
Abstract
Social capital is widely recognized as health bolstering and more recently as playing a central role in family and community disaster response and recovery. Community social institutions may be considered a critical mechanism for the development of social capital, as they provide opportunities for community members to interact to build the networks and relationships that are necessary for taking collective action. In particular, social institutions may have a pivotal role to play in supporting children's health and welfare postdisaster. Community social institutions such as membership, civic, and religious organizations are community resources that stimulate learning and foster healthy child development. This study explores communities impacted by Hurricane Katrina and the Deepwater Horizon Oil Spill (DWHOS). Social institutions data were paired with household interviews from the Women and Their Children's Health Study (n = 521) to explore whether the density and type of community social institutions in the community were associated with child mental health outcomes. Multilevel logistic regression models examining the role of social institutions, household characteristics, maternal characteristics, and child-specific factors in child mental health showed that for each additional prosocial institution established in the community during recovery from Hurricane Katrina, respondents were 21% less likely to report a child mental health diagnosis (odds ratio 0.79; 95% confidence interval 0.63–0.98). These findings highlight the potential of investment in social institutions in communities to bolster resilience and foster meaningful recovery.
Introduction
In 1995, Putnam published an article titled “Bowling Alone,” in which he described the decline in civic participation, an essential element of a “strong and active civil society.” In this work, he described social capital as a consistent facilitator of cooperation, mutual trust, and coordination to act for mutual benefit. The title of the article referred to the observation that although 10% more Americans were bowling in the 1990s compared with the previous decade, participation in bowling leagues had declined by 40%. Notwithstanding declines in civic engagement, social institutions play a significant role in civic life and may be a critical mechanism for the development of social capital as they provide opportunities for community members to interact to build the networks and relationships that are necessary for taking collective action. 2
In the resilience activation model developed by Abramson et al., 3 a notional “marketplace” of social and civic institutions providing for the acquisition and exchange of resources was described. In such a marketplace, social institutions provide opportunities, along with other types of institutions such as schools and informal networks, for residents to interact. In particular, social institutions may have a pivotal role to play in supporting children's health and welfare after disaster disruption.
According to the Neighborhood Resources Model, 4 community social institutions are community resources that stimulate learning and foster a social environment that ensures the healthy development of children. These entities include schools and faith-based organizations, and community institutions such as libraries, civic groups, or membership organizations. 5 These organizations are increasingly being recognized for the critical indirect role they play in promoting community health. 6 Social networks and social capital have been studied in relation to postdisaster health and well-being. 7 Theoretically, we know that bonding, bridging, and linking social capital play a role in disaster recovery. 8 What is less well understood is the role that social institutions conducting activities unrelated to traditional disaster response play in the postdisaster context.
Disasters disrupt institutional life and social capital networks
Physical damage to buildings and infrastructure can reduce functionality of institutional spaces. Community needs that arise during disaster disruption often require a shift in the type or scale of work typically carried out by an institution requiring institutions to adapt to changing community needs. 9 Physical damage created by a disaster also disrupts social life. Individuals and families coping with a disaster may have less time and resources to engage with institutions and social networks, displacement fractures social networks and disrupts established networks of social capital, and individual and household level stress can shift engagement in social and civic life. 10
The Gulf Coast experiences persistent disaster risk and exposure. Between 2000 and 2019, 146 Major Disasters were declared by the Federal Emergency Management Agency (FEMA) in Gulf states (FEMA, n.d.). 11 Among those are multiple, significant catastrophic events that have impacted families, including Hurricanes Katrina, Irma, Harvey, and the Deepwater Horizon Oil Spill (DWHOS).
