
Abstract
Background:
Black communities, comprising 32.2% of Louisiana’s population, were disproportionately affected by the COVID-19 pandemic. Significant social disparities and a high prevalence of chronic health conditions within this demographic have heightened their vulnerability to the virus. Long-term exposure to air pollutants, along with preexisting immune and respiratory conditions, has been associated with increased susceptibility to COVID-19. This study seeks to evaluate the relationship between fine particulate matter (PM2.5) exposure and COVID-19 incidence and mortality rates in Louisiana, USA.
Methods:
Descriptive and multivariate regression analyses were conducted to examine the associations between PM2.5 levels and county-level COVID-19 incidence and mortality (both count and rate) in Louisiana. ArcGIS spatial analysis was utilized to perform zonal statistics, enabling a geographic assessment of the relationships between air pollution and COVID-19 outcomes.
Results:
Louisiana’s 19-year average PM2.5 concentration (9.1 µg/m³) exceeds the U.S. average (8.4 µg/m³). Prolonged exposure to PM2.5 has been linked to heightened COVID-19 risks. Specifically, a 1 µg/m³ increase in PM2.5 corresponded to approximately 15% higher COVID-19 incidence and a 22%–35% rise in mortality rates among Black populations, after adjusting for underlying health conditions and risk factors (p < 0.05). Black communities faced approximately 20% greater COVID-19 risks compared with the total population. For exposure durations of 6–14 years, the COVID-19 risk increased by 6.5%–16.4% among Blacks and by 2.8%–10.5% overall. Preexisting health conditions, particularly those affecting diabetic kidney function, were more strongly associated with COVID-19 risks than respiratory diseases across all PM2.5 exposure durations.
Conclusions:
The disproportionate impacts of COVID-19 on Black communities highlight the urgent need to address air pollution and health disparities to reduce COVID-19 risks in Louisiana. Our findings underscore the importance of controlling PM2.5 levels and implementing effective public health responses to prevent COVID-19 and other future respiratory diseases at both local and state levels.
INTRODUCTION
Nearly 99% of the global population is exposed to ambient air pollution levels that are linked to numerous adverse health effects, even at concentrations lower than previously acknowledged. This underscores the substantial impact of air pollution on public health. 1 Recently, both the World Health Organization and the U.S. Environmental Protection Agency (EPA) revised their annual particulate matter (PM2.5) standard levels to 5 and 9 µg/m³, respectively.1,2 PM2.5 can be emitted directly from sources as primary particles or formed in the atmosphere as secondary particles through chemical interactions with gases such as sulfur dioxide, nitrogen oxides, ammonia, and other organic compounds. 3 PM2.5 particles are capable of remaining airborne for extended periods and can travel hundreds of miles from their point of origin. 4
Louisiana’s PM2.5 emission data, as reported by Terrell and James (2020) and derived from the National Emissions Inventory, indicate a 20% reduction in overall emissions between 2014 and 2017.4,5,6 However, industrial PM2.5 emissions increased by 33% during the same period. 7 Between 2000 and 2018, the average concentration of PM2.5 in Louisiana was 9.1 µg/m3 (range: 7.6–17.6 µg/m3), 8 which surpasses the national average level of 8.5 µg/m3 in the United States. 9 In a 2020 national study examining county-level air pollution and COVID-19 mortality rates in the United States, a 1 µg/m³ increase in PM2.5 was strongly associated with an 8% increase in the COVID-19 mortality rate.10,11
PM2.5 particles can penetrate deep into the lungs and enter the bloodstream, contributing to a range of adverse health outcomes. 12 These include respiratory, cardiovascular, and neurological conditions, as well as diabetes, obesity, kidney disease, chronic obstructive pulmonary disease (COPD), and reproductive disorders.13,14,15,16,17 Long-term exposure to PM2.5 has also been linked to premature deaths among individuals with chronic heart or lung diseases. 18 Furthermore, a study demonstrated that a 10 µg/m3 increase in PM2.5 concentration was significantly associated with a 1% increase in mortality rates from both cardiovascular 19 and respiratory diseases. 20 Additional health effects of PM2.5 exposure include compromised immune system function,21,22,23 inflammation in lung cells,24,25 unbalancing angiotensin-converting enzyme 2,26,27,28 and increased susceptibility to severe COVID-19 symptoms and death.14,29
Several studies have reported that a 1 µg/m3 increase in PM2.5 exposure is associated with an 8%–18% increase in COVID-19 mortality.11,30 Furthermore, studies have documented that the majority of hospitalized patients with COVID-19 had multiple underlying health conditions.22,31,32 The presence of these preexisting conditions has also been linked to the severity of COVID-19 outcomes.31 Studies have demonstrated associations between PM2.5 exposure and chronic health conditions such as hypertension, diabetes, cardiovascular disease, kidney disease, and obesity. These conditions are commonly associated with COVID-19 mortality, particularly among Black population.33,34,35,36,37,38 In Louisiana, increased industrialization and traffic are the major sources of PM2.5, leading to elevated exposure levels and heightened vulnerability to respiratory illnesses, particularly among the Black population. 39 Between 2014 and 2017, industrial PM2.5 emissions increased by 33% due to ongoing industrial expansion, hence accounting for 25% of total PM2.5 emissions in 2017.4,5,6,7 Approximately 55% of the Louisiana’s parishes have exceeded the EPA PM2.5 safety level of 9 µg/m3.3,9 Previous studies in Louisiana revealed associations between elevated PM2.5 levels and a higher percentage of Black residents, increased social disparities, and older age demographics.8,40 Higher rates of underlying health conditions were also linked to living near industrial areas, further increasing vulnerability to respiratory illnesses, particularly among Black populations.40,41 Additionally, exposure to elevated PM2.5 levels has been associated with a higher prevalence of hypertension, diabetes, and obesity in adolescents,37,42,43,44 conditions that are among Louisiana’s leading causes of death. 45
The Black population bears significant social and health disparities including higher percentages of underlying health conditions, poor living conditions, generational poverty, and other disparity factors, and hence they are the most vulnerable to COVID-19. 46 These vulnerabilities have contributed to disproportionately higher rates of COVID-19 cases (32%) and deaths (38%) among this demographic. 47 Among the 10 parishes (counties) with the highest COVID-19 cases and deaths, over 80% have a Black population exceeding 40%. 48 These parishes, which include East Baton Rouge, Orleans, and Jefferson, are among the most populous (100,000–500,000 residents per parish) and are situated in the industrialized corridor, exposing them to elevated PM2.5 levels.41
Previous studies have reported higher COVID-19 mortality rates among Black populations,39,40,48 but in Louisiana, research on the connection between chronic PM2.5 exposure and COVID-19 infection and mortality among Black communities remains limited. The objective of this study is to map the spatial distribution of PM2.5 exposure and COVID-19 incidence and mortality in Louisiana and assess their associations, adjusting for underlying health conditions and social factors within Black communities. We hypothesized that communities exposed to higher PM2.5 concentrations and for longer durations would exhibit higher COVID-19 incidence, mortality (counts and rates), and related chronic health conditions. This study focuses on the 1-year period from March 1, 2020, to March 1, 2021, which aligns with the prevaccination phase for individuals aged 18 years and older in all 64 parishes. The study period was deliberately selected to avoid bias related to vaccination efficacy, as vaccines for this age group became widely available in Louisiana on March 29, 2021. 49
MATERIALS AND METHODS
Study population
We conducted a parish-level ecological study on Louisiana residents aged 18 and older. The population of Louisiana is 4.6 million with 2.75 million Whites (59.3%), 1.49 million Blacks (32.2%), 213,000 Hispanic (4.6%), 78,700 Asian (1.7%), 72,600 non-Hispanic mixed race (1.6%), and 32,900 others (0.71%).48
Data collection
COVID-19 data
Parish-level daily reported COVID-19 testing results, number of cases, and deaths stratified by race/ethnicity, age, and sex were reported to and collected by the Louisiana Department of Health and publicly released weekly were used. 50 COVID-19 data were obtained cumulatively weekly between March 1, 2020, and March 1, 2021, from the Louisiana Department of Health COVID-19 tracker website. A total of about 408,000 cases and 9600 deaths were reported during this timeframe.50
PM2.5 data
Ground level PM2.5 data over 19 years (2000–2018) were downloaded from publicly available database (https://github.com/wxwx1993/PM_COVID) produced by van Donkelaar et al.8 and organized and made available by Wu et al.10 This county-level data derived from satellite PM2.5 masses (total and compositional mass concentrations combining Aerosol Optical Depth) retrieved from the NASA MODIS, MISR, and SeaWIS instruments with the GEOS-Chem chemical transport model and calibrated to ground-based total and compositional masses using Geographically Weighed Regression.8,10 The PM2.5 exposure levels were estimated annually across Louisiana. We generated parish-level PM2.5 levels to assess the temporally averaged PM2.5 over 6 years (2013–2018), 11 years (2008–2018), and 19 years (2000–2018) within each parish using ArcGIS (Zonal Statistic Analysis). We mapped each dataset by percentile using ArcGIS Pro to visualize the geographic patterns of PM2.5 levels in different time periods.
