
Abstract
With the emergence of multidrug-resistant nontyphoidal (NT) Salmonella, knowledge of resistance patterns is critical for appropriate presumptive treatment. This report describes the prevalence and trends of NT Salmonella antimicrobial susceptibility within the New York State (NYS) Foodborne Diseases Active Surveillance Network (FoodNet). The NYS Department of Health, Wadsworth Center Public Health Laboratory tested all Salmonella isolates from the NYS FoodNet catchment area between May 2003 and December 2007 for antimicrobial susceptibility to ampicillin, chloramphenicol, streptomycin, sulfisoxazole, tetracycline, nalidixic acid, and ciprofloxacin. Isolate susceptibility results were linked to their corresponding demographic and clinical data and analyzed. Multidrug-resistant isolates were defined as resistant to ampicillin, chloramphenicol, streptomycin, sulfisoxazole, and tetracycline (R-type ACSSuT). Antimicrobial susceptibility for 2189 FoodNet cases (98.5% of total cases) showed 79.6% pansusceptible, 6.9% R-type ACSSuT, and 13.5% resistant to at least one antimicrobial agent but not R-type ACSSuT. Four (0.2%) isolates were resistant to ciprofloxacin. From 2004 to 2007, cases with R-type ACSSuT significantly decreased from 8.7% (37/424) to 4.8% (24/499) (p < 0.01). Serotypes with the highest proportion of R-type ACSSuT included Salmonella Typhimurium 17.9% (79/444), and Salmonella Newport 29.1% (51/175). Among Salmonella Typhimurium isolates, over 40% of the African-American cases (19/46) had R-type ACSSuT isolates, compared with 15.7% of the Caucasian cases (58/369) (p < 0.01). R-type ACSSuT Salmonella Typhimurium cases were hospitalized (41.8%) more frequently than pansusceptible Salmonella Typhimurium cases (24.9%), after controlling for age (p < 0.05). Length of hospitalization was not significantly different. Although R-type ACSSuT NT Salmonella has decreased since 2003 within the NYS FoodNet catchment area, monitoring resistance patterns remains important in identifying emerging resistant strains, vulnerable populations, and determining appropriate presumptive treatment regimens. The higher rate of R-type ACSSuT among the African-American cases requires further study.
Introduction
Multidrug-resistant (MDR) NT Salmonella first appeared in the 1960s but attained more prominence as a public health concern in the 1990s, with the emergence of a MDR strain of Salmonella Typhimurium definitive phage type 104 (DT104) (resistant to ampicillin, chloramphenicol, streptomycin, sulfisoxazole, and tetracycline) associated with more invasive disease and a higher case fatality rate (Threlfall, 2002; Travers and Barza, 2002; Helms et al., 2005). From 1979 to 1996, the percentage of MDR Salmonella Typhimurium isolates increased from 0.6% to 34% in the United States (Glynn et al., 1998).
MDR NT Salmonella is typically acquired from consumption of the contaminated food derived from animals (Cohen and Tauxe, 1986; Angulo et al., 2000). Increased levels of MDR NT Salmonella within these food products have corresponded to increased use of antibiotics in food animals for therapeutic purposes, disease prevention, and growth promotion (McEwen and Fedorka-Cray, 2002; Anderson et al., 2003; WHO, 2004).
With the emergence of MDR NT Salmonella, knowledge of current resistance patterns becomes critically important in determining appropriate initial treatment regimens as antibiotic susceptibilities are rarely known before treatment (Travers and Barza, 2002). To better understand MDR NT Salmonella trends, in 2003, the New York State Department of Health (NYSDOH) Wadsworth Center Public Health Laboratory began antimicrobial susceptibility testing of all Salmonella isolates received. This report describes the prevalence and characteristics of NT Salmonella antimicrobial susceptibility within the New York State (NYS) FoodNet catchment area from 2003 to 2007.
Materials and Methods
Study population
FoodNet is a core program within the Centers for Disease Control and Prevention (CDC)'s Emerging Infections Program tasked with assessing the burden of foodborne illness within the United States through active laboratory-based surveillance of specific foodborne pathogens including Salmonella. New York became a FoodNet site in 1998, with a catchment area that presently includes 34 counties in the Albany, Rochester, and Buffalo regions, representing approximately 4.3 million residents.