Child health and disasters
Child mental health consequences of disaster include: increased stress, fear, feelings of helplessness, outbursts, fear of separation from parents, trouble sleeping, irritability, anxiety, depression, and post-traumatic stress disorder. 12 Psychological response due to disaster exposure is part of a typical human stress response. Most children cope with acute stressors with support from social networks without treatment 13 ; however, some require additional supports to adjust. Pre-existing emotional or behavioral difficulties, negative coping, extent of disaster exposure, fear reactivity, regulatory ability, and coping skills influence child mental health after disasters. 14 Parental and household factors also influence child adjustment after disaster; parental reaction to the disasters, psychosocial functioning pre-events, distress postdisaster exposure, social support, and sense of community are parental-level risk factors of negative mental health outcomes in children. 15
In 2010, there were nearly 14 million children living in Gulf States. 16 In addition to acute disaster impacts, families in Gulf States are also more socially vulnerable than the U.S. population on average and face daily chronic stressors. All Gulf States report lower median income and higher rates of child poverty, public assistance, and food insecurity than the U.S. average. These are all indicators of the health vulnerabilities of children in the region, which are exacerbated when exposed to a disaster. 17
Links between social capital and health
Social capital is defined as “resources that are accessed by individuals as a result of their membership of a network or group.” 18 Social capital bolsters health at the individual level through access to information, instrumental support (e.g., borrowing money), and reinforcement or social affective support. At the social group level, social capital takes the form of social networks in a community and social contagion, informal social control, and collective efficacy. 19 Empirical research shows that social capital is consistently associated with health-related behaviors, physical and mental health outcomes, 20 and child development. 21 Social capital may promote or constrain healthy behaviors by promoting norms and attitudes, enhancing psychosocial functioning, providing access to resources or information, and biologically through activation of the hypothalamic–pituitary–adrenocortical 22 axis. 23
Children are dependent on their family, networks, and community institutions, therefore studying child mental health benefits from a socio-ecological approach. 24 We examine child mental health outcomes by using a socio-ecological framework of child mental health postdisaster (Fig. 1). The present analysis integrates several data sources to explore the role of social institutions as a proxy for social capital in promoting or protecting children's mental health. The outcome of child anxiety or depression is measured at a fixed point in time. We examine the changing landscape of social institutions, focusing on the exogenous factor of Hurricane Katrina recovery that with support from more than $13.4 billion in community development block grant funding created the opportunity to expand institutions before the DWHOS. 25 We hypothesize that greater social institutions will be associated with improved health outcomes even after adjusting for factors at the child, mother, and household levels.
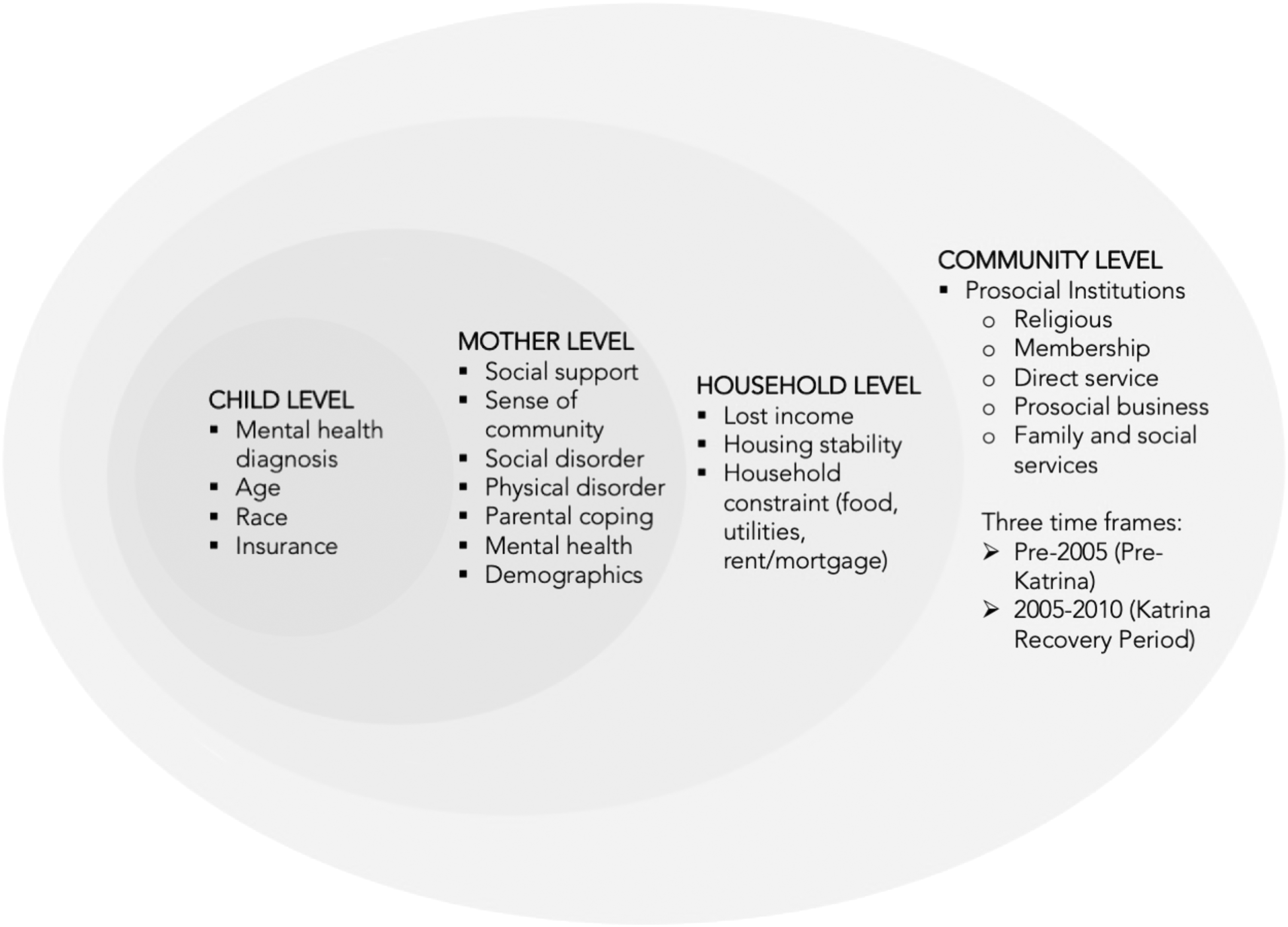
Ecological model of child mental health postdisaster.
