-19, and it can be leveraged to measure and reduce health disparities and strengthen community resilience to respond more effectively to the next public health crisis. We emphasize how public health tracking agencies can engage communities in data collection and reporting; we also discuss the complementary role that communities can take to mobilize data to change policies and institutions, strengthening resilience through increased information and capacity driven by community priorities. Success requires the continuous collection of timely data at a community scale, and public health agencies partnering with communities to use the information in decision making and evaluation to ensure progress over time. We highlight community-engaged data collection and reporting—community air monitoring in Imperial County, CA—as an example of working with communities to improve public health data collection and reporting, increase community dialogue and engagement in governmental decision making, and inform public health tracking to reduce health disparities and strengthen community resilience.
INTRODUCTION
Stark racial and ethnic disparities exist in the incidence and severity of COVID-19 illness (the illness caused by the severe acute respiratory syndrome coronavirus 2 virus or SARS-CoV-2). Nationally, the COVID Tracking Project reports that 23% of COVID-19 deaths are among African Americans (cases with race data, as of July 27, 2020), although they comprise 13% of the U.S. population. 1 In New Mexico, American Indians/Alaska Natives account for 59% of COVID-19 deaths, but just 9% of the total population; in California, Native Hawaiian/Pacific Islanders have a rate of COVID-19 infections of 218/100,000 compared with an overall rate of 62/100,000 statewide, 2 and Latinos are contracting COVID-19 infections at three times the rate of whites. 3
However, the data needed to fully and rapidly assess and address the racial, ethnic, and socioeconomic disparities in COVID-19 impacts have not been released in a timely manner, are not standardized across communities and states, nor reported publicly and independent of political influence. During the early stages of the pandemic, few states reported data by race and ethnicity for cases, deaths, and testing, 4 , 5 limiting epidemiological investigations and a targeted policy response. In California, as in a number of other states, race and ethnicity data are missing for over one out of three reported cases. 6 The federal government only recently required that states submit demographic data on COVID-19 cases and deaths by August 1, 2020 7 —7 months after the first reported cases in the United States. Concerns have been raised about the politicization of surveillance data by selective suppression of data: for example, Nebraska chose to stop reporting data on infections at meatpacking facilities, an industry where nearly 75% of employees are black or Latino, and that accounts for nearly one out of six cases in Nebraska. 8 , 9 Public health professionals have raised concerns about data suppression and transparency after directives for hospitals to report data to the Department of Health and Human Services rather than long-standing procedures to report data to the Centers for Disease Control and Prevention (CDC). 10
