
Abstract
We study the interrelationships between health, residential segregation, and disaster-related material losses (income loss, job loss, economic/property damages) due to the worst ever man-made disaster of its kind, the Deepwater Horizon oil spill (DHOS). Social, economic, and health consequences of the DHOS disaster were assessed in the Survey of Trauma, Resilience, and Opportunity among Neighborhoods in the Gulf, a population-representative study of adults aged 18 years and older living in coastal counties of the Gulf of Mexico in 2016, about 6 years after the disaster. We found that odds of poor/fair health was nearly three times higher among adults who reported DHOS property damage than among those without this material loss using logistic regression models that controlled for individual-level social determinants of health (race/ethnicity, age, gender, marital status, education, household income, and employment) and adjusted for the multilevel structure of the data. Considering alternative measures of residential segregation by race and income (including dissimilarity, exposure, and polarization or concentration at the extremes), only zip code-level income polarization interacted with DHOS material loss to widen inequalities in health. Damage-related health differences were statistically indistinguishable for zip codes with increasingly concentrated affluence, but damage-related health differences widened rapidly with increasingly concentrated disadvantage. At the maximum (1.6 standard deviations below the mean), nearly three-quarters of adults with damages reported poor/fair health versus less than one-third of those with no damages. Our findings suggest that environmental disaster, through disaster-related material loss, both activates and exacerbates existing social and spatial stratification of health.
Introduction
Decades of research shows that the negative social, economic, and health consequences of disasters occur most frequently and with the most severe impacts among the most disadvantaged individuals and communities. These unequal impacts of disaster may further set in motion cycles of disadvantage, poverty traps, and other forms of accumulating disadvantages in which individual hardships are amplified by earlier unequal impacts of disaster that are manifest in the social and spatial stratification of communities. For example, on a global scale, the adverse economic and health consequences of environmental disasters are recognized as being concentrated among poorer and more unequal nations. 1 In the United States, the geographic distribution of environmental hazards has been associated both with state- and county-level differences in income inequality 2 ; racially and economically stratified population changes 3 , 4 ; and race and class inequalities in who is able to leave, where they go, who stays, who returns, and who and where housing, infrastructure, and jobs are rebuilt. 5 The possibility of both increasing scale and scope for environmental disaster due to climate change suggests that their contribution to population stratification may be becoming increasingly important. However, surprisingly little is known about the role of disaster in the social and spatial stratification of health that is not subjected to limitations (e.g., ecological fallacy and individual-level confounding) 6 that decades of research on the cross-level (neighborhood-to-individual) mechanisms of social and spatial stratification of health has identified and sought resolve. 7 , 8 , 9 In this study, we evaluate how disaster may illuminate existing systems of stratification and even amplify social and spatial stratification of health.
Over the last several decades, research on social determinants of health has expanded rapidly to provide increasingly stronger empirical evidence on the multilevel processes through which health is socially and spatially stratified. Grounded in social ecology, this research traces multilevel pathways from macrostructural conditions through increasingly more localized social processes thought to generate inequitable distribution of health-related resources and insults. We refer to this literature as area effect research—grouping together a body of work across the social sciences and public health, which increased rapidly over the last decades of the 21st century due to the elimination of technological barriers (e.g., statistical methods, data linkage capacity) to testing social–ecological hypotheses. 10 However, it is only recently that studies have begun to extend multilevel area effects research to explore the macro-to-micro pathways through which environmental hazards may generate accumulating disadvantages in individual well-being 11 —thus far, focusing only on economic outcomes. 12 Multilevel research linking environmental disaster with the stratification of health has the potential to reenergize and extend research on the stratification of health more broadly.
A seminal finding from the area effect research on social determinants of health has been that the spatial stratification mechanism of residential segregation is the “fundamental cause” 13 linking macrostructural conditions (of prejudice and injustice) to individual health disparities by race and class. 14 , 15 , 16 Theoretical debate about these findings has clarified distinctions between—on the one hand—potential manifest, material mechanisms of social determinants of health, 17 —and on the other hand—perceived psychosocial pathways. 18 , 19 Furthermore, this literature has found that differences in health (assessed using a broad-based self-assessment of health 20 ) associated with areal measures of stratification (e.g., segregation) can in large part be explained by (and in small samples sometimes cannot be distinguished from) individual-level material circumstances. 21 , 22 , 23 Moreover, the unraveling of social and spatial stratification dynamics in a population requires careful attention to the potentially independent and interdependent role of material circumstances as a proximal factor (in the pathway between racism, segregation, and individual well-being), which can be both a product of exposure to residential segregation and determinant of residing in a segregated community.