Methods
Sample and data collection
The Women and Their Children's Health (WaTCH) Study collected longitudinal data from 2852 women in seven Parishes in South Louisiana on the health effects of the oil spill through telephone interviews conducted between July 2012 and August 2014 and face-to-face interviews conducted between July 2012 and October 2014. Detailed study methodology has been published elsewhere. 26 Social institutions data were paired with family data, resulting in a sample of 521 mother–child dyads from the WaTCH Study for the present analysis.
Measures
Child level
Child anxiety or depression was assessed by asking mothers whether a doctor or health professional had ever told them that their child had depression or anxiety problems (yes/no). Demographic characteristics included child health insurance (yes/no), child race (White, African American, Multiracial, Other), and child age (10–13, 14–17).
Mother level
Social support was measured by five questions that assessed perceived functional support predicated on having someone in their network whom they could count on for everyday favors such as a ride, to take care of them if ill, to lend money for a medical emergency, to talk to about troubles with a family relationship, and to help locate housing if they had to move. Consistent with past research studies, respondents who indicated having fewer than two of these supports were classified as having low or no social support. 27
Sense of community was measured by using the 12-item Sense of Community Index (SCI); the median score was used to categorize respondents into low and high measures of the SCI. 28 Coping with parental demands was assessed by asking mothers to indicate in general how well they are coping with the day-to-day demands of parenting and raising children (very well, somewhat well, not very well, not well at all). Maternal mental health was assessed by using the Kessler-6. Consistent with literature on scoring the Kessler-6, a score of 13 or higher indicates probable serious psychological distress (SPD). 29
Perceived neighborhood physical and social disorder was assessed by asking respondents about their level of concern about neighborhood issues such as concern about letting children play outside or having property stolen among other issues on a scale of 1 to 10. Items were grouped and scored into physical and social disorder summary scores. Consistent with the ecometric work of Sampson et al., physical and social disorders were categorized into three levels by using even cutoff points (rarely or not concerned, moderately concerned, or very concerned). 30 Demographic characteristics included mother employed (yes/no), education (<high school, high school/GED, some college, college graduate), age, and marital status (married, widowed, divorced, separated, living with partner, never married).
Household level
Income was assessed by asking mothers to report on their total household income in the previous year before the oil spill (<$10,000, $10,000–20,000, $20,000–30,000, $30,000–40,000, $40,000–50,000, $50,000–60,000, $60,000–70,000, $70,000–80,000, $80,000–90,000, $90,000–100,000, >$100,000). Housing stability was measured by asking respondents whether they had lived in a permanent place at any time since the oil spill (yes/no). Household constraint was assessed by asking respondents to indicate whether they had not had enough money for rent or mortgage, utilities, or food in the past 3 months. Respondents indicating trouble with affording one or more of these essentials were categorized as financially constrained.
Community level
Social institutions measures were computed by using social institutions data downloaded from the Dun and Bradstreet Million Dollar Database in July 2017. Data were collected on all institutions with the Standardized Industry Classification (SIC) codes for Services and Public Administration (70–99) for the state of Louisiana from 1700 to 2010 (n = 105,267). 31 Social institutions measures were aggregated at the census block group level for total number religious, membership, direct services, prosocial businesses, and social and family services, and they were adjusted for population density as rates per 100,000 population. Census block groups typically are subdivisions of census tracts, include ∼600–3000 people, and cover a contiguous area. 32 A total prosocial institutions measure was computed, summing all the groups into one summary measure and for two timeframes pre-2005 (representing the pre-Katrina institutional landscape) and 2005–2010 (reflecting the institutions that were begun in the short-term recovery period after Katrina). See Table 1 for examples of each type of organization included in the social institutions measures.