The COVID-19 pandemic has shown how an underfunded and fragmented data infrastructure can hinder our collective ability to protect the public's health. Public health systems did not adequately detect community spread early in the pandemic; have not provided standardized and comparable data across states and municipalities; and have largely lacked contextual data on the association between COVID-19 and race, socioeconomic status, and pre-existing health conditions. This gap in actionable surveillance data has undermined decision making on how to effectively reduce the spread of COVID-19 through rapid testing, case identification, contact tracing, and case isolation, as well as efforts to equitably target public health messaging and resources to the most vulnerable communities. 11
Low-income and communities of color entered the COVID-19 pandemic with multiple vulnerabilities, including higher rates of chronic disease, 12 exposure to pollution, 13 , 14 and disparities in health care access and treatment. 15 Many residents in these communities are also more likely to be essential workers, to live in crowded housing, and to be uninsured. 16 People in these communities are also more likely to bear a disproportionate risk of exposure to multiple socioeconomic stressors and environmental hazards over time, otherwise known as cumulative impacts that contribute to excess burden of disease, 17 further underscoring the salience of systemic racism as a risk factor for COVID-19. 18 For example, in California, Census tracts with higher proportions of African American and Latino residents tend to have higher levels of particulate matter pollution from vehicles 19 ; likewise, black and Latino Californians are more likely to live in zip codes where multiple environmental health hazards are concentrated. 20
Recent research suggests that previous exposure to air pollution may exacerbate COVID-19 severity—possibly by directly limiting the body's ability to fight off the virus, or by causing underlying chronic diseases that are associated with higher COVID-19 fatality. 21 , 22 , 23 , 24 In a preliminary cross-sectional study of 3000 U.S. counties (98% of the population), an increase of 1 microgram per cubic meter (μg/m 3 ) in long-term exposure to fine particulate matter (PM2.5) increased COVID-19 death risk by 8%. 25 Another analysis found that each 1 μg increase in PM2.5 was associated with an average of 9.4 more cases, 3.0 more hospitalizations, and 2.3 more deaths from COVID-19. 26 Previous research has linked poor air quality to premature death, acute respiratory illness, and emergency room visits and hospitalizations from asthma. 27 , 28 , 29
Particulate matter exposure is specifically linked with inflammation in the lungs, 30 adverse effects on the immune system, 31 cardiovascular mortality, and abnormal blood clotting 32 ; all of these factors are predictors of death from severe COVID-19 disease. 33
The discovery of the potential link between COVID-19 severity and air pollution was possible because of data collected from both environmental and public health tracking. Tracking refers to the ongoing systematic collection, analysis, interpretation, and reporting of data to inform and empower public health decisions. Tracking is foundational to the three core functions of public health: (1) assessment, (2) policy development, and (3) assurance. 34 Without data for public health assessment, it is not possible to understand the distribution, drivers, and changes in community health and enable evidence-based policy development. Without sufficient data to evaluate success, there can be no assurance that decisions are effective, unbiased, and adequate to protect health. Data collection, analysis, and interpretation must occur continuously, regardless of location or time, feeding a cycle of assessment, action, and evaluation.