Critical research questions tested by these studies have been whether correlations between spatial inequality and health observed using aggregated data (like those that have thus far predominated research on disaster and spatial inequality and health) persist when studied using multilevel data. The alternative mechanisms thought to link spatial inequality (indexed by segregation) and poor health are: (1) material and indirect, operating through unequal opportunity, whereby individuals access material resources gained personally or through their family and network shapes health; or (2) psychosocial and direct, operating through psycho-neurobiological processes (wherein anger, shame, and hostility triggers physiological dysregulation) or the absence of social support to buffer these processes that generate poor health among both affluent and poor individuals. Moreover, life course, social ecology theory on “accumulating disadvantages” motivates (3) a feedback mechanism that stratification by race and class (e.g., income) interacts over space (e.g., cross-level neighborhood–individual interactions) and/or time to generate feedback systems that widen inequalities. 24 , 25
In contrast with the larger body of population health research, with notable exceptions, 26 , 27 , 28 , 29 much of the area effect research on disaster and social determinants of health offers little engagement with the previously described debate about psychosocial and neomaterialist explanations for the interplay between social and spatial stratification of health. Particularly in multilevel research exploring how the places in which people live may precipitate, amplify, or buffer the individual health consequences of disaster, studies have highlighted psychosocial processes (e.g., stress, trust, support, and coping). This includes, for example, area effect research on social capital (social support, social cohesion, collective efficacy, and community attachment) as a buffer between environmental disaster and individual health. 30 , 31 , 32 , 33 , 34 , 35 , 36 , 37 Even in the selection of outcomes, disaster research has tended to focus on mental and behavioral health outcomes (e.g., depression, substance abuse), which may in fact be the most important mechanisms of disaster, but remain only a subset of the ways social stratification might “get under the skin.” 38 In the broader population health literature, there has been a fairly balanced exploration of both the “material mechanisms” of social determinants of health and the “psychosocial mechanisms,” and increasingly, there is attention to their potential interdependency. 39
Strong scientific foundations exist for hypothesizing that environmental disaster provides a means to better understand how well-being—in its social, economic, and health dimensions—may become socially and spatially stratified. At the neighborhood level, there has been considerable attention to the measurement of community resilience and vulnerability to disaster (although usually using measures of central tendency rather than distributional measures of social and spatial inequality—like residential segregation), and a growing branch of “validation studies” exploring whether these typically county-level measures “predict” county-level disaster impacts (e.g., death rates 40 ). At the individual level, there is also a large body of research testing the material mechanisms of social determinants of health that employs disaster events as natural experiments in which material conditions are “exogenously shocked” allowing researchers the opportunity to improve inferences about the “causal” impact of material conditions on individual health, socioeconomic attainment, and mobility. 41 Finally, area effect research offers strong theoretical and empirical grounding for selecting segregation by race and income as spatial stratification measures that capture the distribution of vulnerability and resilience, including recent studies that have illuminated the potentially unique importance of their interdependence as widening economic inequality is racially polarized. 42 , 43
Man-made environmental disasters may provide a unique opportunity to examine these processes. For example, exogenous the Deepwater Horizon oil spill (DHOS), which impacted community along the Gulf of Mexico, is widely recognized to have been the largest marine petroleum release in history. From a psychosocial perspective, studies suggest that this disaster generated unique forms of discord and division within communities, 44 , 45 , 46 From a neomaterialist perspective, DHOS studies have suggested that material losses may be the mechanism through which people's health has been affected, 47 a finding which is consistent in the year after the spill 48 and 6 years later. 49 , 50
Our overall objective was to begin to trace the potential multilevel and accumulative macro-to-micro population dynamics linking environmental disaster, place-based systems of social stratification, and social disparities in health. Due to the considerable body of research exploring psychosocial mechanisms, we focus on strengthening evidence for the material mechanism, which we observe here as individual material loss due to the DHOS. We evaluate whether disaster-related change in material circumstances operates independent of existing individual-level social determinants of health (Hypothesis 1). Then, we explore whether disaster widens existing social and spatial stratification systems through feedback that accumulates over spatial levels: specifically, whether there is cross-level interaction between individual material loss and zip code-level residential segregation that widens inequalities in health (Hypothesis 2). We thus explore the relationship between individual health, individual material loss due to the DHOS, and residential segregation of zip codes as potentially operating through both individual-level mechanisms and cross-level (individual–neighborhood) feedback mechanisms, and we test whether disaster simply reflects or actually exacerbates social and spatial stratification of health.