NYS Public Health Law requires laboratories and physicians to report all salmonellosis cases to local health departments (LHDs) and submit isolates to the NYSDOH Wadsworth Center Public Health Laboratory for diagnostic confirmation and speciation. LHDs collect standardized data for each case including age, race, ethnicity, hospitalization, outbreak status, travel history, vital status, and isolate source. The LHDs submit all case information to the NYSDOH through a secure web-based data collection system. Within the FoodNet counties, surveillance officers actively monitor clinical laboratories and contact LHDs to ensure ascertainment of all laboratory-confirmed salmonellosis cases and review case reports for accuracy and completeness.
Antimicrobial resistance
Beginning May 1, 2003, the NYSDOH Wadsworth Center Public Health Laboratory performed susceptibility testing against a limited panel of antimicrobial agents on all Salmonella isolates received as an internal mechanism to assist in state outbreak and cluster investigations. Susceptibility to ampicillin, chloramphenicol, streptomycin, sulfisoxazole, tetracycline, and ciprofloxacin was evaluated using the Kirby–Bauer disc diffusion method (Bauer et al., 1966). This specific panel of antibiotics was chosen because of their association with MDR Salmonella Typhimurium DT104. Beginning in 2005, nalidixic acid, an elementary quinolone, was added to the panel as a screening test for potential ciprofloxacin resistance, with ciprofloxacin susceptibility testing only performed on nalidixic acid–resistant isolates. Isolates were categorized as sensitive, intermediate, or resistant to each antimicrobial agent using the zone diameter interpretation guidelines defined by the Clinical and Laboratory Standards Institute (CLSI, 2009).
Minimum inhibitory concentrations (MICs) of ciprofloxacin were determined for all isolates resistant to either nalidixic acid or ciprofloxacin using the E-test method (AB Biodisk, Piscataway, NJ). Ciprofloxacin resistance was defined as a MIC of ≥4 μg/mL, in accordance with the CLSI guidelines (CLSI, 2009). Decreased susceptibility to ciprofloxacin was defined as a MIC of ≥0.125 μg/mL (Hakanen et al., 1999; Stevenson et al., 2007).
Data analysis
Confirmed cases of NT Salmonella within the FoodNet surveillance area from May 2003 to December 2007 for whom isolates were submitted to the state laboratory were analyzed. Epidemiologic case reports were linked to antimicrobial susceptibility results using unique laboratory identification numbers. For this analysis, isolates determined to have intermediate susceptibility values were categorized as sensitive. Pansusceptible isolates were sensitive to all tested antimicrobial agents. The multidrug resistance pattern analyzed was defined as resistance to at least ampicillin, chloramphenicol, streptomycin, sulfisoxazole, and tetracycline (R-type ACSSuT). Isolates resistant to at least one antimicrobial agent but not R-type ACSSuT were grouped as other resistance patterns. Isolate source was categorized as blood, stool, urine, other, or unknown. Other sources included abscesses, bone, gallbladder, joint, sputum, wound, and gastrointestinal aspirate.
Cases were considered hospitalized if hospitalization occurred within 7 days before or after the specimen collection date. Vital status was assessed at hospital discharge for hospitalized cases or 7 days after the specimen collection date for the nonhospitalized cases. A positive travel history was defined as having traveled internationally within 7 days of illness onset.
As Salmonella pathogencity varies greatly by serotypes (Jones et al., 2008), demographic and clinical characteristics comparisons by antimicrobial pattern were limited to Salmonella Typhimurium and Salmonella Newport, as these serotypes accounted for over 86% of the R-type ACSSuT isolates. Demographic and clinical characteristics were compared using the chi-square test and Fisher's exact test, where appropriate, as well as the Cochran–Mantel–Haenszel statistic for age adjustment. The Wilcoxon rank-sum test was used to compare the median age.
Multidrug resistance temporal trends were evaluated using the Poisson regression model to account for the variations in the NYS FoodNet surveillance population and NT Salmonella case frequency. The first complete year of susceptibility testing (2004) was used as the baseline for comparisons. A p-value < 0.05 was considered statistically significant. All data analysis was completed using SAS (Statistical Analysis Software, v9.1) (SAS Institute, Cary, NC).