Health and social disparities
Parish-level health, behavior, and social factors were collected from multiple database sources. These are: (1) Health and behavior factors: Underlying health conditions: prevalence of hypertension, diabetes, cardiovascular, kidney, obesity, COPD,asthma, and smoking status. 51 (2) Demographic and socioeconomic factors such as age, race, ethnicity, income, household size, uninsured people, and persons living in poverty,48 including a social vulnerability index (SVI), which refers to the negative effects on communities health caused by external stressors such as disease outbreaks on human health ranked from 0 (low SVI) to 1 (high SVI). 52
DATA ANALYSIS
For statistical analyses, we categorized race as Black, White, and other races/ethnicities (Asian, Hispanic, Hawaiian, and others) and age as adults (18–64 years) and elderly adults (65 years and older) across 64 parishes. The parish-level Black population density (%) was calculated using percentage of Black population per total population of each parish. Univariate statistics (minimum, 25th, 50th, 75th, maximum, and mean ± standard deviation) were used to describe reported COVID-19 cases, deaths, incidence rates, mortality rates, and PM2.5 levels. COVID-19 incidence and mortality rates were calculated as number of cases and deaths per 10,000 population per parish in total and stratified by race. PM2.5 average levels were reported over three exposure periods—19 years (2000–2018), 11 years (2008–2018), and 6 years (2013–2018) (Table 1). Negative binomial distribution and log link function were used to estimate unadjusted and adjusted risk between chronic PM2.5 exposures and COVID-19 mortality and incidence rates in the Black population compared with total and White populations adjusting for underlying health conditions and social factors status (Table 2), multivariable generalized linear models, Poisson distribution and log link function were used to estimate risk of COVID-19 case and mortality (Table 3). We were interested in two underlying health condition functions: (1) respiratory disease and (2) diabetic kidney disease. Respiratory disease factors include COPD, asthma, obesity, cardiovascular disease, hypertension, smoking, and socioeconomic factors. Diabetic kidney disease factors include diabetes, acute or chronic kidney disease, hypertension, and socioeconomic factors. Socioeconomic factors include household size, percent of uninsured population, percent of people under poverty, population aged 65 and older, population 18–64 years, and population density. Metropolitan parishes variable was added for all COVID-19 cases and deaths models to quantify the risk of PM2.5 exposure in populated parishes. Metropolitan parishes variable was categorized as metropolitan and nonmetropolitan parishes according to the U.S. Office of Management and Budget 2020 reported by U.S. Census Bureau. 53 The multicollinearity analysis was conducted to avoid variable redundancy, setting a variance inflation factor (VIF) cutoff at 2.5. Variables with VIF below 2.5 were selected to form multivariable regression models.
Characteristics of Parish Level of Average Particulate Matter Concentrations, COVID-19 Cases, Deaths, Mortality Rate, and Incidence Rate per 10,000 Population by Race in Louisiana Between March 1, 2020–2021
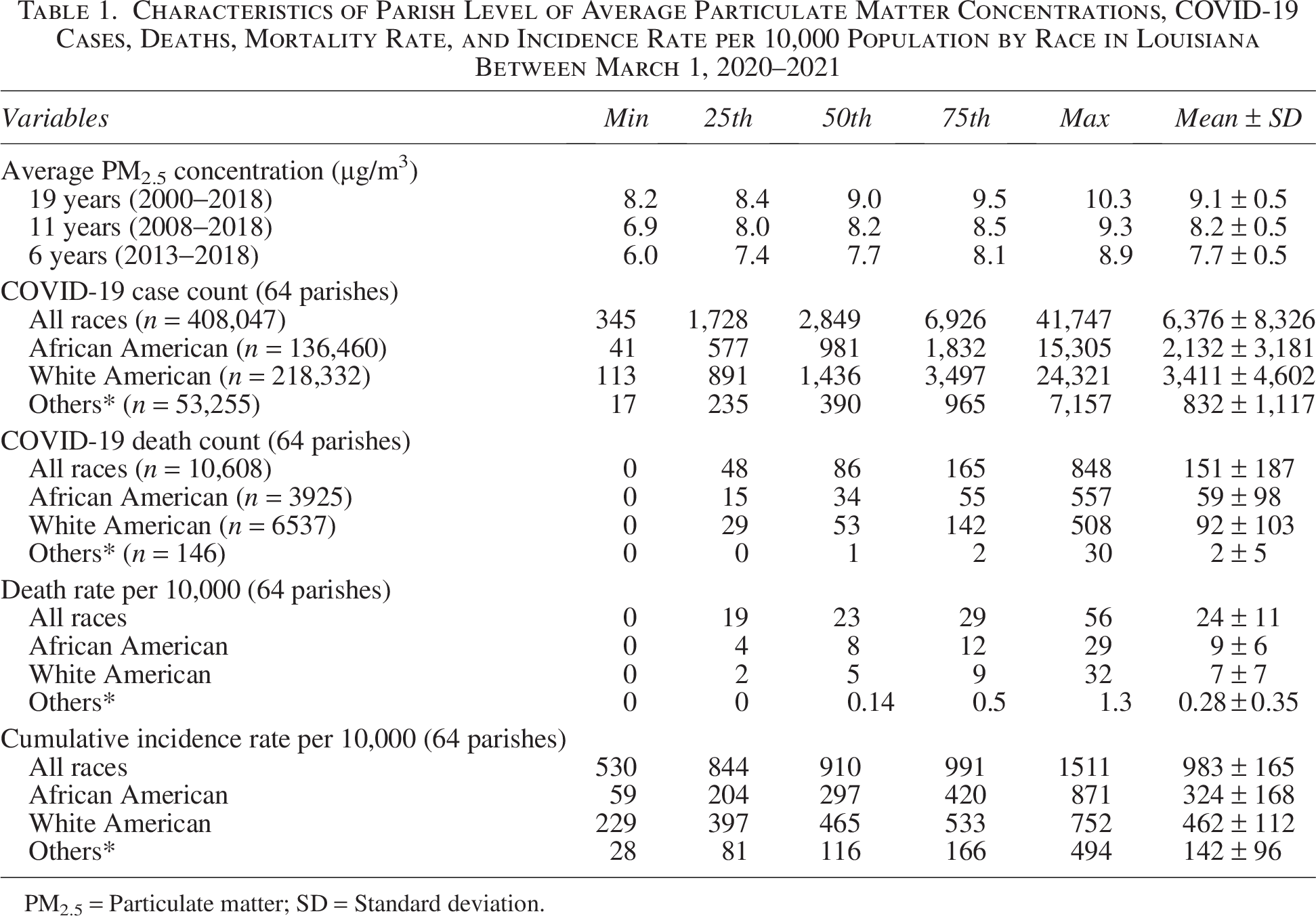
PM2.5 = Particulate matter; SD = Standard deviation.