Methods
Participants
The Survey of Trauma, Resilience, and Opportunity among Neighborhoods in the Gulf (STRONG) collected a population-representative sample of 2520 adults aged 18 years and older living in coastal counties and parishes along the Gulf of Mexico in 2016, about 6 years after the DHOS. This study was approved by the RAND Human Subjects Protection Committee. The stratified sampling methods and construction of survey sample weights have been detailed elsewhere. 51 In summary, county-based stratified sampling of landline and cell phone users was conducted, with random sampling of wireless service phone number banks and random digit dialing to capture listed and unlisted landlines. Response rates for the Gulf Coast states employed in this analysis (i.e., Alabama, 16.3%; Florida, 11.6%; Louisiana, 17.8%; and Mississippi, 18.0%) were equivalent or better than national trends in randomized phone surveying. 52 Due to comparatively low response rates for Texas (1.3%), for which surveying was subcontracted, Texas was excluded. From the non-Texas Gulf of Mexico sample (n = 1897; henceforth Gulf Coast), respondents with item nonresponse on income (n = 321), DHOS material loss (48), or other items (n = 30) were excluded. The final sample included 1498 participants.
Measures
Self-rated health
Self-rated health is assessed using the question “In general, would you say that your health is excellent, very good, good, fair, or poor.” We employ a dichotomous indicator for “fair” or “poor” health, henceforth “poor/fair health.” This is a common and valid way to operationalize scales of self-reported health, 53 which offered the best trade-off between accuracy and precision for our aims.
Migration history
Migration history is assessed using a series of questions about respondents' current residence (state, county/parish, zip code), whether they “live[d] in [that county/parish] at the time” of the DHOS and if not where (state, county/parish) they did live. We categorize respondents as: in-migrants to the Gulf Coast since the disaster, internal migrants who moved between Gulf Coast counties since the disaster, and Gulf Coast nonmigrants. 54
DHOS material losses
DHOS material losses are assessed among all respondents who were residing in Gulf Coast counties at the time of the DHOS (i.e., not assessed among Gulf Coast in-migrants) using three questions from a series about direct and indirect exposures attributed to the DHOS, specifically: “Did you or any member of your immediate family have any property that was lost or damaged because of the DHOS or clean-up?”; “Did the DHOS lead you to lose money?” and “Did the DHOS lead you to lose your job or work fewer hours?” In order for respective loss variables to be observed for the entire sample, we included a category for in-migrants to the Gulf Coast (who were not asked about DHOS losses). Also for job loss, we distinguished respondents reporting they were not employed (“retired,” “unemployed,” or “disabled”) at the time of the DHOS.
Residential segregation
Residential segregation at the time of the DHOS was measured for respondents categorized above as nonmigrants using the most granular geographic information available—zip code. 55 More granular measures have been shown elsewhere to be more strongly associated with health. 56 , 57 Residential polarization of income was assessed using the index of concentration at the extremes (ICE), a measure developed to offer a simple method for capturing the spatial concentration of affluence versus disadvantage. 58 , 59 Residential segregation by race/ethnicity and poverty status was measured along its two conceptual dimensions—evenness and exposure—respectively, using the index of dissimilarity and index of exposure. 60 , 61 We calculated the indices using Census Bureau data closest in time to the DHOS (i.e., for dissimilarity and exposure, block-group-level data for the respondent's zip code from the 2010 Census and 2009–2013 American Community Survey [ACS], and for the ICE, zip code-level data from 2006 to 2011 ACS). 62 For sensitivity analyses, we assessed the sociodemographic composition of the respondent's zip code and income equality (Gini coefficient) for the county from 2006 to 2011 ACS.
Individual sociodemographic characteristics
Individual sociodemographic characteristics include race/ethnicity, gender, as well as current age, educational attainment, marital status, household income category, and labor market participation.