Social Institution Categories
Data analysis
Hierarchical logistic regression models were fit to assess the associations between mother, household, and community-level factors with the outcome child anxiety or depression. 33 First, a Pearson chi-square statistic was computed to determine which of the mother and household level factors were independently associated with the outcome child anxiety or depression. An unadjusted logistic regression model was computed for each community social institution measure for three timeframes. Factors independently associated at each level with child anxiety or depression were included in a series of stepwise logistic regression models. The log-likelihood, Akaike information criterion, and Bayesian information criterion tests were performed to determine the best-fitting model. 34 Stata version 16 and ArcGIS version 10.1 were used to complete analyses. 35 Institutional Review Boards at Columbia University, New York University, and Louisiana State University reviewed and approved this research.
Results
More than 15% of children in the sample had anxiety or depression according to maternal report (n = 95), and 17% of mothers reported SPD (n = 105) (Table 2). Nearly three-quarters of respondents expressed concern (n = 449, 72%) about social disorder. Nearly 12% of study participants reported unstable housing (n = 74), and 13.3% reported constrained household resources (n = 82). In parishes where study participants resided, the mean number of prosocial institutions was 3.55 per 100,000 population (SD 3.35; Table 3). Before 2005, the greatest proportion of institutions established was religious (mean 0.94, SD 1.22). Between 2005 and 2010, the greatest number of organizations established was membership (mean 0.66, SD 1.14).
Sample Characteristics
SCI, Sense of Community Index; SPD, serious psychological distress.
Mean Social Institutions in Each Census Block Group
CBG, census block group; SD, standard deviation.
Bivariate analysis showed that social support, parental coping, maternal SPD, neighborhood physical disorder, income, household constraint, and mother education, age, and marital status were all independently associated with child anxiety or depression (Table 4). Total prosocial institutions and membership organizations established in 2005–2010 were statistically significantly associated with child anxiety or depression (Table 5).
Bivariate Association Between Mother, Household, and Demographic Characteristics and Child Mental Health Diagnosis
Bolded values are statistically significant with a 95% Confidence Interval (p < 0.05).
T-test.
Fisher's exact test.
MH, mental health.
Association Between Community Social Institutions and Child Mental Health Diagnosis, Adjusted for 2010 Population Density
Statistical significance.
CI, confidence interval; OR, odds ratio.
Multilevel logistic regression models (Table 6) showed that parental coping and strong social support were protective against child anxiety or depression whereas maternal psychological distress was a risk factor (Model 1). As parent coping improved, respondents were 55% less likely to report child anxiety or depression (odds ratio [OR] 0.45, 95% confidence interval [CI] 0.29–0.70). Mothers with SPD were twice as likely to report a child with anxiety or depression (OR 2.37, 95% CI 1.31–4.31), and mothers reporting strong social support were 57% less likely to report child anxiety or depression (OR 0.43, 95% CI 0.25–0.75).
Association Between Mother, Household, Demographic, and Community Characteristics and Child Mental Health Diagnosis Adjusted for Population Density (Multilevel Logistic Regression, Odds Ratios Reported)
Bolded values are statistically significant with a 95% Confidence Interval (p < 0.05).
AIC, Akaike information criterion; BIC, Bayesian information criterion.
In models two and three, household- and mother-level demographic factors were not significant predictors of child anxiety or depression. On postestimation testing; household and mother-level variables did not strengthen the model and were not retained. In model four, total prosocial institutions were associated with child anxiety or depression and did not explain away any of the maternal level factors. For each additional prosocial institution in the community, children were 21% less likely to have anxiety or depression (OR 0.79, 95% CI 0.63–0.98). Model five examined membership organizations within the umbrella group of total prosocial institutions. For each of the additional membership organizations, mothers were 32% less likely (OR 0.68, 95% CI 0.48–0.97) to report child anxiety or depression whereas parent coping and social support remained protective and maternal SPD remained a risk factor.