Comparison of Particulate Matter Coefficient in Crude and Adjusted Models of Total Mortality Rate, Total Incidence Rate, Black Mortality Rate, Black Incidence Rate, White Mortality Rate, and White Incidence Rate Within 19, 11, and 6 Years of Particulate Matter Exposure Periods in Louisiana Between March 1, 2020, and March 1, 2021

Respiratoty disease factors: adjusting for chronic obstructive pulmonary disease (COPD), asthma, obesity, cardiovascular disease, hypertension, smoking, household size, % of uninsured population, % of poverty, population aged 65 and older, population 18–64 years, and population density.
Diabetic kidney disease factors: adjusting for diabetes, kidney disease, obesity, hypertension, smoking, household size, % of uninsured population, % of poverty, population aged 65 and older, population 18–64 years, and population density.
Full adjustment: adjusting for COPD, asthma, obesity, cardiovascular disease, hypertension, diabetes, kidney disease, smoking, household size, % of uninsured population, % of poverty, population aged 65 and older, population 18–64 years, and population density.
*0.01 < p < 0.05; **0.001 < p < 0.01.
Comparison of Particulate Matter Coefficient in Crude and Adjusted Models of Total Death Count, Total Case Count, Black Death Count, Black Case Count, White Death Count, and White Case Count Within 19, 11, and 6 Years of PM2.5 Exposure Periods in Louisiana Between March 1, 2020 and March 1, 2021
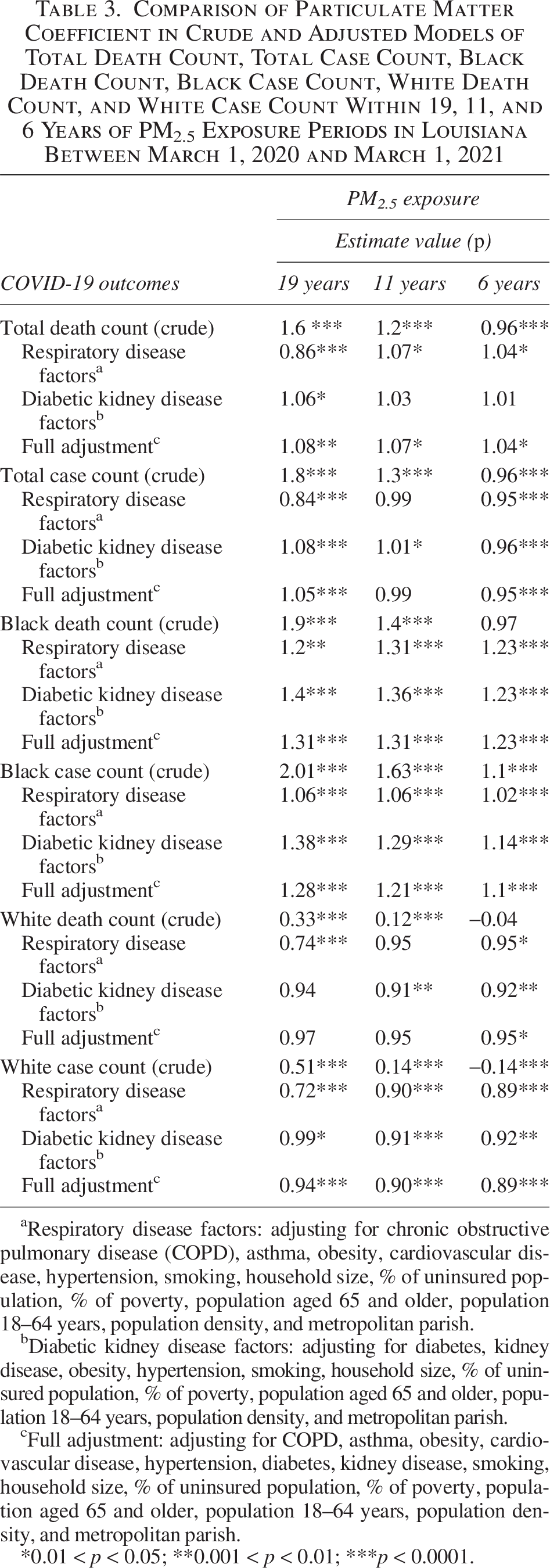
Respiratory disease factors: adjusting for chronic obstructive pulmonary disease (COPD), asthma, obesity, cardiovascular disease, hypertension, smoking, household size, % of uninsured population, % of poverty, population aged 65 and older, population 18–64 years, population density, and metropolitan parish.
Diabetic kidney disease factors: adjusting for diabetes, kidney disease, obesity, hypertension, smoking, household size, % of uninsured population, % of poverty, population aged 65 and older, population 18–64 years, population density, and metropolitan parish.
Full adjustment: adjusting for COPD, asthma, obesity, cardiovascular disease, hypertension, diabetes, kidney disease, smoking, household size, % of uninsured population, % of poverty, population aged 65 and older, population 18–64 years, population density, and metropolitan parish.
0.01 < p < 0.05; **0.001 < p < 0.01; ***p < 0.0001.
The multivariable regression models were used to assess the roles of underlying health conditions on the relationship between COVID-19 and PM2.5. Multivariable linear regression models were built using four primary models: Crude model (Eq. 1), adjusted for respiratory disease function and socioeconomic factors (Eq. 2), adjusted for diabetic kidney disease function and socioeconomic factors (Eq. 3), and full adjustment (Eq. 4).




Three average PM2.5 exposures were used in each model representing exposure over 6, 11, and 19 years. Four different outcomes were used for each model: COVID-19 case count, death count, cumulative incidence rate, and mortality rate. A total of 48 predictive models were established to represent 48 different exposure-outcome scenarios with model residuals normally distributed.
