
Abstract
Background:
The COVID-19 crisis unfolded foregrounded by unprecedented levels of where historical underinvestment in basic infrastructure have left the working poor, uninsured, and underinsured vulnerable. Social inequalities related to race, ethnicity, and socioeconomic status leads to certain groups being disproportionately exposed to multiple environmental hazards and social stressors.
Methods:
Building on the existing Health and Air Pollution Study cohort (established in 2017) based in the multiethnic urban neighborhoods in South LA, we assessed acute health symptoms, stress measures, and socioeconomic metrics between May and October 2020. We assessed the pandemic-associated traumatic stress score based on a 10-item questionnaire.
Results:
Among the 242 participants that completed a phone-based survey, we identified preexisting high-risk comorbidities: asthma or COPD (19%), diabetes (24%), hypertension (38%), and obesity (48.4%). Nearly four out of five respondents employed before the pandemic reported job loss or reduction of hours. Isolation, family, and economic concerns were among the top stressors reported by participants. Stress related to access to medical care was reported by one-quarter of participants. Stressors were reported more frequency among uninsured participants. Concern over isolation and inability to buy essential items were most associated with higher pandemic-associated traumatic stress score.
Discussion and Conclusions:
Understanding the experiences, stressors, and resources in urban environmental justice neighborhoods are key to design policies and programs aimed at improving the socioeconomic impacts of the current—and in future—public health crises.
INTRODUCTION
Patterns of unequal urban development have resulted in the concentration of poverty, racial segregation, and environmental hazards, which have in turn exacerbated health disparities. 1 The COVID-19 crisis emerged in the United States underpinned by persistent and deepening urban inequities, where historical underinvestment have left the poor, uninsured, and underinsured vulnerable. Poorer families, immigrant communities, and people of color may suffer greater vulnerability owing to differences in preexisting health status; greater co-exposures to pollutants; a compromised ability to cope with the adverse effects of new health insults due to poor nutrition or limited access to health care, preventive, or social services; and modifying effects of psychosocial stress associated with the living in poverty or perceptions of social disadvantage. Black, Indigenous, and People of Color have a disproportionate burden of underlying comorbidities, including diabetes, cardiovascular disease, asthma, morbid obesity, liver disease, and kidney disease.2,3 Social inequalities related to race, ethnicity, and socioeconomic status lead to certain groups being disproportionately exposed to multiple environmental hazards and social stressors, creating a “double jeopardy” that makes such individuals more susceptible to disease and contributes to health disparities.4,5
Black, Indigenous, and Latinx people died at far higher rates from the novel corona virus than other groups in the U.S. 6,7,8 Low-income communities of color in urban settings live in more crowded conditions and are more likely to be employed in public-facing occupations that prevent physical distancing.69 Access to health care and ability to engage in social distancing, builds on known structural inequalities. Disparate exposure to environmental hazards, such as air pollution, are an additional factor that contribute to the disproportionate impact COVID-19 in urban communities of color.10,11 While long-term economic, social, and health consequences of COVID-19 remain uncertain, a recent study of major historical pandemics suggest that the adverse economic consequences of pandemics last for about 40 years and greatly exceed those of wars. 12 Inequalities in living and working conditions result in differences in likelihood of infection and death due to COVID-19. 13 The pandemic revealed that certain populations face more vulnerabilities to health and well-being as a result of the pandemic and its broad sweeping impacts.
In March 2020, Los Angeles (LA) County, California widely implemented and enforced distancing policies, school closures, and limited operations of many businesses with slow and then partial reopening as vaccines became available.14,15 Such policies, affected the daily routines, social relations, health and economic well-being of millions of LA residents. Neighborhoods in South LA comprise a diverse urban community of ∼500,000 predominantly low-income residents of color and are among the most polluted neighborhoods in the state of CA.16,2 In these communities, one finds industrial manufacturing, oil and gas extraction, chemical production, and traffic. At the same time, social stressors, such as under- or unemployment, unsafe working conditions, racism, and social exclusion, may make residents less able to cope with their health problems and perhaps more susceptible to disease, morbidity, and premature mortality.
We conducted a phone-based survey among residents in South LA, an environmental justice community, in the opening months of the pandemic when there remained widespread uncertainty about many aspects of the illness. Our work, grounded in existing community partnerships, sought to contextualize the ways that existing stressors, vulnerabilities, jobs, and access to resources might help structure disease vulnerability and outcomes. Our research aimed to assess impacts due to the pandemic in households in South LA; characterize and understand social stressors in the COVID-19 during the first phase of the pandemic.