Results
From May 2003 to December 2007, 2223 NT Salmonella cases were identified in the NYS FoodNet catchment area. Antimicrobial susceptibility testing was completed on the isolates of 98.5% of the cases (n = 2189). The most common serotypes included Typhimurium (n = 444), Enteritidis (n = 392), Newport (n = 175), Heidelberg (n = 170), and Tennessee (n = 77).
Ciprofloxacin and nalidixic acid resistance
Four isolates were resistant to ciprofloxacin (MICs >32 μg/mL), with all but one occurring in 2004 (Table 1). Resistance to nalidixic acid increased from 1.5% in 2005 (year nalidixic acid resistance testing began) to 2.6% in 2007. One isolate resistant to nalidixic acid was also resistant to ciprofloxacin by both disc diffusion and MICs. Over 86% of the remaining isolates resistant to nalidixic acid had reduced ciprofloxacin susceptibility, with MICs ranging from 0.125 to 0.75 μg/mL.
Susceptibility testing: May to December 2003 only.
Resistance to at least ampicillin, chloramphenicol, streptomycin, sulfisoxazole, and tetracycline.
Resistance to ≥1 antimicrobial agent but not R-type ACSSuTb.
Nalidixic acid susceptibility testing began in 2005 as a screening test for ciprofloxacin resistance.
Three ciprofloxacin-resistant isolates in 2004 represented a cluster of Salmonella Schwarzengrund from one family. The other ciprofloxacin-resistant isolate was Salmonella Kentucky. There was no history of international travel elicited from the ciprofloxacin-resistant cases.
Multidrug resistance
Overall, almost 80% (n = 1742) of the NT Salmonella isolates were pansusceptible, 7% (n = 151) were R-type ACSSuT, and 14% showed other resistance patterns (Table 1). Substantial declines in resistance to almost all antimicrobial agents were observed, most declining from levels of 15–20% in 2003 to 6–12% in 2007.
R-type ACSSuT varied by serotype with the highest proportions occurring in Typhimurium 17.8% (79/444), Newport 29.1% (51/175), Dublin 75% (6/8), Paratypi B. var. L (+) tartrate (+) 40% (4/10), and Choleraesuis 66.7% (2/3). Although second only to Salmonella Typhimurium in the overall incidence, there was only one Salmonella Enteritidis isolate that was R-type ACSSuT (Table 2).
Resistance to at least ampicillin, chloramphenicol, streptomycin, sulfisoxazole, and tetracycline.
Temporal trends of antimicrobial resistance
NT Salmonella with R-type ACSSuT decreased significantly from 8.7% in 2004 to 4.8% in 2007 (p < 0.01), whereas the proportion of pansusceptible isolates rose from 78.1% to 82.6% between 2004 and 2007 (Fig. 1). When stratified by serotype, the proportion of R-type ACSSuT isolates decreased in both Salmonella Typhimurium and Salmonella Newport serotypes from 2004 to 2007, with year to year variations (Fig. 2). Overall, R-type ACSSuT Salmonella Typhimurium isolates declined from 20.5% to 12.5% between 2004 and 2007 (p = 0.045), with the highest rate, 25.5%, occurring in 2005. R-type ACSSuT Salmonella Newport isolates decreased from 43.6% in 2004 to 17.4% in 2007 (p = 0.083) with the lowest level of resistance appearing in 2005 (10.7%).