The analysis results were reported and interpreted as (1) the relative increase in the COVID-19 incidence and mortality rates associated with a 1 µg/m3 increase in each PM2.5 exposure period (Table 2) and (2) the relative increase in the COVID-19 counts (cases and deaths) associated with a 1 µg/m3 increase in each PM2.5 exposure period (Table 3). We evaluated sensitivity by repeating all the analyses excluding parishes that had zero COVID-19 deaths to estimate exposure to PM2.5 as well as modifying the adjustment for confounders such as log transformation or categorization of the covariates. All analyses were carried out using SAS statistical software (Cary, NC). Parish-level spatial analysis was conducted using ArcGIS software to create descriptive maps that illustrate the distributions of COVID-19 counts and rates and PM2.5 levels in different exposure periods.
RESULTS
PM2.5 distribution in Louisiana
The spatial distribution of PM2.5 levels within a 10-mile buffer zone surrounding active gas and oil wells, solid disposal sites, roads, and urbanized parishes is illustrated in Figure 1. Parishes within these regions, characterized by higher PM2.5 levels, are predominantly situated in heavily industrialized areas with dense traffic and extensive urban activities.
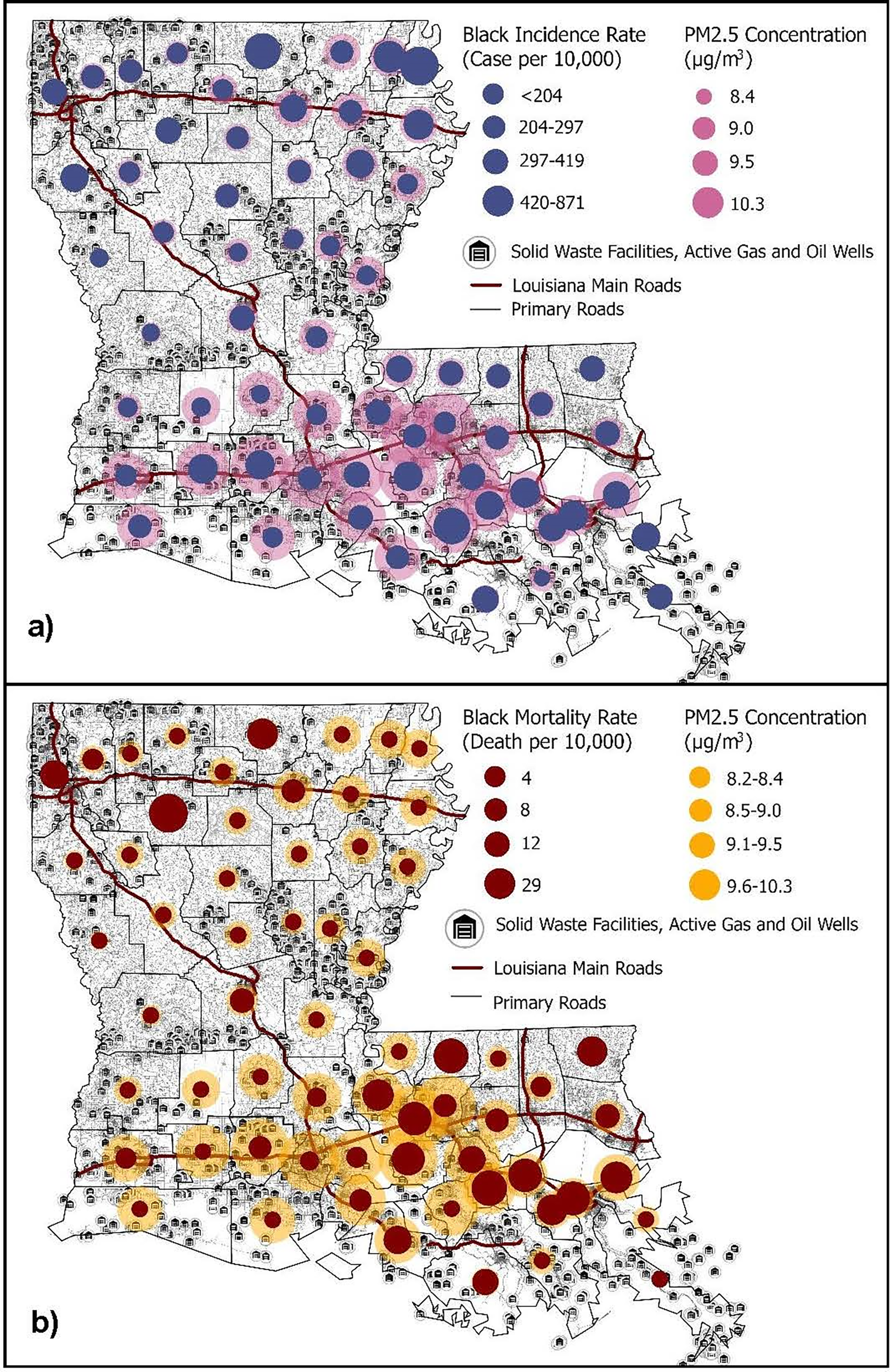
Overlayed hotspots of COVID-19.
COVID-19 incidence and mortality—measured in both counts and rates—were observed to rise with prolonged PM2.5 exposure, especially in parishes with a high proportion of Black residents. These areas, often situated along Louisiana’s industrial corridor, underscore the compounded effects of air pollution and socioeconomic disparities on public health outcomes.
COVID-19 cases and deaths in Louisiana
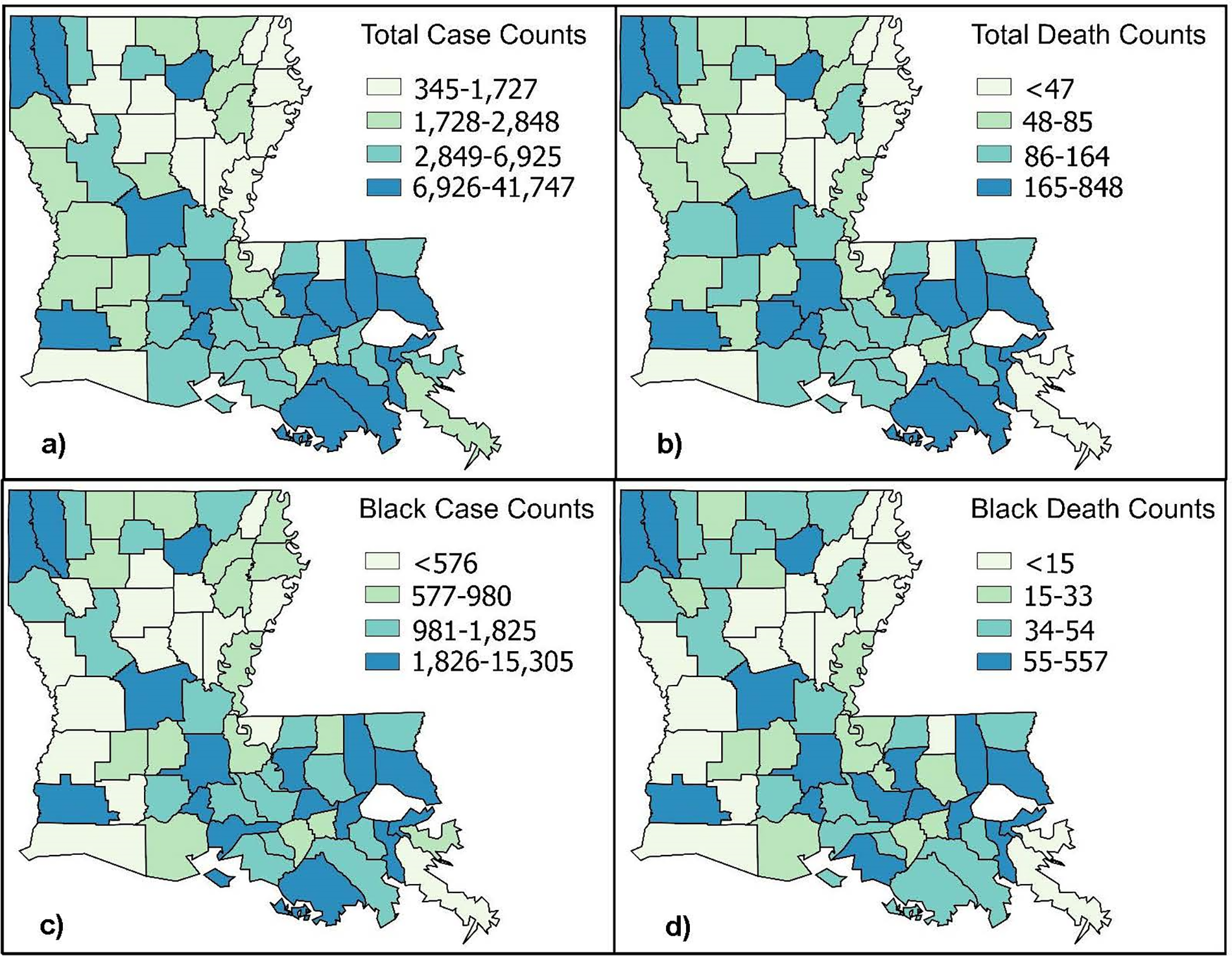
Among the 64 parishes evaluated, four reported zero COVID-19 deaths and three reported fewer than 100 COVID-19 cases. Across Louisiana, a total of 10,608 COVID-19 deaths were recorded, comprising 3925 Black individuals, 6537 White individuals, and 146 individuals of other races. Additionally, 408,047 COVID-19 cases were reported statewide, including 136,460 Black individuals, 218,332 White individuals, 53,255 individuals of other races, and 22,150 individuals of unknown racial origin.