METHODS
Environmental justice community cohort
The Health and Air Pollution Study cohort (established in 2017) draws from the multiethnic urban neighborhoods in South LA and was leveraged to assess acute health symptoms, stress measures, and socioeconomic metrics between May 2020 and October 2020. Details of recruitment are available elsewhere. 17 The data collected prior to the pandemic included demographics, physical health history, respiratory health symptoms, household and personal exposures, anthropometric measurements, perceived stress, physical activity patterns, occupational information and residential history. The neighborhoods where the cohort is based is comprised of majority renters (>75%) and when compared to the state, fall into the lowest quintile for educational attainment and the top 15% for poverty. Further, this area is among the top 10% most disproportionately-environmentally burdened neighborhoods in the state according to CalEnviroScreen, CA’s environmental justice screening tool to identify highly burdened and vulnerable communities. The cohort consists of 972 participants from 488 households, including 792 Latinx/Hispanic, 115 Black/African American, 54 Asian/Asian Americans (primarily Korean) from children (starting at age 5) through elders (up to age 95).
One adult member per household member was contacted to complete a phone-based questionnaire about all household members, including children. If a participant was not able to be contacted, due to phone number change, additional contacts of the same household were contacted to provide updated information. Verbal consent was ascertained, and interviews were conducted in English, Spanish or Korean based on the participant preference. All protocols and survey materials were approved by the University of Southern California Institutional Review Board.
Health, economic and social outcomes
The questionnaire was adapted from the World Health Organization COVID-19 health symptoms. The diagnosis of COVID-19 was based self-reported confirmed cases. To ascertain additional impacts of COVID-19 and the associated consequences, we adapted the University of California San Diego COVID-19 Impact Measure for each member of the household. Questions asked about changes in access to medical care, illness, behavioral changes (e.g., social distancing and household cleaning practices), impact on employment status and childcare, changes in access to food and transportation, COVID attitudes and adherence, mental health and stress, neighborhood safety and coping mechanisms (including smoking, exercise, and substance use). For households with children, we asked the adult/caregiver to respond to questions about how child’s healthcare and daily routine (e.g., school, children care and food access) have been impacted by COVID-19, adapted from the National Institute of Health ECHO COVID survey.
Pandemic-associated traumatic stress scale
We used the 10-item questionnaire specific to the COVID-pandemic, which includes five categories: intrusion symptoms, negative mood, dissociative symptoms, avoidance, and arousal symptoms.18,19 The total score was calculated by adding the responses based on a scale of 1 (not at all) to 5 (very often) to reflect general COVID stress severity (range 10–50).
Data analysis
All results were recorded into RedCap database, and survey data were linked to previously collected health measurement and questionnaires using a common ID. We explored the prevalence of conditions and impacts by various factors, including vulnerability factors. Further assessment of the role of race, age, preexisting co-morbidities, smoking history, and immigration status on the variables collected was performed. We assessed the association between various health symptoms (yes vs. no) and pandemic-related worries (highly concerned vs. not concerned) with the pandemic-associated traumatic stress score. Models were ran separately and adjusted for sex and age (binary category of over age 65 or 65 and under). Data were analyzed with STATA 15 IC.
RESULTS
Characteristics of the study participants
A total of 242 adults participated in the survey (Table 1) across two neighborhoods in South LA. The average age of the participants was 53 (range 19–96), and 28% were 65 years of age or older at the time of the interview. The majority of the participants identified as female (72.6%). This cohort was racially/ethnically diverse: 68.5% (n = 165) identified as Hispanic/Latinx, 17% (n = 41) identified as Black or African American, 7.9% (n = 19) identified as Asian or Asian–American and 6.6% (n = 16) as multi-racial. Nearly two-thirds preferred a language other than English to complete the interview. Among the participants, 60% were high school graduates while one in six lacked health insurance. Ninety households resulted having children living in the home, ranging from 1 to 6 children with a median of two. Among the participants, we identified preexisting high-risk comorbidities including asthma or COPD (19%), diabetes (24%), hypertension (38%), and obesity (48.4%), based on body mass index (BMI) measured at baseline entry to the study. Seventy-three people reported ever smoking. Compared with the full adult cohort (n = 654), the sub study was slightly younger, more female, and less likely to be a current smoker (Supplementary Table S1)
Study Demographics
COVID-19-Related Stressors and Coping Mechanisms.
Bolded if proportions differ significantly (p < 0.05) from the comparison group based on the Independent-Samples Mann–Whitney U Test.