Statistical analysis
We use a multilevel approach to fitting logistic regression models to evaluate: Hypothesis 1: whether DHOS material losses are associated with individual health, independent of other individual-level social determinants of health; and Hypothesis 2: whether there are cross-level interactions between individual's DHOS material loss and zip code measures of social and spatial stratification (i.e., residential segregation by race/ethnicity or income). All analyses employ sample weights constructed to produce population-generalizable estimates and adjust standard errors for clustering of respondents within zip codes, that is, we employ Stata 15.1 “svy” commands for complex survey design data analysis. 63 We evaluate the improvement to model fit of variables or sets of variables using adjusted Wald tests for complex survey data. Due to the challenges in appropriately interpreting interactions in nonlinear regression models, 64 we report log odds for all models, and for models with interactions, we estimate predicted probabilities and differences in predicted probabilities of poor/fair health, as well as the standard errors and 95% confidence intervals (CIs). We estimate these statistics using the Stata “margins” commands, which apply the delta method to calculate standard errors and CIs.
Results
Sample descriptive statistics
One-quarter of Gulf Coast adults report poor (8%) or fair (17%) self-rated health, henceforth, poor/fair health. Non-Hispanic Black (15%) and Hispanic (10%) adults comprise one-quarter of the sample, with 72% non-Hispanic White (Table 1). The gender distribution is about equal and average age is 50 years. About half of adults are currently married, with never (24%) and formerly married adults (28%) almost equally divided. More than half of adults have, respectively: greater than a high school education (59%); household income at least $40,000 (59%); and employment that is either full time (44%) or part-time (9%). Since the DHOS, about 17% of adults had moved into the Gulf Coast, with relatively few internal migrations between Gulf Coast counties/parishes (4%). Among adults who were residing in the same coastal county/parish in 2016 as at the DHOS, the most common material loss was financial (23%), closely followed by loss of job or hours (22% of those employed at DHOS), and about 5% reported property damage due to the DHOS. 65
Descriptive Statistics for the Survey of Trauma, Resilience, and Opportunity Among Neighborhoods in the Gulf, 2016
DHOS, Deepwater Horizon oil spill; ICE, index of concentration at the extremes.
The subsample of respondents who had remained in the same county or parish since DHOS (n = 1281) had a sociodemographic distribution similar to the sampled population. According to conventional standards for interpreting dissimilarity, 66 this subsample's average non-Hispanic White/non-Hispanic Black dissimilarity is moderate, as is the poverty dissimilarity. Exposure indices are on average less than 0.2 and given observed skew, logged for subsequent analyses. The average ICE is nearly at the midpoint of the possible range from −1.0 to +1.0, indicating that on average zip code shares of affluence and disadvantage are about evenly balanced.
Poor/fair health and DHOS material loss
Table 2 presents the test of potential material loss pathways linking disaster to poor health (Hypothesis 1). We first report the log odds of poor/fair health associated with individual characteristics conceptualized as social determinants of health (Model 1) and then assess independent associations with DHOS material losses (Models 2–4). Although all forms of material loss were associated with poor/fair health in bivariate associations (data not shown), after adjusting individual-level social determinants of health, only respondents who reported that they or their family experienced property damage were statistically significantly more likely to report poor/fair health. The odds of poor/fair health is nearly three times greater among adults experiencing property damage than among adults residing in the Gulf Coast at the time of the DHOS who did not [odds ratio (OR) = exp(1.01) = 2.75]. In-migrants after DHOS had significantly reduced odds of poor/fair health relative to those with damage (data not shown, OR = 0.22, 95% CI: 0.08–0.63), but did not reach statistical significance relative to those without (Table 1). Differentials associated with property damage were largely independent of, and at least as big as, those for social determinants of health including education, income, employment, and (to a lesser extent) race/ethnicity. For example, recognizing that log odds of −0.7 equates to an OR of 0.5, we observe odds of poor/fair health in both Model 1 and Models 2–4 that were (1) reduced by about half for adults with some college relative to high school and by about half again for those with at least a bachelor's degree; (2) reduced by nearly half if the household earned $20,000–$39,000 versus less than $20,000 and by a third for the top two income categories; and (3) over three times higher for respondents out of the labor market than full-time employed.
Log Odds of Poor Self-Rated Health Associated with Sociodemographic Characteristics and Exposure to Material Loss Due to the Deepwater Horizon Oil Spill
Data are from the Survey of Trauma, Resilience, and Opportunity among Neighborhoods in the Gulf 2016. Logistic regression models adjust for sampling weights and clustering of respondents within zip codes. Parentheses contain 95% CIs.
p < 0.05.
p < 0.01.
p < 0.001.
p < 0.10.
CI, confidence interval.