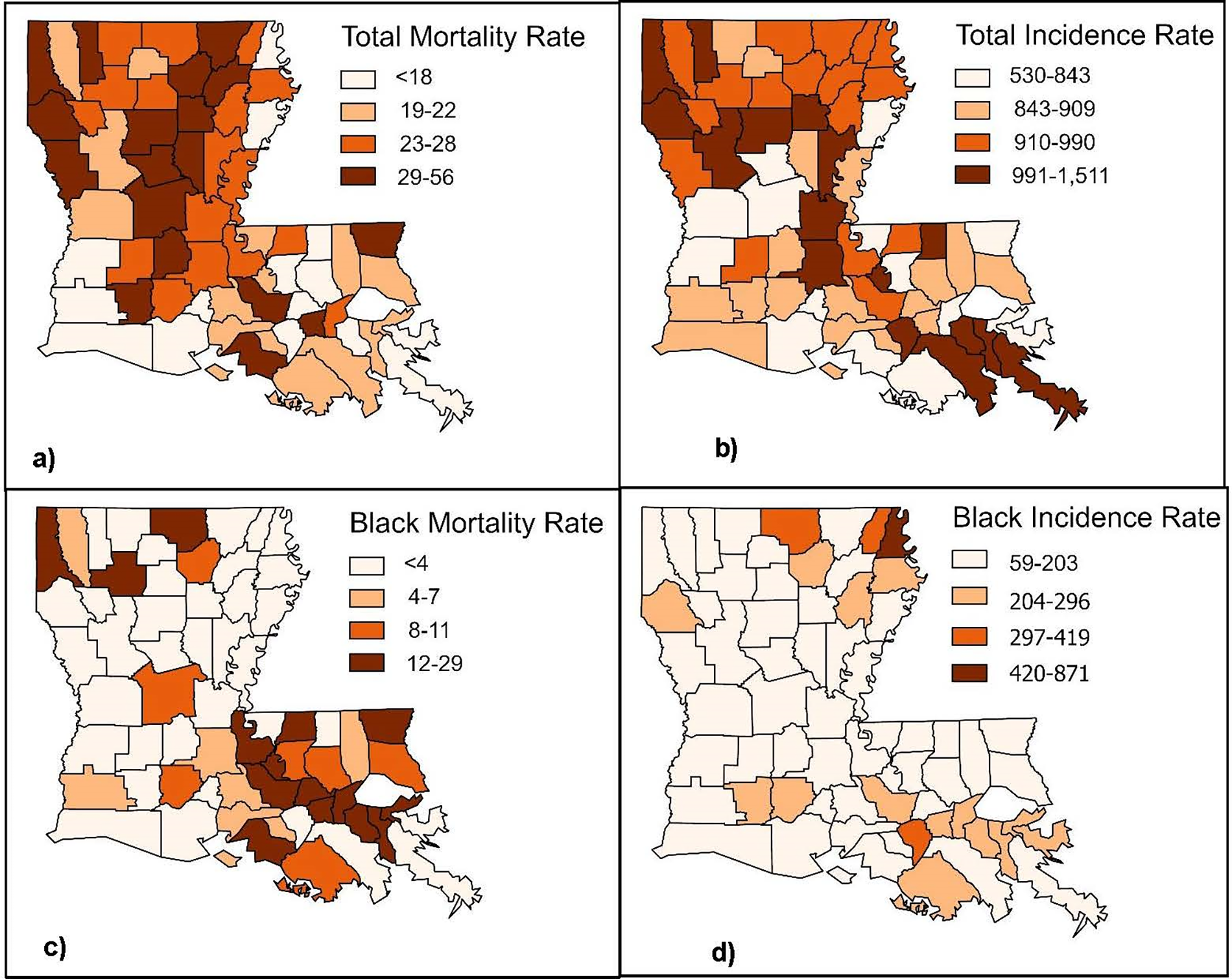
The average Black mortality rate per 10,000 persons (nine deaths) was 1.3 times higher than that of Whites (seven deaths per 10,000) and 32 times higher than other races (0.28 deaths per 10,000) (Table 1). In northern Louisiana, similar spatial patterns were observed between total and Black COVID-19 incidence and mortality counts and rates, particularly in parishes within the upper 25th percentile for these variables (Figs. 2 and 3). In the southern region of Louisiana, higher Black mortality rates (>13 deaths per 10,000 population) were concentrated in five parishes: West Baton Rouge, Iberville, St. John the Baptist, and Orleans (Fig. 3c).