COVID-19, health concerns and health care access during the early pandemic
At the time of the interview, 142 (58.7%) reported experiencing at least one symptom of COVID since March 1, 2020. Of those reporting any symptoms, 27 reported fever, 41 cough, 32 shortness of breath, and 12 loss of smell. Forty-five people reported isolating due to symptoms. Sixty-eight participants said they received at least one COVID test and 11 participants reported a positive diagnosis. The most common reasons for not getting tested included lack of available appointments, long wait times and fear of leaving one’s home. Nearly two in five participants reported skipping a medical appointment due to fear of COVID-19, including among those with chronic health conditions. In addition, about 28% of participants had appointments cancelled by their health care provider and 43% switched to tele-medicine visits.
Impacts on employment and financial security
Approximately 60% were employed before the lockdown orders. Most participants worked in essential sectors (see Supplementary Table S2). The top employment sector was child or elder care (n = 33). In addition, participants worked cleaning and maintenance, fast food restaurants, and manufacturing. Fourteen participants worked in health services including nursing, health promotion, and pharmacy. A total of 41% of respondents employed before pandemic experienced a temporary job loss and another 30% faced reduced work hours. About 12% reported a permanent job loss, while 6% obtained new employment after the lockdown began. A total of 14% of participants reported that their current employment put them at increased risk of contracting COVID-19. Only eight people reported that their employer provided them to personal protective equipment (PPE) to reduce risk of COVID.
Government support programs were accessed by many households during the early pandemic. A total of 138 households reported receiving the federal stimulus check, which was most often used to pay for rent and food. Thirty-six people received unemployment aid either through California’s Pandemic Unemployment Assistance, whereas 17 people received a combination of unemployment benefits and the stimulus check. However, 66 households reported not receiving any financial support.
Impacts on travel and transportation
Nearly 80% of people reported traveling away from their home less frequently during the pandemic. About one-fifth of the respondents relied on public transportation such as buses and another 16% primarily traveled by walking or biking. When only considering high-risk participants, one in four relied on the bus, and a similar number using rideshare as primary mode of transportation. Only 5% of respondents reported walking more during the pandemic.
Food access
During the early pandemic, nearly half of the participants reported had difficulty finding food locally, and 15% reported having to travel farther to acquire basic foods. Families and elderly people relied on food banks (18.2%) or senior food programs (6.2%), and 10.7% of households with children used the LA Unified School District (LAUSD) food program. Some households with children also expressed that they were not able to obtain food from LAUSD owing to their child’s school being located far or not having means of transportation.
Digital communication and information sources
About three-fourths of participants has access to high-speed internet; however, 15.7% of households only had access to the internet via their cellphone and 10.7% reported no access to the internet. When looking at sources of trusted information about COVID-19, a majority (82.6%) relied on television news. Others also reported that they obtained COVID-19 from family/friends, social media, and the Los Angeles County Department of Public Health, 29.8%, 27.7%, and 21.5%, respectively.
STRESS, COPING AND WELL-BEING
COVID-related worries
Isolation, family, and economic concerns were among the top stressors reported by participants (Fig. 1). Over 50% of participants were “very concerned” about getting sick with COVID-19 compared with 19% who said they were “not concerned.” When asked about am at-risk family member getting COVID-19, over 63% reported “very concerned.” The most prominent stress factor was impact on family (61.2%), followed by stress due to quarantine/social distancing (59.5%). Other significant stress factors included health concerns (57.9%), impact on the community (53.7%), and financial concerns (52%) (Table 2). Almost half of the sample reported being very concerned about not being able to pay bills. In regard to isolation, 38% reported being very concerned about being socially isolated by themselves and 43% reported being very concerned if family members were to be socially isolated. Stress related to access to medical care was reported by one-quarter of participants. Stressors were reported more frequency among uninsured participants. Talking with friends was the more frequently reported activity to help cope with the impacts of the pandemic and shutdown. Watching television, reading, and eating were also common activities. Fewer people reported relying on alcohol or smoking to cope with the pandemic’s impacts.