Poor/fair health, material loss, and residential segregation
Table 3 presents models testing the interaction between property damage material loss and residential segregation at the time of the DHOS (Hypothesis 2). The sample is restricted to respondents who had not moved into the Gulf Coast or between Gulf Coast counties since DHOS. We find that poor/fair health is not associated with the dissimilarity indices (Models 5–6). Among the exposure indices (Models 7–8), poor/fair health is independently associated with poverty exposure, but the index does not significantly interact with property damage (Model 8). Only the ICE index is both independently and interactively associated with property damage (Model 9).
Log Odds of Poor/Fair Self-Rated Health Associated with Property Damage, Residential Segregation, and Their Interaction, Controlling for Sociodemographic Characteristics
Data are from the Survey of Trauma, Resilience, and Opportunity among Neighborhoods in the Gulf 2016. All logistic regression models include covariates not shown to control for respondent's race/ethnicity, gender, age, marital status, education, income, employment. Models adjust for sampling weights and clustering of respondents within zip codes. Parentheses contain 95% CIs.
p < 0.01.
p < 0.10.
p < 0.05.
In Figure 1, we depict the findings from Model 9 illustrating how the gap in poor/fair health between those who did and did not experience DHOS-related property loss is significantly magnified by the extent of ICE. The figure shows spatial stratification: the predicted probability of poor/fair health increases with increasingly more negative ICE (i.e., greater concentration at the lower extreme). Most striking, however, is the evidence supporting a cross-level feedback mechanism for widening inequalities (i.e., accumulating disadvantages) that the trend is much stronger for respondents who reported experiencing DHOS-related property loss. In fact, this material loss is associated with poor/fair health, but only when low-income households outnumber high-income households in the respondent's zip code.
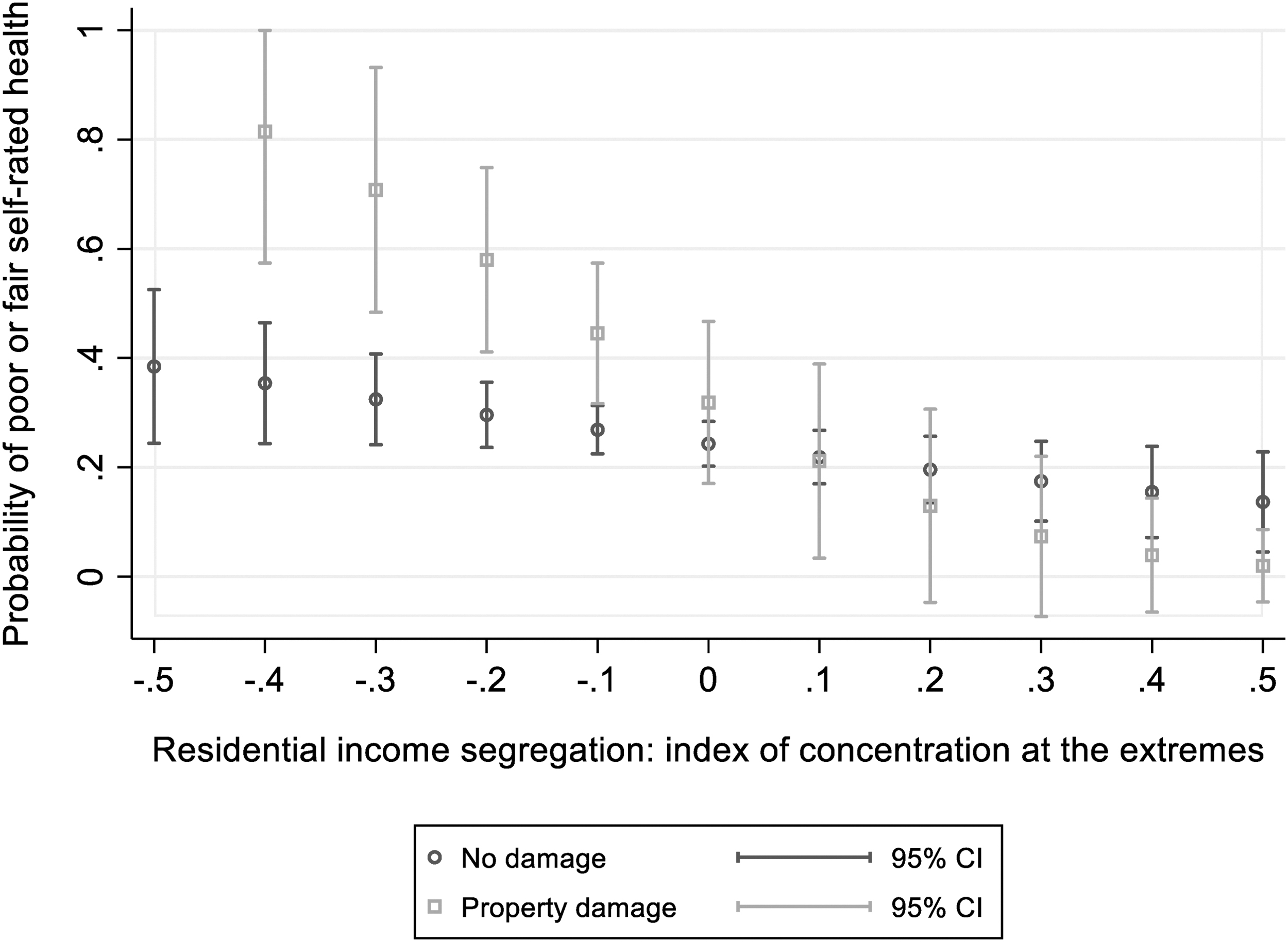
Predicted probability of poor self-rated health by experience of DHOS property damage and income segregation of zip code at the time of the DHOS. Predicted from Model 9 of poor/fair self-rated health with covariates for DHOS property damage, residential income segregation (i.e., index of concentration at the extremes of income), interaction of damage × segregation, and individual and household DHOS (race/ethnicity, gender, age, marital status, education, income, and employment status), which are set to their mean value for the prediction. All statistics are sample weighted and adjust for clustering of respondents within zip codes. CI, confidence interval; DHOS, Deepwater Horizon oil spill.