Discussion
Mother-level factors of coping, social support, and mental health distress persist in explaining variation in child anxiety or depression throughout each level of analysis. Household and demographic characteristics were not explanatory and did not strengthen the model of child anxiety or depression after the DWHOS. At the community level, total social institutions established between 2005 and 2010 as well as membership organizations established between 2005 and 2010 are protective against child anxiety or depression—this period refers to organizations established during the recovery period from Hurricane Katrina and leading up to the DWHOS. Examples of membership organizations include: recreation, civic, social, dwelling-based, and labor organizations and business and professional associations.
A longitudinal study examining crime in 264 cities in the United States from the 1990s to 2010s found that additional social institutions focusing on nonprofit organizations that work in “community life” lead to reduced crimes rates. 36 Our findings, in a sample of families recovering from the DWHOS, while examining a much shorter time frame, provide further evidence that community institutions may play a critical role in improving community health and well-being and bolstering resilience. Community social institutions provide opportunities for community members to come together to interact, establish connections, and build social support. Leveraging the role that social institutions play in communities providing non-disaster-related community services is a critical lever for building community capacity and resilience in the preparedness, response, and recovery phases of disaster.
This study quantified social institutions at the census block group level by using SIC classifications. In pairing household interview data with the administrative level of social institutions, we are able to comprehensively include social institutions across vast geographies. The counterbalance to this level of data is detailed information on household and community interactions with social institutions. Additional research is needed to explore how organizational capacity relates to associations between health outcomes and service types, community integration, constituency served, and neighborhood tenure in disaster-affected settings to understand how families and institutions interact and support each other during disaster recovery.
Preparedness efforts could include policies, programs, and funding dedicated to establishing membership organizations and to building capacity within those organizations as a community development approach to increasing resilience. This could serve the dual purpose of increasing community capacity and reducing vulnerability at the community level in the absence of a disaster threat while also resulting in resilience when faced with a disaster or disruption.
The association between institutions established between 2005 and 2010 and child health is an interesting finding, as these were the first 5 years of investment in recovery from Hurricane Katrina in Louisiana. These findings support the notion that investments made during Hurricane Katrina recovery are working to increase community resilience to a future disaster event, in this case the DWHOS. Additional funding and efforts during long-term recovery to bolster community institutions is a strategy to ensure increased resilience and capacity in future disaster events. This is critical in areas at persistent risk for frequent disasters, such as those experienced along the Gulf Coast. Future research examining the role of investment during disaster recovery in future disaster resilience as well as in evidence-based approaches to bolstering community institutions and social support are critical for improving disaster outcomes for children, families, and communities.
This article on factors associated with child anxiety or depression is preliminary, and findings should be interpreted with the study limitations in mind. Community-level social institutions are the only community-level variables included in the analysis. Additional community-level characteristics need to be examined to better understand contextual effects on child health outcomes, including data on how people within a community interact with institutions. The outcome measure of child anxiety or depression was captured with a single item reported by mothers, thereby limiting the psychometric reliability. Further, mothers were asked to report on what they had been told by a doctor or health professional regarding their child's anxiety or depression, a potential source of recall bias. Methodologically, this analysis includes a large number of singleton households residing in a census block group. There is little guidance on sample size recommendations for nested study designs. 37 Within the context of these limitations, the finding that greater social institutions established during the recovery period from Hurricane Katrina are associated with reduced odds of a child's mental health diagnosis advances our understanding of the role of community institutions in disaster recovery processes.
This examination of the ecological association of social and civic institutions with the psychological and emotional states of disaster-exposed children suggests that children's mental health may be attributable to more than their own psychological or biological characteristics, their caregivers' mental health, and household constraints. It was noteworthy that the presence and density of prosocial institutions established in Katrina's aftermath were most strongly associated with this effect on children. These agencies, in particular, may have been founded with a particular trauma-informed focus in mind. Moreover, many of these prosocial institutions founded in Katrina's aftermath were predicated on principles of community engagement, with notional missions of cultivating collective self-efficacy: in a sense, helping people to “bowl together” rather than “bowl alone.” Further research is warranted to explore these associations, and their potential etiology.
Footnotes
Acknowledgments
The authors gratefully acknowledge the WaTCH study participants, the community advisory board, and the study support staff. In addition, the authors acknowledge the critical support of the study's Principal Investigator, Edward Trapido, as well as our co-investigators Edward Peters, Ariane Rung, Elizabeth TH Fontham, Lori Peek, and Jaishree Beedasy.
Author Disclosure Statement
No competing financial interests exist.
Funding Information
This research was funded by the National Institute of Environmental Health Sciences (1U01ES021497).