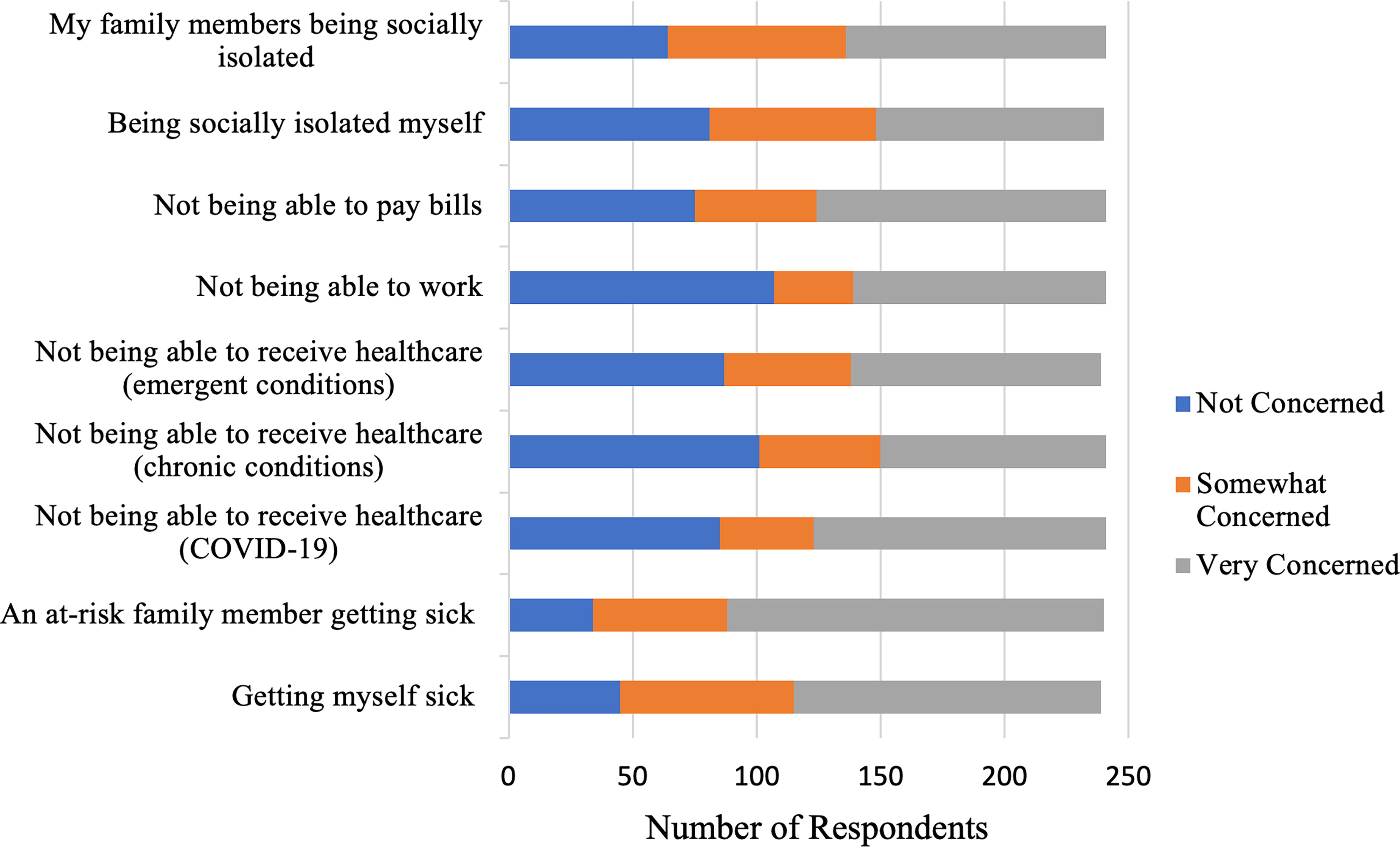
COVID-19 concerns reported during the early phase of the pandemic.
Pandemic-associated traumatic stress scale
Nine participants did not complete all questions and were excluded from pandemic-associated traumatic stress scale (PTSS) analyses, for a total of 233 people. Participants scores ranged from 10 to 42, with a mean of 22. Among vulnerable groups, participants without medical insurance reported higher scores on the PTSS compared with others (24 vs. 22). On average being very concerned about not being able to buy essential items (β: 7.2; 95% confidence interval [CI] 3.1–11.3) and isolation (β: 7.2; 95% CI 5.1–9.3) were associated with the largest increased in PTSS scores. Experiencing a COVID-related health symptom during the early pandemic was associated with largest increases in PTSS (Fig. 2) adjusted for sex and age when compared with participants who expressed no concern. Experiencing COVID-related health symptoms were associated significantly associated with increases in PTSS compared with those who did not report experiencing the health symptom. While, we evaluated the association between pandemic coping mechanism and PTSS, the only significant finding was a decrease in PTSS among those reporting eating more (β: 3.0; 95% CI 1.2–4.9).