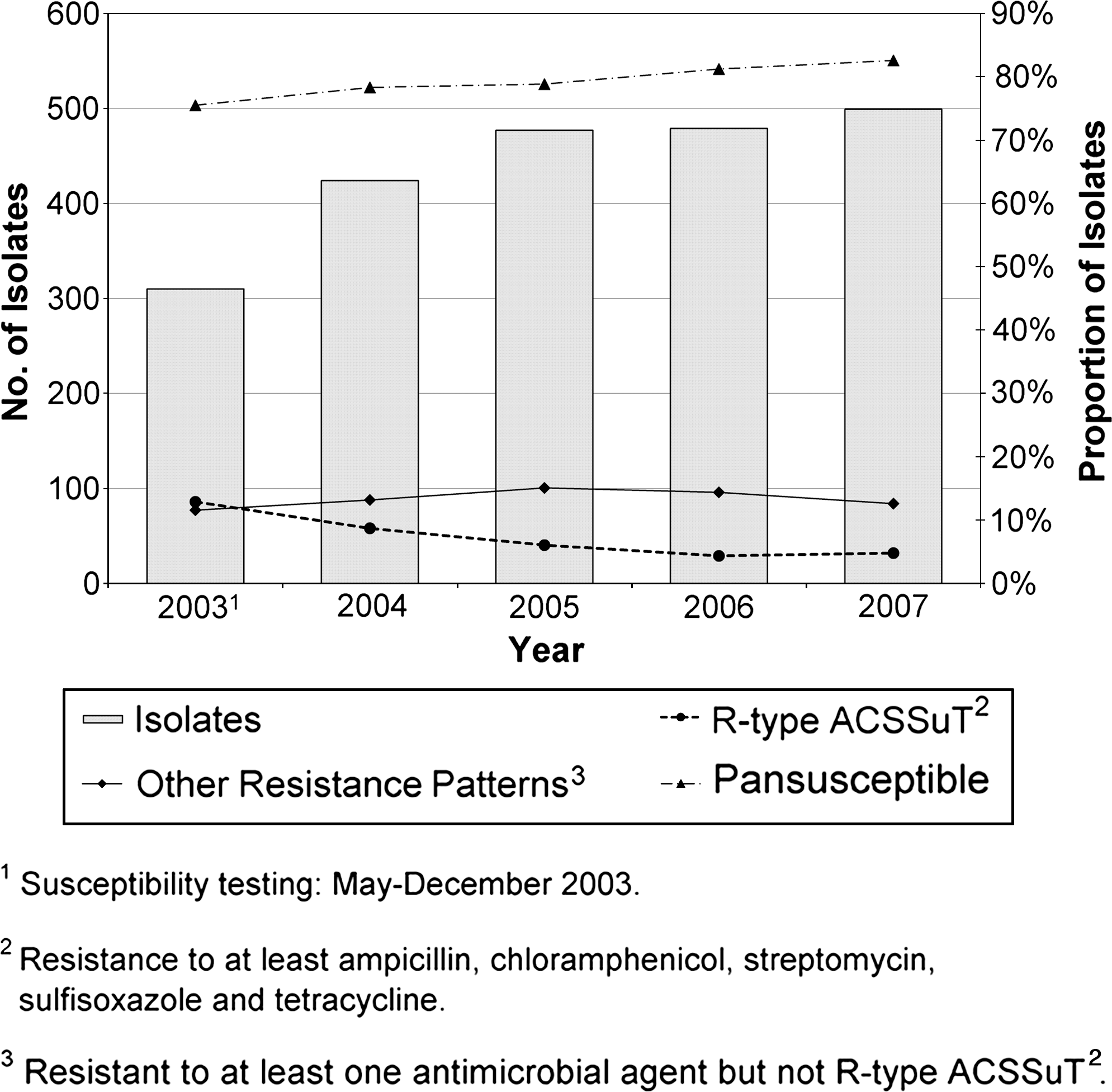
Nontyphoidal Salmonella temporal trends by antimicrobial resistance patterns within New York State Foodborne Diseases Active Surveillance Network, 2003–2007.