For example, if we hold constant all assessed individual-level sociodemographic characteristics (i.e., set them to the sample mean), the predicted probability of poor/fair health for individuals residing in communities with an ICE of −0.3 (i.e., the percentage of low-income households exceeds high-income households by 30 percentage points) is 71% among those who reported the DHOS-related property damage (95% CI: 11%–93%) compared with only about 32% for those who did not experience property damage (95% CI: 4%–41%). When ICE is skewed toward low incomes to this extent, exposure to property damage is associated with about a 39 percentage point difference in the probability of poor/fair health (95% CI: 16.7%–58.8%). However, when ICE is equally and oppositely skewed toward high incomes (e.g., ICE = +0.3), the predicted probability of poor/fair health is less than 20% irrespective of property damage, and the difference in poor/fair health is statistically indistinguishable (at about 10%). The figure thus supports the hypothesis that disaster generates a cross-level feedback system of accumulating disadvantages in which individual material loss (property damage) interacts (crossing or accumulating over spatial levels) with zip code residential segregation (ICE) to widen the social and spatial stratification of health.
Sensitivity tests
In sensitivity tests (Appendix Table A1), ICE better predicted poor/fair health than various indicators of sociodemographic composition of zip codes (i.e., housing value, or percentage non-Hispanic Black, Hispanic, unemployed, no vehicle, employed in the occupational category most impacted by DHOS—agriculture, forestry, fishing, hunting, and mining, vacant housing, or rural; Models A1–A9), including zip code median household income (logged; Model A3). It also predicted poor/fair health better than an alternative income segregation measure at a higher, less granular spatial level (i.e., county Gini coefficient for household income inequality; Model A10). Moreover, inclusion of interactions between the respondents' own income and property damage (which were not statistically significant) did not change the strength or significance of the interaction between income concentration and property damage (Appendix Table A1, Model A11).
Discussion
We find that 6 years after the DHOS the experience of property damage due to the disaster continues to distinguish self-rated health in a nationally representative sample of Gulf Coast adults. Moreover, this type of material loss considerably widens health disparities associated with residential income segregation. Fair/poor health was observed in about 70% of adults who experienced DHOS economic or property damages and were living, at the time of the DHOS, in a zip code with concentrated income disadvantages (ICE = −0.30). By comparison, fair/poor health was observed in only 30% of adults who had not experienced DHOS property damage but who had experienced similar levels of concentrated income disadvantage at the time of DHOS. Furthermore, for adults living in nonpolarized zip codes or those with concentrated affluence, there were no damaged-related differences in health, irrespective of material loss, that is, about 20% of all adults reported poor/fair health. The observed magnitude of disparities we observe and indications of their persistence (i.e., the survey was fielded 6 years after DHOS) lend support and motivate new directions for research focusing on material mechanisms and multilevel feedback.