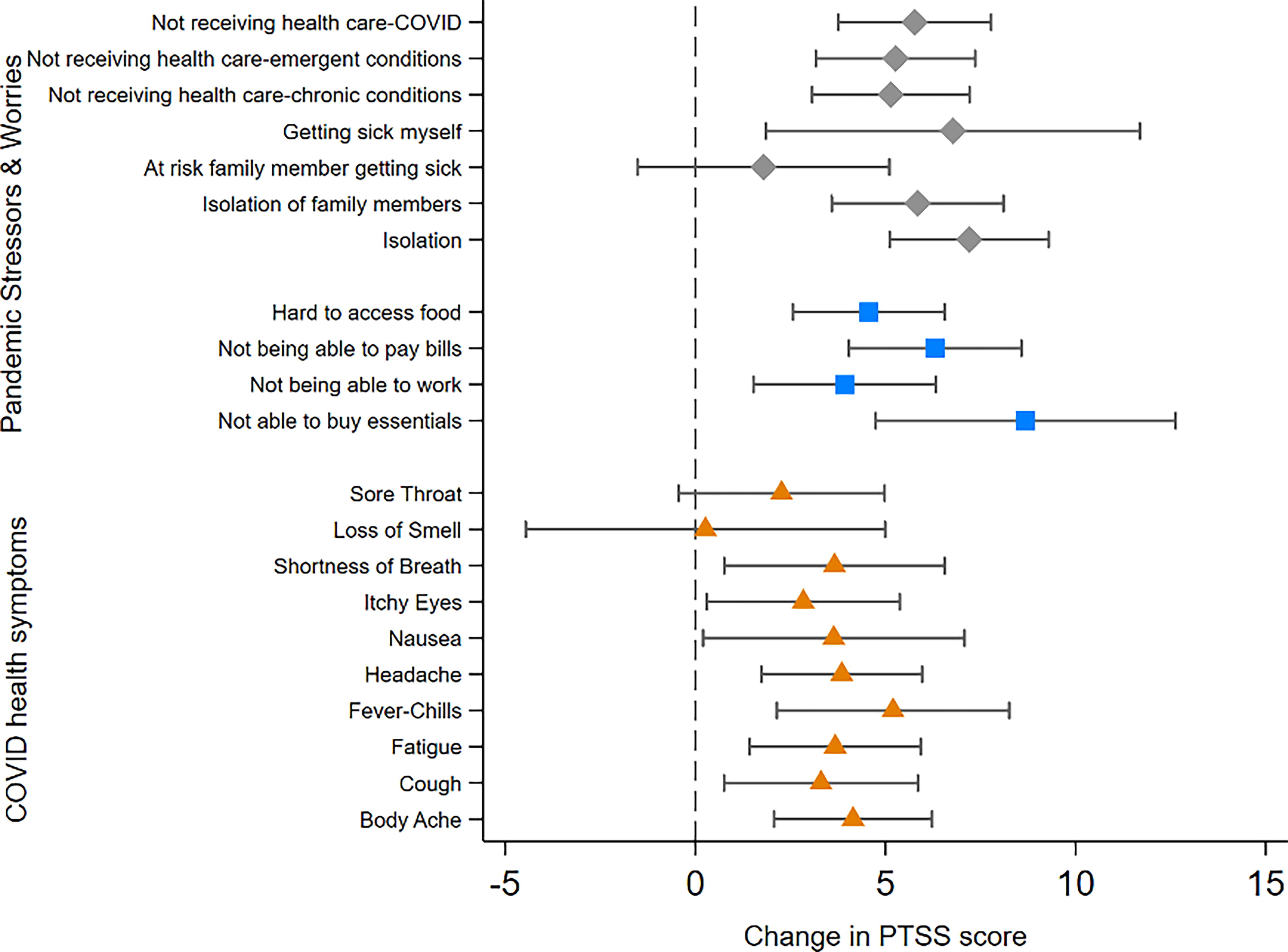
Results of separate regression models on the associated between self-reported pandemic-related worries (comparing very concerned with not concerned group) and COVID-19-related health symptoms on PTSS score. All models were adjusted for sex and age. PTSS, pandemic-associated traumatic stress scale.