Percentile of spatial distribution of
Percentile of spatial distribution of COVID-19 rate per 10,000 population:
Long-term PM2.5 level exposures
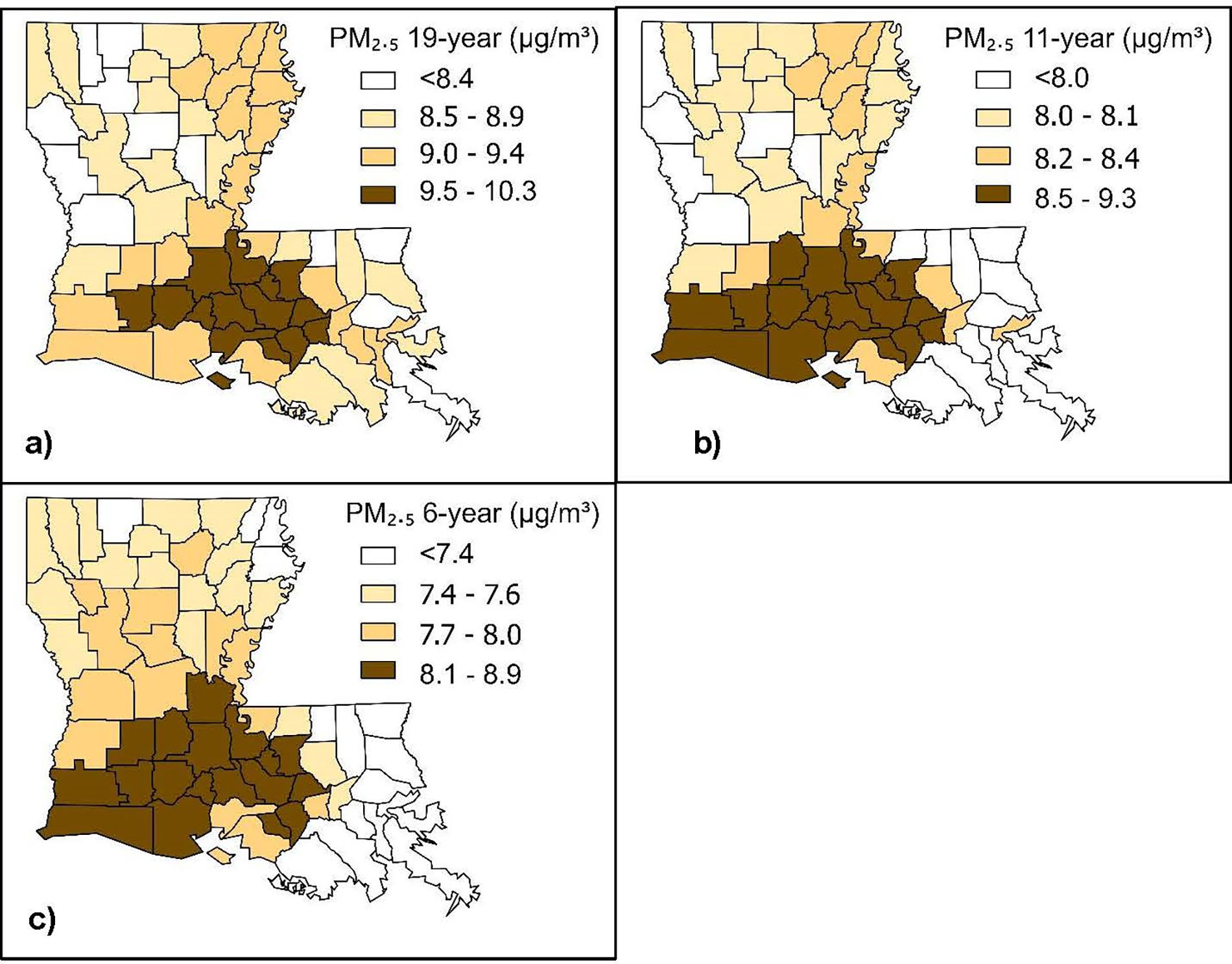
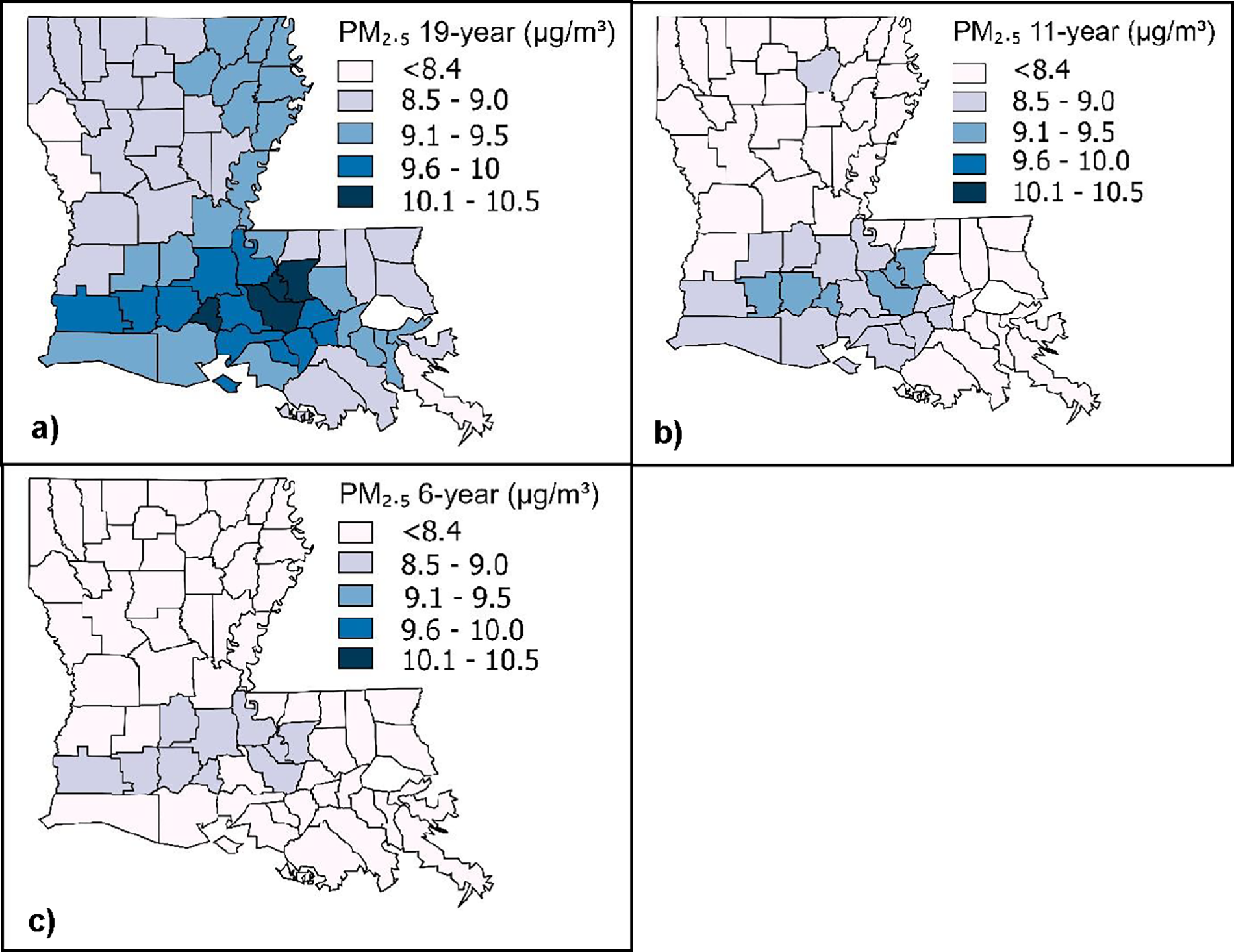
The average PM2.5 concentrations in Louisiana have trended downward since 2000: 2000–2018 (9.1 ± 0.5 µg/m3); 2008–2018 (8.2 ± 0.5 µg/m3); and 2013–2018 (7.7 ± 0.5 µg/m3) (Table 1, Fig. 4). The highest PM2.5 levels areas were observed in southern Louisiana where most parishes are industrialized and urbanized (Fig. 1). Jefferson and St. Charles parish PM2.5 levels—parishes inclusive of or next to New Orleans—have decreased to below the EPA safety level (<8 µg/m3) (Fig. 4b). The parish-level average PM2.5 over 6-year levels have mostly decreased to <8 µg/m3; however, 16 parishes remain in the higher percentile range including Mississippi Industrial Corridor parishes: Baton Rouge, Iberville, and Ascension (Fig. 4c). Twenty-three parishes had average 19-year PM2.5 levels higher than the EPA safety level (Fig. 5a), while six parishes PM2.5 levels remain higher than EPA’s safety level over 11 years; however, all below in 6-year period (Fig. 5b, c).