Our findings extend to research on environmental disaster, the more widely observed findings from social determinants of health, that (1) health differences associated with communities—and specifically the spatial concentration of material disadvantage at a subcounty level—operate independent of adults' increased exposure to poor material conditions and material loss in these communities; and (2) these community conditions magnify differentials in health associated with these material circumstances. This is important because previous multilevel research on disaster has generally reported weaker and more inconsistent associations with community conditions than observed more broadly in multilevel social determinants of health. 67 Our findings suggest that one explanation may be the predominance of county-level indicators and indices of social vulnerability that measure composition (but do so with insufficient spatial granularity) and generally do not incorporate measures of residential segregation (which capture the inequality of more spatially granular composition). Thus, our findings are the first to build on earlier work finding more speculative evidence that economic segregation operated as a community-level social determinant of health following disaster. In that study, income inequality within community health districts increased the likelihood of depression among New York City adults surveyed by phone after the September 11 terrorist attack, but only among low-income adults, and neither individual income nor community income inequality predicted depression in the full sample. 68
Our findings suggest that material loss operates most powerfully through property damage: it was the only DHOS material loss that differentiated health independent of individual sociodemographics capturing well-established social determinants of health. Research has similarly identified housing-related property losses and instability following the foreclosure and economic crises of the Great Recession as a leading mechanism that this economic disaster shaped social stratification of health. 69 Research on housing and health also points out that property losses have the potential to reflect material gains accumulated over years or even generations, since home ownership is the most common form of wealth in the United States. 70 Additionally, because our property loss question asked about both damages experienced by respondents as well as their family, its unique salience may be that it captured material losses in the individuals' social network.
Additionally, our finding that the social stratification of health (measured by individual property loss) is widened by spatial stratification of health (measured by relative income concentration at the extremes) lends support to the hypothesis that disaster does not simply reflect existing systems of social and spatial stratification, but it exacerbates them. It also lends support to the proposition that, in an “age of extremes,” the ICE better captures the importance of spatial stratification than other more conventional segregation measures. 71 Our findings do not support a direct psychosocial pathway between spatial inequality and health, 72 and we speculate that the interaction may capture the greater economic precarity of individuals residing in areas with concentrated disadvantage (e.g., due to a lack of potentially compensating material resources within their social networks).
Research on population growth and migration has made such an argument for the entirety of the United States, in which interactions between racial and socioeconomic composition are seen to provide evidence of feedback cycles of spatially and socially stratified disaster resilience, that is, segmented resilience. 73 , 74 So too has research on wealth, in which adult social position (e.g., race and education) differentiates both associations of county-level assessment of damage due to natural hazards and of federal disaster disbursements. 75 Life course social determinants of health research provide empirical evidence for feedback cycles between health, social, and economic attainments across individual's lives and generations. 76 And multilevel social determinants of health research, particularly on residential segregation, describe macro-to-micro as well as micro-to-macro pathways for these cycles. 77 Our findings lend support to such macro-to-micro pathways considered in the broader social determinants of health literature, but underdeveloped respective to disaster.
The limitations of our findings suggest directions for future work. First, although we used retrospective accounts of residential history since the DHOS and material losses attributable to the disaster to measure community conditions and the disaster-related material loss before self-rated health, the cross-sectional nature of the data means that time sequencing is unclear. Moreover, it was beyond the scope of this study to obtain more geographically granular than county-level residential histories and five-digit zip codes for current residence. Additionally, by selecting measures of segregation's two dimensions most commonly associated with health (e.g., especially, dissimilarity for concentration–evenness), our measures were not sensitive to the patterns of spatial clustering within and between zip codes. 78 The later form of measurement bias could explain our null findings respective to racial segregation.
Future studies should examine more detailed residential histories, measures of racial segregation explicitly designed to capture spatial patterning of residential clustering, and alternative units other than zip code or county for summarizing and contrasting these patterns. More detailed measures of financial and job loss, as well as economic and property damage, that capture the magnitude of loss could also provide further insights about how disaster loss affects health outcomes. Moreover, like others who have reframed the “reverse-causality” debate as an opportunity for understanding accumulative feedback cycles, 79 we suggest that our findings motivate further exploration of the potential role environmental disaster plays in macro–micro population dynamics of social and spatial stratification, vis-à-vis health. As posited more broadly respective to human development, 80 the feedback between social stratification, disaster, and health our study begins to unravel may include historical feedback over time as healthier, more resilient individuals move between communities, as well as developmental feedback between health and material circumstances over the life course and even intergenerationally.