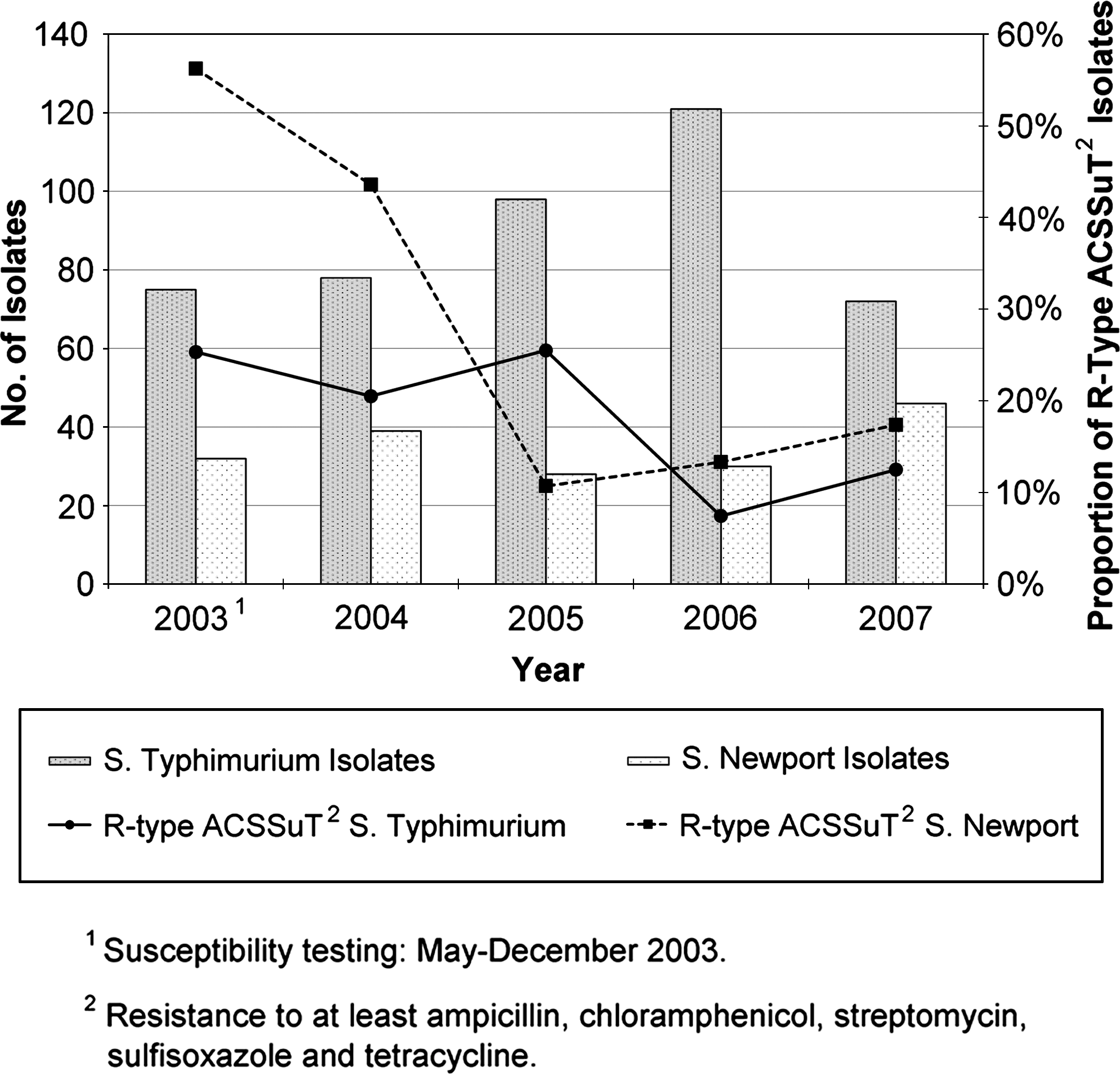
Salmonella Typhimurium and Salmonella Newport temporal trends for R-type ACSSuT2 isolates within New York State Foodborne Diseases Active Surveillance Network, 2003–2007.
Outbreaks
Outbreaks were more likely to be associated with pansusceptible isolates (10.5%) than R-type ACSSuT isolates (5.3%) (p = 0.04). Only eight R-type ACSSuT isolates were associated with outbreaks. Six of these isolates were associated with a 2004 multistate summer cluster of Salmonella Newport of an undetermined source with the same resistance profile and pulsed-field gel electrophoresis pattern. The remaining two cases were related to a small Salmonella Typhimurium outbreak in the spring of 2005 associated with a Mother's Day brunch in Canada.
Demographic and clinical characteristics
No significant differences in demographic and clinical characteristics were found when comparing resistance patterns of Salmonella Newport cases. Therefore, the following results are limited to Salmonella Typhimurium cases only.
Among all Salmonella Typhimurium African-American cases, 41.3% (19/46) expressed R-type ACSSuT compared with 15.7% (58/369) among Caucasians (p < 0.01). Relative to the other serotypes, infections with Salmonella Typhimurium occurred at a significantly higher frequency among African-American cases (32.2%) than Caucasian cases (19.6%) (p < 0.01).
R-type ACSSuT cases were significantly older (median age, 41 years) than pansusceptible cases (median age, 25 years) (p < 0.01) (Table 3). No significant differences were observed for gender, ethnicity, or international travel history.
Resistance to at least ampicillin, chloramphenicol, streptomycin, sulfisoxazole, and tetracycline.