CONCEPTUAL FRAMEWORK
The COVID-19 pandemic is a generational public health disaster, rapidly unfolding on a global scale, with other crises sure to follow. Climate change is also a global public health disaster that will impact every future generation in the United States and globally. Regional disasters such as Hurricane Katrina, and local disasters such as wildfires, will continue to occur with increasing frequency. But our current public health response, lurching from one crisis to the next, poorly serves the public interest. The Institute of Medicine warned in 1998 that giving attention to “specific foci of interest lead(s) to episodic action, but not the sustained effort that is needed” to support public health capacity. 35
Accurate, local, and timely data are essential during public health crises, but a sustained investment in public health data and information is critical for increasing emergency preparedness and community resilience needed to withstand future crises. Community resilience—the ability to withstand, adapt, and recover from a disaster or other catastrophic event—depends on rapid and relevant information gathering and sharing through social and institutional networks. 36 Figure 1 outlines six dimensions of community resilience for which data need to be tracked—as well as five characteristics of data that are actionable at a community scale—to strengthen resilience and more effectively respond to and recover from public health emergencies. 37
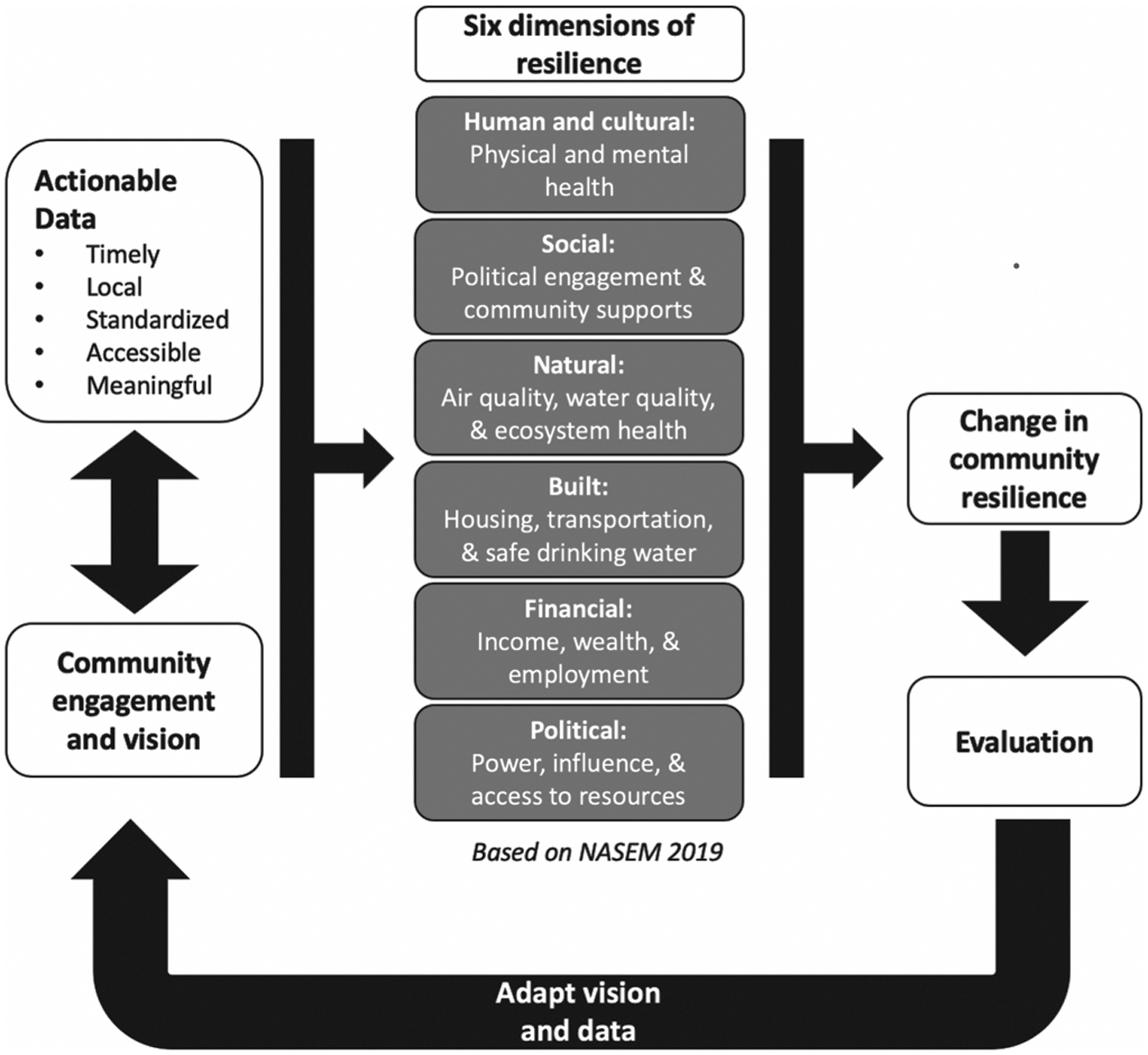
Actionable data can be used to envision, change, and evaluate community resilience.
Information relevant to many of the six dimensions of resilience are tracked over time and space by various governmental and nongovernmental entities. For example, data are available throughout much of the world on air quality, water quality, and financial indicators. However, the data often do not serve the priorities of the community: for example, air quality may not be measured at a sufficiently detailed local or neighborhood-level scale, and many important and emerging drinking water contaminants are not monitored. For this reason, data collection efforts need to be constantly evaluated with respect to community priorities and improved to be actionable for communities; in some cases, when relevant hyperlocal data are not available, a citizen/community science approach to collecting data may be called for. 38 Other dimensions of resilience, such as social cohesion, are difficult to measure and track, but no less important: social and cultural resilience are key to protecting health in communities, but are difficult to measure in a standardized way and, therefore, neglected by researchers and policymakers. Complex interactions among these dimensions are also difficult to measure but can be critically important. For example, the need to socially isolate in response to the COVID-19 pandemic will reduce community resilience in the event of a heat wave or wildfire because it may be unsafe to go to cooling centers or evacuation shelters, thereby potentially increasing risk of illness or death from heat-related illness or fire.