Quartile of average PM2.5 levels (µg/m3).
Time series of PM2.5 levels (µg/m3) change from
Association between PM2.5 exposure and COVID-19
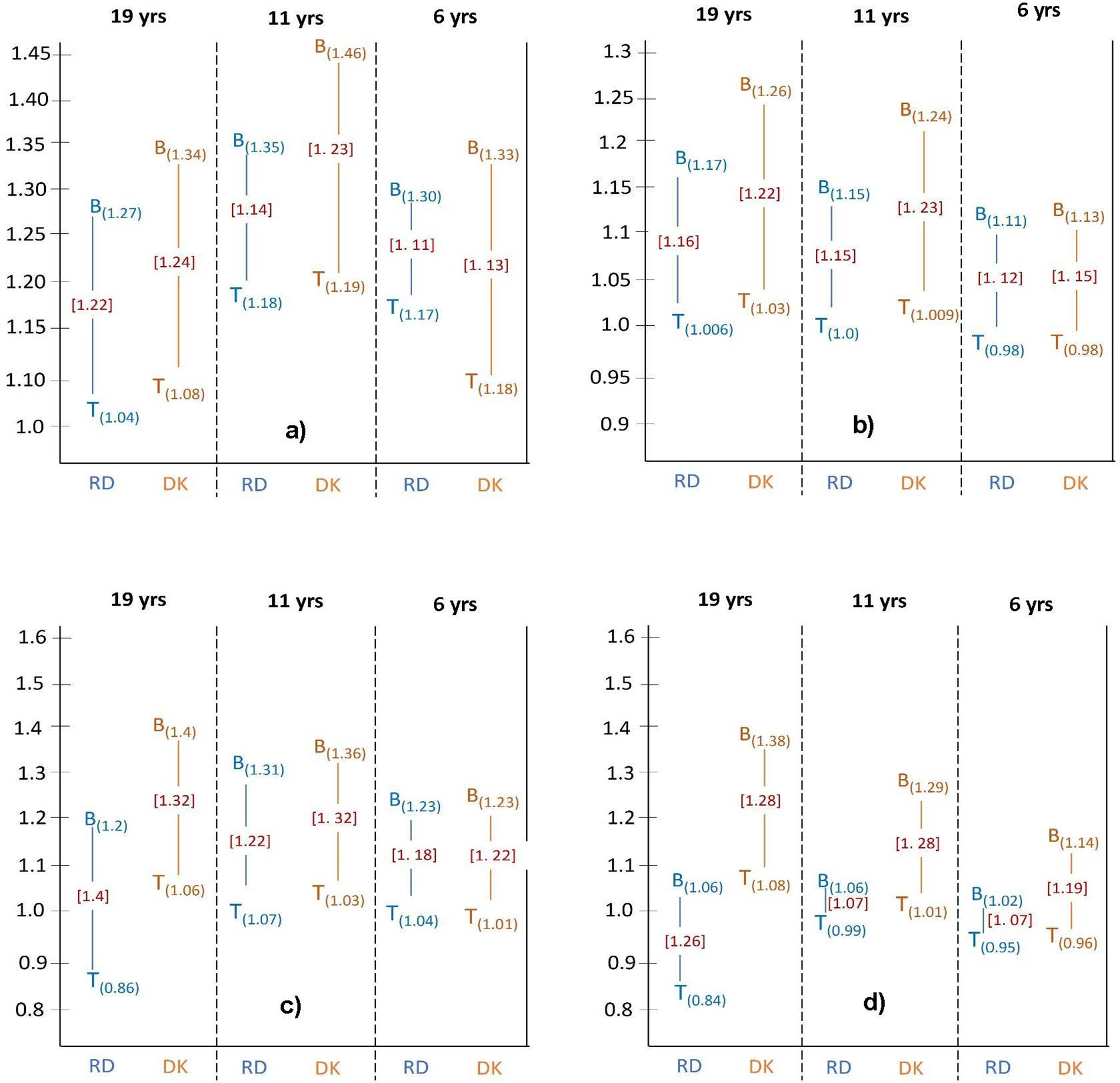
COVID-19 mortality and incidence rates and COVID-19-related death risk in Blacks were ∼11%–40% higher than that of the total population across all PM2.5 exposure periods. Furthermore, COVID-19 mortality rates in Blacks with diabetic kidney disease characteristics were higher than in Blacks with respiratory disease characteristics; however, Blacks consistently had higher rates than other race/ethnicities (Table 2, Fig. 6).
Risk of COVID-19 comparisons between Black population and overall population;
PM2.5 exposures and COVID-19 mortality rate
In fully adjusted models, PM2.5 levels over 6–11 years, a 1 µg/m3 increase in PM2.5 concentrations was significantly associated with 33%–39% increase in total mortality rate (p < 0.03) (Table 2). Blacks had an increased COVID-19 mortality rate across all exposure periods when adjusting for respiratory disease; however, a significant 30%–46% increase was observed with PM2.5 exposure over 5 years (p = 0.04) or over 5–10 years adjusting for kidney disease (p = 0.04) (Table 2, Fig. 6).
PM2.5 exposures and COVID-19 incidence rate
A 1 µg/m3 increase in PM2.5 over 19 years was associated with 0.6%–3% increase in COVID-19 incidence rate in all races (Table 2). In Blacks, a 15%–26% increase in COVID-19 incidence rates was associated with increased PM2.5 over 11 and 19 years when adjusted for respiratory and kidney disease, respectively (all p = 0.04).
PM2.5 exposures and COVID-19 death count
Adjusting for respiratory or kidney disease, a 1 µg/m3 increase in PM2.5 concentration was significantly associated with a 4%–8% increase in COVID-19 deaths among those metropolitan parishes when exposure occurred over 6–11 years (p = 0.04) and 19 years (p = 0.01), respectively (Table 3). COVID-19 death counts increased ∼8% COVID-19 with at least 11 years of PM2.5 exposure. In Blacks, a 1 µg/m3 increase in PM2.5 concentrations was associated with 1.4–1.9 times higher death counts (p < 0.0001). Similar results were obtained in models adjusted for respiratory disease or kidney disease.
PM2.5 exposures and COVID-19 case count
Among those metropolitan parishes, a 1 µg/m3 increase in PM2.5 concentrations was associated with 30%–80% increase in COVID-19 cases in all races (p < 0.0001). In Blacks when adjusted for kidney disease or respiratory disease, a 1 µg/m3 increase in PM2.5 concentrations was associated with a 14%–38% (p < 0.0001) and a 2%–6% (p < 0.0001) increase in COVID-19 cases. The largest increase (38%) in cases was observed in models with 19 years of PM2.5 exposures and adjusted for kidney disease (p < 0.0001) (Table 3). In Whites, significant inverse associations were observed in all predictive models across all exposure periods (p = 0.03).