Resistance to ≥1 antimicrobial agent but not R-type ACSSuTa.
R-type ACSSuTa compared with pansusceptible cases.
Referent category.
Significant when compared with pansusceptible cases (p = 0.017).
Fisher's exact two-tailed p-value.
Adjusted for age using the Cochran–Mantel–Haenszel statistic.
R-type ACSSuT cases were hospitalized more frequently (41.8%) than pansusceptible cases (24.9%), after age adjustment (p = 0.035). The length of hospitalization was similar for R-type ACSSuT and pansusceptible cases (4.0 vs. 4.5 days, respectively). More R-type ACSSuT isolates (6.3%) were obtained from blood than pansusceptible isolates (3.3%). Fatality was notably higher in cases with R-type ACSSuT isolates (3.8%) than in cases with pansusceptible isolates (0.3%); however, the difference was not significant when adjusted for age (p = 0.07).
Discussion
In NYS FoodNet counties, 0.2% of the isolates were resistant to ciprofloxacin, a fluoroquinolone, with all but one case part of a cluster within the same family. However, the near doubling of nalidixic acid resistance between 2005 and 2007 is the cause for concern. Similarly, the CDC's National Antimicrobial Resistance Monitoring System (NARMS) noted a significant increase in nalidixic acid resistance from 0.4% in 1996 to 2.7% in 2006 (CDC, 2009).
Previous studies have reported that Salmonella isolates resistant to nalidixic acid tend to have reduced ciprofloxacin susceptibility, even when these isolates are found to be ciprofloxacin susceptible using the disc diffusion method (Lewin et al., 1991; Hakanen et al., 1999; Szych et al., 2001; CLSI, 2009). While only one nalidixic acid–resistant isolate was also ciprofloxacin resistant, almost all the nalidixic acid–resistant isolates exhibited a decreased susceptibility to ciprofloxacin, indicating the potential for a possible treatment failure in patients treated with fluoroquinolones. The increasing trend of nalidixic acid resistance suggests a potential underestimation of ciprofloxacin resistance.
The proportion of NT Salmonella R-type ACSSuT isolates significantly decreased in NYS FoodNet counties from 8.7% in 2004 to 4.8% in 2007. NARMS reported that the prevalence of R-type ACSSuT isolates in the United States in the most recent years has been declining from 9.3% in 2003 to 5.5% in 2006, ranging from 5.5% to 10% each year (CDC, 2009). By serotype, NARMS reported a significant decrease in Salmonella Typhimurium with R-type ACSSuT resistance pattern from 33.7% in 1996 to 19.7% in 2006, similar to the declines within NYS FoodNet counties between 2004 and 2007. There have been no recent regulatory changes to antibiotic use in food animals in NYS, so an explanation for the declines in R-type ACSSuT Salmonella Typhimurium is not clear.
In contrast to the decline seen with Salmonella Typhimurium, NARMS found that R-type ACSSuT Salmonella Newport isolates increased from 5.9% in 1996 to a high of 25.8% in 2001, with a subsequent drop to 12.0% in 2006 (CDC, 2009). The surge in MDR Salmonella Newport between 1996 and 2001 coincided with the emergence of MDR AmpC-resistant Salmonella Newport (resistant to at least ACSSuT and amoxicillin–clavulanic acid, cephalothin, cefoxitin, and ceftiofur) that was associated with dairy cattle between 1998 and 2003 (Gupta et al., 2003). The NYSDOH Wadsworth Center Public Health Laboratory began antimicrobial resistance testing in 2003, following the peak noted within both NARMS and the dairy cattle population, as the portion of R-type ACSSuT Salmonella Newport isolates declined from 43.6% in 2004 to 17.4% in 2007.
Previous studies have associated Salmonella Dublin isolates with higher proportions of invasive disease, hospitalization, and case fatality (Werner et al., 1979; Vugia et al., 2004; Jones et al., 2008). Most of the Salmonella Dublin cases in the present study express R-type ACSSuT. The high portion of Salmonella Dublin R-type ACSSuT isolates coincided with the emergence of a MDR strain of Salmonella Dublin within the northeastern cattle industry between 2005 and 2006 (Cornell University Animal Health Diagnostic Center, 2006). This highlights the importance of how monitoring emerging resistance patterns in the cattle industry can potentially serve as forewarnings of resistance patterns likely to emerge within the human population and lead to more effective treatments, particularly with known invasive Salmonella serotypes.