As shown in Figure 2, leveraging data to strengthen community resilience requires a repeated set of actions by public health agencies or other organizations, and a complementary set of actions taken by communities. From a foundation of data collected in response to community priorities, public health actions to strengthen resilience can include (1) providing information in response to a concern; (2) providing education, training, and/or outreach; (3) improving data quality and access; (4) informing or improving public health response plans, interventions, or programs; (5) informing policy, regulation, or legislation; and (6) implementing interventions to reduce or prevent exposure to health hazards. 39
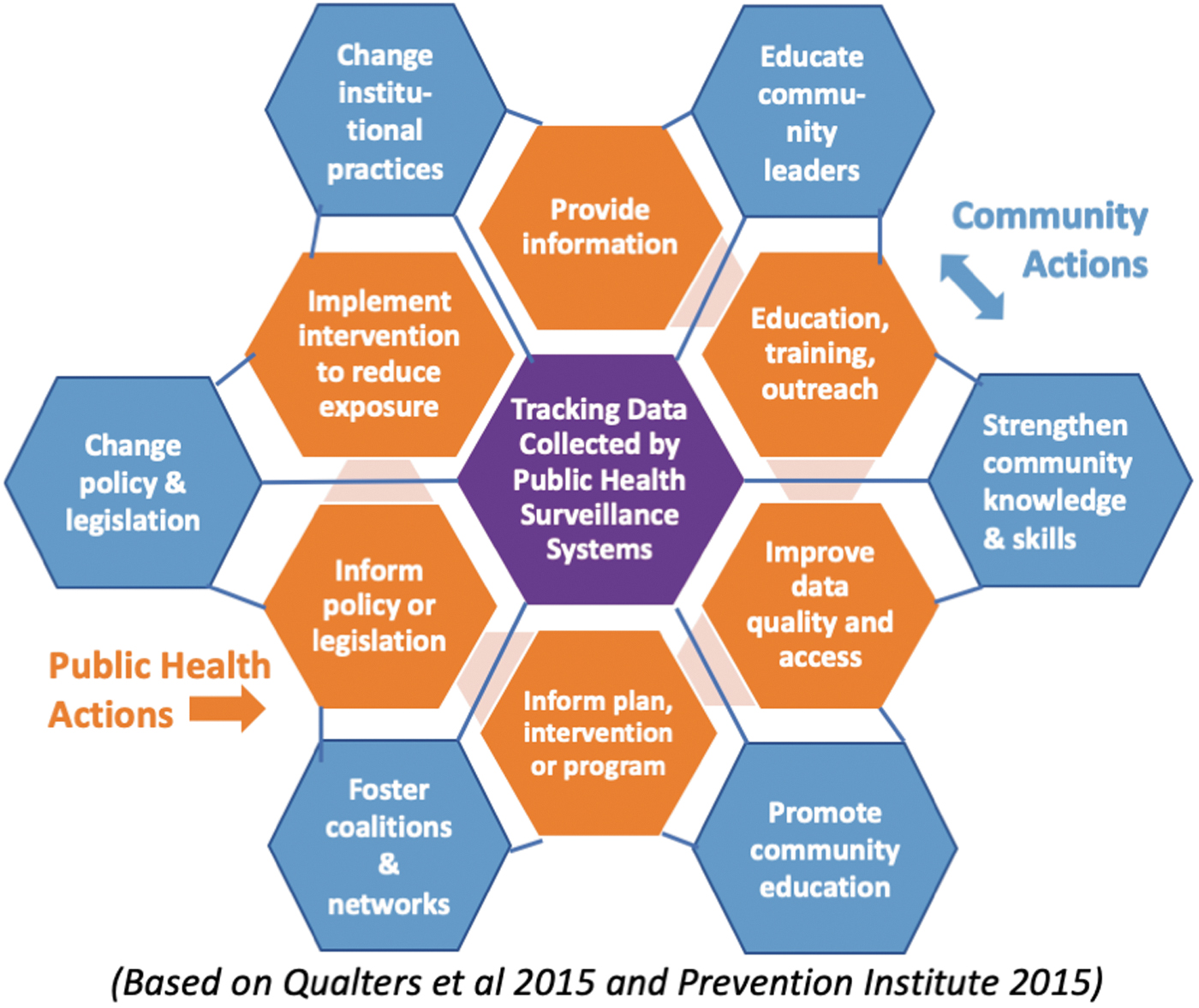
Framework for using tracking data to strengthen community resilience and address environmental health disparities.
The Prevention Institute's THRIVE framework provides a spectrum of community actions that can improve upstream determinants of health and address health disparities. 40 These include (1) strengthening individual knowledge and skills, (2) promoting community education, (3) educating providers, (4) fostering coalitions and networks, (5) changing organizational practices, and (6) influencing policy and legislation. 41 The THRIVE framework outlines a strengths-based approach to community resilience centered on leveraging local relationships, knowledge, and other assets or capacities in implementing actions to improve community conditions and social determinants that shape health outcomes. These determinants of health include access to safe, quality, and affordable housing, green space, transportation, education, employment, goods and services, and environmental resources such as water, soil, and indoor and outdoor air.