DISCUSSION
The work aims to characterize the lived experiences of residents living in South LA in the early phase of the pandemic and help reveal quality of life factors that help contextualize future data on morbidity and mortality rates that would disproportionately burden this community, the ways that existing stressors, vulnerabilities, jobs, and access to resources might have helped structure disease vulnerability and outcomes. In this study, we describe immediate impacts to families in urban environmental justice neighborhoods during the initial lockdown, and choices and lack of choices that might determine the ability of many families to work from home, the challenges of caring for children and elderly at home, and reliance of employment in low wage, heavily impacted sectors such as in health facilities. Environmental justice communities, before the pandemic, often develop coping mechanisms to contend with living in overburdened communities or working in vulnerable professions. 20 How individuals experience and cope with stressors affects whether and how they seek medical care, and whether and how well they adhere to health professionals’ advice, including whether they are able to implement health advice, such as the challenges of social distancing or isolation in cramped living spaces. Reactions to stressors can promote or inhibit healthful practices and influence motivation to practice habits that promote health. 21
As the COVID-19 crises unfolded, vulnerable families in South LA were already coping with structural inequality. The concentration of workers in industries such as home health care, housekeeping, restaurants, salon work, retail, and wholesale trade meant that residents were both hard-hit by spending cutbacks and more exposed in jobs on the frontlines of busy or essential sectors. Underserved communities are already distrustful of public health institutions; communities of color and people with disabilities have historically been undertreated or abused through the medical system, and undocumented immigrants fear punitive measures should they access social services or present at a clinic or hospital.22,23,7
In neighborhoods already burdened by cumulative environmental and social burdens residents also disproportionately worked in professions that were hard hit by the pandemic in later months. Susceptibility to underlying health conditions such as hypertension, diabetes, high blood pressure, and asthma play a role in the disparities in mortality from COVID-19, these are also known to be illnesses of racism, poverty, and associated with exposure to environmental toxins. 24 Thus, the risk factors for COVID-19 complications should be examined within the context of environmental racism, and the adverse social determinants of health that put such communities at increased risk for disease.
Analysis of mortality data across California during the early pandemic, found higher disparities in mortality from COVID-19 for Blacks and Latinxs individuals; such disparities were larger among adults under 65 years old. Research shows that foreign-born and non-citizen individuals also faced disproportionately higher mortality rates.25,3,4 While there is data on the racial disparities that shaped morbidity and mortality from COVID, fewer studies have documented how residents experienced the pandemic in the early phases, the tradeoffs they were able to make, how they coped with shutdowns, and how their existing lived realities might have shaped health outcomes as the pandemic played out neighborhood by neighborhood and family by family.
People of color are more likely to be employed in essential industries and in occupations with more exposure to infections and close proximity to others. 26 Nearly 40% of low-income households in LA experienced food insecurity during the first months of the pandemic. 27 Immigrant families faced additional complicating factors (e.g., employment in jobs with higher potential exposure, lack of medical care and paid leave, multigenerational housing, less access to social safety net) which should be considered for public health approaches.28,29 The pandemic unfolded as a disaster for many groups, revealing and worsening existing social fractures, and leaving the most vulnerable with few coping resources in terms of interruptions to income, medical costs, and other variabilities. In this context, with growing evidence if disparate harm, there is critical need to structure supports for communities at different institutional levels (home, school, work), sectors, and age.
Previous research also shows that women, unemployed, low-income, and those living in segregated communities are more at risk for exposure to pandemic stressors. 30 These groups often have fewer resources, and are therefore more likely to experience adverse mental health effects. The COVID-19 pandemic is occurring against a backdrop of social and economic inequalities together with health disparities which are spatially patterned. 31
CONCLUSIONS
COVID-19 is a pandemic that has highlighted the issues of vulnerability, marginalization, and health disparities, reaffirming how the physical environment and health are intertwined. Nonetheless, research and practice in public health education and interventions in the U.S. context has a long tradition of focusing on individual behavior change to promote population health. 32 However, the limits of individual level interventions have been challenged as insufficient for population level protections, particularly in the context of vulnerable populations or environmental justice communities. 33 Understanding the experiences, stressors, and resources in urban environmental justice neighborhoods are key to design policies and programs aimed at improving the socioeconomic impacts of the current—and in future—public health crises.
Footnotes
AUTHORS’ CONTRIBUTIONS
J.J. and B.S. conceptualized the research and acquired funding. J.J. wrote the original draft and supervised the project. B.S. revised and edited the article. M.T. and A.J. led the project administration, investigation, and data collection.
AUTHOR DISCLOSURE STATEMENT
The authors have no conflicts to disclose.
FUNDING INFORMATION
This work was supported in part by a grant from the University of California Office of the President (
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.