Footnotes
Author Disclosure Statement
The authors have no conflicts of interest or financial ties to disclosure.
Funding Information
This research was made possible by a grant from The Gulf of Mexico Research Initiative (231501-00). Data are publicly available through the Gulf of Mexico Research Initiative Information & Data Cooperative (GRIIDC) at
Appendix Table A1
Odds Ratios of Poor/Fair Health Associated with Zip Code Sociodemographic Composition, ZCTA Income Segregation, County Income Segregation, Individual Sociodemographics, and Damage Due to Deepwater Horizon Oil Spill
| Model A1 | Model A2 | Model A3 | Model A4 | Model A5 | ||
|---|---|---|---|---|---|---|
| Material loss | ||||||
| Property damage (Ref: No) | ||||||
| Yes | 2.35 a (1.00–5.52) | 2.36 a (1.01–5.51) | 2.23 b (0.92–5.39) | 2.31 b (0.97–5.49) | 2.32 b (0.98–5.45) | |
| Damage × household income | ||||||
| Yes × ($20,000–$39,999) | ||||||
| Yes × ($40,000–$74,999) | ||||||
| Yes × (≥$75,000) | ||||||
| Zip code income segregation | ||||||
| ICE | 0.08 a (0.01–0.66) | 0.12 c (0.02–0.58) | 0.12 c (0.02–0.60) | 0.13 b (0.01–1.07) | 0.10 a (0.01–0.73) | |
| Material loss × zip code income segregation | ||||||
| Yes × (ICE) | ||||||
| Zip code sociodemographic composition | ||||||
| % Non-Hispanic Black | 0.99 (0.98–1.01) | |||||
| % Hispanic | 1.02 (0.98–1.05) | |||||
| Median household income (logged) | 0.96 (0.85–1.08) | |||||
| % Households with no vehicle | 1.00 (0.95–1.06) | |||||
| % Unemployed (pop. age ≥16 years) | 0.98 (0.86–1.12) | |||||
| Model A6 | Model A7 | Model A8 | Model A9 | Model A10 | Model A11 | |
| Material loss | ||||||
| Economic or property loss (Ref: No) | ||||||
| Yes | 2.28 b (1.00–5.21) | 2.35 b (0.99–5.58) | 2.47 a (1.08–5.66) | 2.33 b (0.96–5.65) | 2.40 a (1.02–5.64) | 1.02 (0.14–7.59) |
| Material loss × household income | ||||||
| (Yes damage) × ($20,000–$39,999) | 1.95 (0.13–29.26) | |||||
| (Yes damage) × ($40,000–$74,999) | 4.34 (0.53–35.32) | |||||
| (Yes damage) × (≥$75,000) | 1.15 (0.11–12.59) | |||||
| Zip code income segregation | ||||||
| ICE | 0.17 a (0.03–0.83) | 0.08 a (0.01–0.66) | 0.11 c (0.02–0.59) | 0.11 c (0.02–0.55) | 0.11 c (0.02–0.56) | 0.17 a (0.03–0.85) |
| Material loss × zip code income segregation | ||||||
| (Yes damage) × (ICE) | 0.004 a (0.00–0.71) | |||||
| Zip code sociodemographic composition | ||||||
| % Employed in agriculture, forestry, fishing hunting, mining (pop. age ≥16 years) | 1.06 (0.98–1.14) | |||||
| Median housing value | 1.00 (1.00–1.00) | |||||
| % Vacant housing | 0.99 (0.97–1.01) | |||||
| % Rural | 0.99 (0.98–1.01) | |||||
| County income segregation | ||||||
| Income inequality (Gini) | 0.04 b (0.00–1.74) | |||||
| Total observations | 1281 | 1281 | 1281 | 1281 | 1281 | 1281 |
Data are from the Survey of Trauma, Resilience, and Opportunity among Neighborhoods in the Gulf 2016. Logistic regression models include covariates not shown to control for respondent's race/ethnicity, gender, age, marital status, education, income, employment. Models adjust for sampling weights and clustering of respondents within zip codes. Parentheses contain 95% confidence intervals.
p < 0.05.
p < 0.10.
p < 0.01.
ICE, income concentration.