Assets or capacities that contribute to resilience, which the spectrum of community actions in the THRIVE framework can both leverage and strengthen also include trusting relationships among community members and institutions; meaningful participation by local leadership and involvement in community-based institutions; opportunities for artistic and cultural expression that reflects the identities and backgrounds of all residents; accessible literacy development for all ages that effectively serves all learners; and broadly accepted behaviors, shared knowledge, and sets of practices that can promote community wellness. 42 For example, community-led actions taken to educate residents or service providers can both tap into and fortify existing relationships among residents and institutions to deliver information or services. These actions can also strengthen community resilience by building trust between residents and public health institutions 43 or engaging community health workers as credible messengers to better reach vulnerable populations. 44
Actions from public health institutions that are informed by tracking data can in turn support community-led actions to improve health and strengthen resilience, and vice versa. For example, when a public health agency provides data and information, education, or training in response to a concern identified by community stakeholders, the agency should be supporting actions to grow community knowledge and skills or to promote community health education and literacy. Likewise, community action to change institutional practices around what data are collected, how they are reported, and subsequent policy changes can help build a public health system more responsive to community priorities and increase adherence to public health guidelines.
CASE STUDY: AIR QUALITY TRACKING FOR COMMUNITY ACTION IN IMPERIAL COUNTY
Imperial County, California, consistently ranks among the counties with the worst air quality in the state. 45 , 46 The largely Latino community (84.6%) 47 also contends with some of the highest poverty 48 and unemployment 49 rates in the state, and among the highest rates of emergency room visits 50 and hospitalizations for childhood asthma in California. 51 Imperial County as of June 2020 also had the highest hospitalization rates for COVID-19 in California, 52 compounded by large populations of vulnerable essential workers such as migrant farmworkers living in congregated housing and U.S. citizens returning from Mexico for treatment in Imperial County. 53 As noted earlier, recent studies suggest that air pollution may play an important role in fatalities from COVID-19, exacerbating community vulnerability during the pandemic. 54 Chronic conditions associated with exposure to air pollution—including diabetes, heart disease, and respiratory disease—have also been associated with risk of death from COVID-19, and these conditions are most prevalent among low-income and communities of color. 55
In 2014, Imperial County residents took action to address decades of disparities in the area's air quality when compared with the rest of California. As a first step, the community resolved to address two critical data gaps that potentially contributed to systematic underestimates of local pollution. First, governmental regulatory monitors designed to track ambient air pollution levels did not collect air quality data on a neighborhood scale; second, the data did not appear to accurately reflect the pollution peaks that local residents often experienced.
Comite Civico del Valle (CCV), a local community organization, partnered with researchers from Tracking California and the University of Washington to develop the Imperial County Community Air Monitoring Network (CAMN). The purpose of the network was twofold: (1) to fill a data gap by monitoring local air pollution levels in heavily impacted communities in Imperial County, where previously just five regulatory ambient air monitors were located within 11,600 square kilometers; and (2) to build tracking infrastructure and community capacity to collect and interpret air quality data in a trusted, timely, and relevant manner to support community actions to reduce exposures. Today, the network is fully community owned and operated, and includes 40 air monitors that collect and report real-time data on local air quality. 56
The Imperial CAMN shows how public health tracking can help strengthen resilience, address environmental health disparities, and promote health. Meaningful engagement of impacted residents ensured that the data collected would serve local priorities and support community actions. The five characteristics of actionable data described in Figure 1 are all addressed by the Imperial CAMN. Specifically, the data are as follows:
Timely: Real-time Imperial CAMN data have enabled rapid neighborhood responses to reduce exposure during poor air quality episodes. Local: Neighborhood-level data minimize geographic data gaps and allow for the identification of air pollution hot spots. Standardized: CAMN monitors are calibrated against regulatory monitors to ensure data quality and report consistent metrics across the network over time.
57
Accessible: Real-time CAMN data are reported on public websites and through e-mail alerts, increasing the availability of the data. Meaningful: Data are reported for communities of concern and presented in a way that is understandable to residents.
58
Figure 3 shows how the Imperial CAMN informed community actions to improve environment, health, and several dimensions of community resilience, based on the conceptual framework previously outlined in this article. Community participation in the CAMN's design and implementation, as well as a program to engage high school students in educating other community members, 59 deepened community members' understanding of how to interpret and use local air pollution data to protect health. 60 The community, equipped with CAMN data, also has been able to demonstrate to government officials that regulatory ambient air monitors were not adequately measuring dangerous spikes in pollution during peak pollution events. 61

Actions taken to reduce environmental health disparities based on data collected by the Imperial County CAMN. CAMN, Community Air Monitoring Network.