Discussion
Air pollution is a significant factor contributing to health disparities in the United States. In Louisiana, industrial activity and fuel combustion are the primary sources of total PM2.5 emissions.5 The accumulation of SARS-CoV-2 viral loads is exacerbated in poorly ventilated indoor environments, particularly in communities located near emission sources. This results in increased virus-PM2.5 accumulation indoors, heightening the susceptibility of individuals in these settings to respiratory illnesses and COVID-19 infection.54,55,56 Chronic exposure to PM2.5 pollution can lead to progressive and prolonged inflammation of the respiratory pathways, increasing the risk of acute respiratory and viral infections.25,26 These effects underscore the need to address air pollution as a critical public health concern, particularly in vulnerable populations disproportionately affected by environmental and social inequities.
Higher COVID-19 cases and mortalities were observed with prolonged PM2.5, exposure, particularly in parishes with a high proportion of Black residents, many of which are located along Louisiana’s industrial corridor. Parishes with COVID-19 mortality, incidence, Black mortality, and Black incidence rates in the upper half of the distribution include Morehouse, East Carroll, Madison, Tensas, Concordia, and Evangeline. These parishes also exhibited long-term PM2.5 levels exceeding annual averages and tended to have a higher prevalence of underlying health conditions. Parishes located in regions with elevated PM2.5 levels (>75th percentile) include West Baton Rouge, East Baton Rouge, Lafayette, Iberville, Jefferson Davis, Calcasieu, and Acadia. These areas consistently recorded the highest average annual PM2.5 levels across the three exposure periods studied. Located in southern and eastern Louisiana, these parishes are characterized by a high density of oil and gas industries and congested roadways. COVID-19 cases and deaths were notably higher in these regions compared with other parishes, underscoring the compounded impact of industrial emissions, traffic congestion, and preexisting health vulnerabilities.
In our study, underlying health conditions emerged to act as effect modifiers in the association between PM2.5 exposures and COVID-19 outcomes. As supported by previous studies, underlying health conditions elevate the risk of COVID-19 infection and mortality across the general population; however, these risks were disproportionately higher among Black individuals, irrespective of PM2.5 exposure duration.40,47 The contribution of PM2.5 exposure to COVID-19 infection and mortality, when adjusted for diabetic kidney disease function, was greater than that for respiratory disease function. Notably, Black populations were more vulnerable to PM2.5 exposure across all exposure periods, regardless of underlying health conditions, compared with other racial groups.7,40 Our previous research in Louisiana identified significant correlations between COVID-19 mortality rates in Black populations and conditions such as diabetes, kidney disease, and hypertension, with these correlations being higher than those observed in White populations.46 Parishes with a higher proportion of Black residents (>40%) had COVID-19 incidence and mortality rates that were 1.5–1.7 times higher than those of other parishes when adjusted for underlying health conditions.46 Our results demonstrated robustness across a range of sensitivity analyses.
Many health disparities are believed to stem primarily from racially segregated neighborhoods.57,58 Segregation is driven by structural mechanisms of discrimination that perpetuate political, economic, legal, and social inequities. 59 The majority of PM2.5 exposure resulting from goods and service consumption disproportionately affected Black communities and other racial/ethnic minorities.41,60 In Louisiana, White populations experienced lower air pollution burdens compared with Black populations, partly due to lower poverty and unemployment rates among Whites.7,40 Cardiovascular disease and diabetes in Blacks are associated social and environmental inequities,61,62,63 which are exacerbated by poor nutrition caused by food desserts in Black communities.59 These diseases can be triggered or worsened by chronic exposure to PM2.5.41,61,64 Minority communities in many parts of the U.S. are disproportionally affected by poor social, and environmental conditions.64 At the onset of the COVID-19 pandemic in 2020, Louisiana had the second-highest poverty rate in the United States, with Black populations experiencing higher poverty levels than White and Hispanic populations. 65 Louisiana has a higher prevalence of underlying health conditions compared with the national average, with its overall health quality consistently ranked between 41st and 50th among the 50 states.66,67 Obesity, diabetes, and cardiovascular disease are major underlying health conditions associated with PM2.5 exposure and COVID-19 severity among Black populations. Louisiana ranks first, fifth, and sixth in the nation for these conditions, respectively.47,52 Furthermore, leading underlying health conditions (hypertension (59%), diabetes (37%), heart disease (21%), kidney disease (20%), and obesity (20%)) found in COVID-19 deaths and reported to the Louisiana Department of Health47 are health conditions that significantly associated with PM2.5 exposures and social disparities in our study. Louisiana’s high prevalence of these underlying conditions and high levels of PM2.5 likely contributed to its large number of COVID cases and deaths during the pandemic.
Spatial analysis of high COVID-19 mortality rates among Black populations revealed a pattern similar to the respiratory hazard index (RHI) observed in previous studies. Increased COVID-19 mortality rates were associated with higher RHI and immunological hazard index levels.7 It is crucial to conclude that a comprehensive strategy to prevent future epidemics akin to COVID-19 must extend beyond biological and medical realms. A proactive approach to mitigate future epidemics involves implementing environmental and socioeconomic considerations, and sustainable policy, particularly focusing on reducing air pollution levels, especially in Louisiana parishes with heavily polluted areas with high moisture levels, and frequent fog days.68 These conditions can create an environment conducive to rapid viral transmission dynamics and capable of initiating air pollution-driven transmission of viral infectivity.69 Although our study findings are robust and consistent with other published studies, it has limitations. Our data were observational, which limits the ability to draw causal inferences. We utilized parish-level COVID-19, health, and sociodemographic data, which may reduce accuracy and sensitivity. Nevertheless, given the similarities between our study population and those in other U.S. states, our findings are likely generalizable across the United States.
CONCLUSIONS
Our study has shown strong associations between PM2.5 exposure levels and duration with COVID-19 infection and mortality in Louisiana. Furthermore, our findings highlight the persistent racial disparities in exposures and health outcomes among Black populations, driven by systemic racism in the state. Parish-level data on COVID-19, PM2.5 exposures, and related racial disparities provide valuable insights for a data-driven public health response to similar disease outbreaks. These findings can assist governmental and scientific communities in planning effective public health interventions and establishing preventive measures, including allocating additional resources to mitigate the risk of poor outcomes from COVID-19 and other potential respiratory illness outbreaks. These findings can also raise awareness of the continued need to reduce environmental, health, and racial disparities. It advocates for stricter industrial emissions regulations to reduce PM2.5 levels in Louisiana and beyond, contributing to improved health equity and environmental justice.
AUTHORS’ CONTRIBUTIONS
P.K.T.: Methodology, software, validation, formal analysis, resources, data curation, writing—original draft, writing—review and editing, and visualization. T.R.G.: Conceptualization, validation, resources, writing—review and editing, supervision, project administration, and funding acquisition. D.B.B.: Validation and writing—review and editing.
Footnotes
AUTHOR DISCLOSURE STATEMENT
No competing financial interests exist.
FUNDING INFORMATION
We thank Tulane University's School of Public Health and Tropical Medicine's Dean COVID-19 Rapid Response grant that made this pilot COVID-19 and health disparity research possible.