The increased prevalence of R-type ACSSuT Salmonella Typhimurium isolates observed among African-Americans warrants further study. Over 40% of the Salmonella Typhimurium isolates from African-American cases were R-type ACSSuT in contrast to 15.7% of the isolates from Caucasian cases. While the present study and previous studies have shown Salmonella Typhimurium to be more prevalent in African-Americans (Vugia et al., 2004; Arshad et al., 2007), a difference in the proportion of R-type ACSSuT within Salmonella Typhimurium isolates by race was not expected. One study conducted in the early 1990s by Lee et al. (1994) found African-Americans more likely to be infected by a resistant strain of NT Salmonella and surmised the difference was partly attributable to the Salmonella serotype as well as differences in food preferences, food preparation techniques, or cultural influences. Research to identify factors that contribute to the observed differences in antimicrobial susceptibilities by race is needed.
Previous studies have associated MDR NT Salmonella with more invasive disease. Varma et al. (2005) found that patients with NT Salmonella isolates resistant to ampicillin, ceftriaxone, ciprofloxacin, gentamicin, and/or trimethoprim–sulfamethoxazole were more likely to be hospitalized. Lee et al. (1994) found that NT Salmonella cases resistant to a median of three antimicrobial agents were more likely to be hospitalized compared with pansusceptible cases after adjustments for prior antimicrobial use and underlying diseases. Helms et al. (2002) observed higher rates of mortality associated with R-type ACSSuT strains of Salmonella Typhimurium than with pansusceptible isolates in the Danish population.
In the present study, cases with R-type ACSSuT NT Salmonella Typhimurium isolates were associated with increased hospitalization and mortality rates compared with Salmonella Typhimurium pansusceptible isolates. No significant differences were identified between R-type ACSSuT and pansusceptible isolates of Salmonella Newport. Devasia et al. (2005) also found no difference in hospitalization rates when comparing Salmonella Newport MDR-AmpC and pansusceptible cases. These results suggest that the severity of illness associated with NT Salmonella is influenced by serotype as well as drug resistance pattern.
This study has several limitations. Only a small panel of antimicrobial agents was assessed for each isolate. While these findings suggest a declining trend in antimicrobial resistance, different trends may be occurring in antimicrobial agents not included in this analysis. Nalidixic acid resistance was not assessed until 2005. Consequently, resistance trends could not be analyzed for the entire study period. Phage typing was not performed at the state laboratory, so the proportion of Salmonella Typhimurium isolates that were DT104 was not determined. Over 86% of the isolates expressing the R-type ACSSuT pattern were Salmonella Typhimurium or Salmonella Newport. Due to small numbers, we were unable to evaluate trends for other serotypes expressing R-type ACSSuT.
Case report data on previous antimicrobial usage and underlying illnesses were too incomplete for analysis. Previous antimicrobial usage has been shown to be a risk factor for developing MDR Salmonella illness (Lee et al., 1994; Varma et al., 2006). Higher rates of underlying illnesses could have impacted the increased hospitalization and fatality rates shown in Salmonella Typhimurium R-type ACSSuT cases in the present study.
Although R-type ACSSuT NT Salmonella has decreased since 2003 within the NYS FoodNet catchment area, monitoring resistance patterns remains important in identifying emerging resistant strains, vulnerable populations, and determining appropriate initial treatment regimens. It is important to not only monitor resistance patterns emerging in the human population but also consider resistance patterns emerging in foods derived from animals, such as cattle and poultry, to serve as an early warning system of what to anticipate in the human population.
Footnotes
Acknowledgments
The authors thank Dale L. Morse M.D., M.S., from the NYSDOH, Office of Science; Perry F. Smith, M.D. and Kimberly A. Noyes, M.D., M.P.H. from the NYSDOH, Division of Epidemiology; and Frederick J. Angulo, D.V.M., Ph.D., from the Division of Foodborne, Bacterial, and Mycotic Diseases, National Center for Zoonotic, Vector-Borne and Enteric Diseases, CDC, for their assistance and comments in reviewing this article. This project was supported by Cooperative Agreement Number U01/CI000311 from the CDC Emerging Infections Program.
Disclosure Statement
No competing financial interests exist.