Lessons from the Imperial CAMN on the utility of community engagement in data collection and communications have potential applications for informing COVID-19 response efforts. In Figure 4, the conceptual framework for resilience in this article is used to outline a community-engaged approach to COVID-19 testing, contact tracing, data display and messaging, and policy planning. Building community engagement into the continuum of assessment, policy development, and assurance can increase community data literacy, trust, and adherence to public health messaging and policies. 62 Likewise, community-engaged risk assessment can counter rumors and misinformation about the COVID-19 outbreak. 63 Individual communities have taken steps toward a community-engaged response with targeted testing in high-risk communities, 64 community-based contact tracing, 65 and audience-oriented risk communications. 66

A community-engaged approach to COVID-19 testing, surveillance, and planning.
As an analogous example from the Imperial CAMN, local schools participating in a School Flag Program display flags according to a color-coded index used on a public-facing website to communicate air quality levels based on real-time monitoring data, and include accompanying risk communications—all of which were developed with community input. 67 Similar color-coded indices have been recently deployed by states, 68 cities, 69 and school districts 70 to communicate COVID-19 risk based on health indicators such as numbers of confirmed COVID-19 cases, hospital capacity, and test positivity rates. 71
Community participants in the Imperial CAMN indicate that the project strengthened two key community resilience measures, namely (1) increased capacity to gather, interpret, and use air quality data, and (2) increased community dialogue and engagement in governmental decision making. 72 , 73 The Imperial CAMN leveraged local knowledge and relationships that CCV staff had with community leaders, residents, and public health agencies to strengthen capacities that contribute to community resilience, such as building trust with school administrators to recruit local schools as monitor hosts; mutual co-learning with project partners through long-term collaborations with public health researchers 74 ; and increasing health literacy by developing and distributing community educational materials in English and Spanish to support meaningful engagement in the project. 75 The Imperial CAMN has also enhanced community economic resilience through funding and job training for monitor installation and maintenance; increased the political influence of residents by supporting expansion of community air monitoring in California through Assembly Bill 617 (AB617) 76 ; and created healthier air as community members participate in subsequent government-led planning to reduce pollution. 77 One community member concluded that “It has empowered me more by being able to express and defend our actions with good quality information. For example, we were able to identify areas where air quality was worse and then identify why and where it was coming from.” 78
The Imperial CAMN project provides an example of how public health tracking can be accomplished with effective community engagement to strengthen community resilience to future threats to public health. One project, however, cannot undo decades of socioeconomic disadvantage and entrenched health disparities, and the disproportionate vulnerability of Imperial county residents to the COVID-19 pandemic only underscores how vital it is that investment in public health tracking be conducted in a sustained as well as community-engaged manner.
The Imperial CAMN project could not have accomplished what it did if the air monitoring technology had been imposed from outside without significant investment in community learning, engagement, and capacity building. By investing in training local residents about air pollution, monitoring technology, and interpretation of data, and engaging the local community as equal partners in all phases of design and implementation of the CAMN, the project was able to make its public health approach responsive to local needs and circumstances, resulting in greater and longer lasting impact. This community-engaged approach is also critical to the gathering and sharing of COVID-19 data, as well as the design of public health interventions around COVID-19, particularly if strengthening resilience in the most vulnerable communities and addressing environmental health disparities is a desired outcome. Moreover, once the current crisis passes, long-term sustained investment in community-engaged public health tracking will be essential to preparing for the next public health emergency.
DISCUSSION
As the COVID-19 pandemic has demonstrated, without timely, local, standardized, accessible, and meaningful data, it is not possible to make the decisions needed—with the urgency needed—to mount an effective public health response. Investment in public health tracking is imperative, and it must not simply address the current crisis, or even prepare for the next crisis. Rather, agencies responsible for public health tracking should work in an equitable partnership with the communities they serve, to collect and report data that are relevant to community priorities and actionable for reducing health disparities and strengthening community resilience to withstand future crises. Elements of an equitable partnership with vulnerable communities include culturally appropriate community-centered outreach; meaningful involvement of residents in data collection and/or analysis; and mutual co-learning through long-term collaborations with research institutions. 79 Engaging with impacted communities throughout assessment, policy development, and assurance will increase the data's relevance and utility, and encourage community adherence to public health guidelines.
Beyond community engagement, several structural changes must occur within public health to improve data collection and reporting for local communities. First, public health tracking agencies must function independently to collect and report actionable data free of political influence. Second, data collection processes need to include characteristics on race and other socioeconomic factors for data disaggregation. Third, public health and the constituents it serves must address the tension between privacy and public health surveillance, to maintain individual privacy while not impeding the ability to collect and disseminate local and timely data.
Improvements in public health data will be limited without a sustained and committed investment in public health. Of the $3.6 trillion spent on health each year in the United States, only 3% is dedicated to public health. The Affordable Care Act had allocated the Prevention and Public Health Fund (PPHF) for “expanded and sustained investment in prevention and public health programs.” But the annual $2 billion budgeted for PPHF beginning in 2015 has never reached promised levels of funding. 80 Instead, funds have been allocated to other legislative priorities, including tax cuts and biomedical research. 81 In the meantime, local health departments have reported reducing their workforce by >56,000 staff nationwide since 2008. 82 A survey of >46,000 government public health workers in 50 states in 2017 showed an aging workforce with only 14% having a public health degree, and with 48% planning to leave or retire in the next 5 years with concerns about low pay as the leading reason. 83 Workforce depletion has gutted frontline data collection at many local and state agencies, and resulted in fewer personnel critical for establishing testing protocols, performing contact tracing, and disseminating data during infectious disease outbreaks.
All levels of government will be forced to make difficult budget decisions in response to COVID-19, and non-COVID-19-related public health data collection may be an appealing target for budget cuts. 84 Public health tracking is often invisible, and the cuts may not be immediately felt by constituents or may garner little attention—until the next public health crisis, such as a hurricane, heat wave, wildfire, or the discovery of contaminants leaching into a city's drinking water.
Rather than focusing on budget cuts, decision makers have an opportunity to use this crisis to reinvest in public health surveillance and community resilience initiatives, including public investments to boost the economy while building a modern public health infrastructure. There are myriad opportunities for investment, including improving the integration of data across clinical systems, including electronic health records 85 ; bolstering health surveillance efforts to gather more spatially and temporally refined data, through both health surveys and clinical data 86 ; investing in the personnel and technologies needed to expedite the processing of health data and move closer to real-time surveillance 87 ; and expansion and enforcement of reportable conditions. 88
Investments should also include funding community engagement as a routine function of all public health surveillance and response efforts 89 ; investing in emerging technologies for digital disease detection 90 ; and funding citizen science activities as a means of improving data collection, data literacy, and community engagement. 91
Finally, tackling the aforementioned investment opportunities will require rebuilding the nation's public health workforce. Focusing workforce development efforts in underrepresented and impacted communities 92 will bring new insights into public health surveillance, and bridge with efforts to improve community resilience.
CONCLUSION
Existing environmental health disparities—the unequal distribution of hazardous environmental exposures and related health conditions—have exacerbated the vulnerability of low-income and communities of color during the COVID-19 pandemic. Our current public health data infrastructure has not met the challenge of identifying and protecting vulnerable communities, nor of supporting a reduction in health disparities by addressing the underlying social and environmental conditions contributing to disproportionate disease burdens in these communities before the pandemic began. For these reasons, investments must be made in environmental and public health data tracking systems to restructure and realign these systems with community priorities to reduce health disparities and to strengthen community resilience before the next public health emergency.
Footnotes
ACKNOWLEDGMENTS
We thank Comite Civico del Valle, Imperial CAMN Community Steering Committee members, and our other Imperial CAMN project partners for the collective work described in this study. We also thank the members of our Tracking Implementation Advisory Group for providing multistakeholder guidance to inform our programmatic priorities and approach. We would also like to acknowledge the input of Paul English, Alexa Wilkie, and Michelle Wong on earlier drafts of this article.
AUTHOR DISCLOSURE STATEMENT
Several of the authors are paid staff members of Tracking California, which receives federal funding from CDC's Environmental Public Health Tracking Program and state funding through subcontracts with AB 617 Community Grants recipients. The authors have no other conflicts of interest to disclose.
FUNDING INFORMATION
The original Imperial CAMN was supported by the National Institute of Environmental Health Sciences of the National Institutes of Health under Award Number R01ES022722.