
Abstract
Human listeriosis is a rare but serious foodborne disease, with high morbidity and mortality in vulnerable populations (e.g., pregnant women, the elderly, and the immunocompromised). The disease is predominantly caused by the consumption of contaminated ready-to-eat foods. Since 2001, an increase in the number of listeriosis cases has been observed in several European Union countries, including England and Wales, predominantly in the over-60s population. The cause of this selective increased incidence is unknown. The Hald Salmonella Bayesian source attribution model was adapted to determine the potential of this approach to quantify the contribution of different food sources to the burden of human listeriosis in England and Wales from 2004 to 2007. The most important food sources for the overall population were multicomponent foods (sandwiches and prepacked mixed salad vegetables) (23.1%), finfish (16.8%), and beef (15.3%). Attribution of major sources of infection was similar for the elderly population (≥60 years old, multicomponent foods [22.0%], finfish [14.7%], and beef [13.6%]). For pregnancy-associated cases, beef (12.3%), milk and milk products (11.8%), and finfish (11.2%) were more important sources of infection. The adapted model also showed that the serotype 4b was associated with relatively more human infections than that of other serotypes; further, the subtype 4b amplified fragment-length polymorphism V was associated with more pregnancy-associated cases than other subtypes of 4b. This approach of quantifying the contribution of various food sources to human listeriosis provides a useful tool in food safety risk analysis, and underlines the need for further emphasis to be given to the reduction of Listeria monocytogenes in high-risk foods, such as multicomponent foods, which are consumed without any further treatment. The need for targeted dietary advice for the elderly population is also highlighted.
Introduction
Since 2001, an increase in the number of listeriosis cases has occurred in several European Union countries, including England and Wales, predominantly in persons over 60 years old. The reasons to this increase are not known, but they are independent of recognized outbreaks, sex, season, ethnicity, socioeconomic status, region, or L. monocytogenes serotype and/or amplified fragment-length polymorphism (AFLP) type (Gillespie et al., 2006; Goulet et al., 2008). The increase is also not accounted for by an increasing proportion of the population being elderly (ACMSF, 2009).
Source attribution approaches describe an association between the outcome (the burden of a given disease) and the specific sources or exposures (Batz et al., 2005; Pires et al., 2009). Foodborne disease source attribution is increasingly used to partition foodborne disease to the most important sources and as such support public health and food safety risk management and intervention strategies. The source attribution model developed by Hald et al. (2004) has proved successful in the attribution of human salmonellosis to animal-food sources in Denmark and also to other European Union member states, including the United Kingdom (Pires et al., 2008). The approach taken in the Hald model is the microbial subtyping approach where the relative contributions of different sources to human salmonellosis are inferred from the comparison between Salmonella subtypes in human and infection-source isolates. The increase in listeriosis cases emphasizes the need to better estimate the burden of disease and the presence of this pathogen in the food chain. We adapted and applied the Hald model to L. monocytogenes to determine whether such an approach may provide further insight and quantify the relative importance of food sources to listeriosis cases, including risk population groups such as the elderly.
Materials and Methods
Surveillance of L. monocytogenes in England and Wales
The Health Protection Agency (HPA) Centre for Infections surveils human L. monocytogenes infections in England and Wales as described in detail by Gillespie et al. (2006). Epidemiologic and microbiologic data from this surveillance system are combined and stored in a Microsoft Access database. National and routine microbiological food surveillance in England and Wales is also coordinated by the HPA. Within this food surveillance program, L. monocytogenes isolates obtained from ready-to-eat foods sampled from retail and food service premises have been referred since 2004. Food descriptions and microbiological data are also stored in the Access database.
All L. monocytogenes isolates from patient cases and food referred to HPA Centre for Infections are confirmed by polymerase chain reaction (McLauchlin, 1997). Isolates are characterized into subtypes by serotyping and AFLP analysis (Guerra et al., 2002; Doumith et al., 2004).
Data included in the model
Data that were used as input for the model included only data collected as part of the L. monocytogenes surveillance programs described above and represented the years 2004–2007 (Table 1).
Pates, chopped livers, and fermented meats.
Sandwiches and prepacked mixed vegetable salads.
Desserts and cooked rice.
Included subtypes that caused human listeriosis but were not isolated from the investigated food sources.
AFLP, amplified fragment-length polymorphism.
Food descriptions were classified according to the food type (poultry, red meat, etc.) and the main ingredient (chicken, pork, etc.). In total, 1529 isolates from 13 ready-to-eat food sources were included in the analysis: beef, pork/ham, tongue, other red meat products (pates, chopped livers, and fermented meats), chicken, turkey, game bird, finfish, shellfish, milk/milk products, salad vegetables/fruit, multicomponent foods (e.g., sandwiches and prepacked mixed vegetable salads), and other foods (e.g., desserts and cooked rice) (Table 1).
Since the purpose of the model was to quantify the relative importance of ready-to-eat food sources to listeriosis cases within risk groups, we categorized cases as pregnancy-associated (all maternal–fetal patients and neonatal patients; a mother–baby pair was considered as one case-patient) and nonpregnancy-associated (patient >1 month of age). Nonpregnancy case-patients were categorized further into those who were over 60 years or not. Three scenarios were investigated, two of them corresponding to risk groups, and one for the overall population. In total, 564 sporadic cases of listeriosis were reported in the overall population from 2004 to 2007 (Table 1). Among these cases, 538 were caused by 20 L. monocytogenes sero-AFLP subtypes, which were isolated from different food sources accounted for in the analysis. These 20 L. monocytogenes sero-AFLP subtypes were included in this scenario analysis, along with a “type” labeled as “others” that included subtypes (1/2a XIII, 1/2a XIX, 1/2b VI, 1/2b XVII, 4b VI, and 4b VIII) that caused human infection but were not isolated from the investigated food sources. In the scenario describing the risk group constituted by pregnant women, 70 reported cases, caused by 12 different L. monocytogenes subtypes (including “others”) (Table 1), were attributed to the food sources. The third scenario attributed human cases of listeriosis among the elderly population (≥60 years old), and utilized 381 cases caused by 20 types (including “others”) (Table 1).
Adaptation of the Hald Salmonella Bayesian risk attribution model
The model developed by Hald and colleagues compares the number of sporadic human cases of salmonellosis by different subtypes with their distribution in different food sources, weighted by the amount of food consumed. The full portrayal and discussion of the assumptions and statistics behind the Salmonella Bayesian risk attribution model is described by Hald et al. (2004). The principle of our adapted model is to compare the number of human sporadic cases caused by different L. monocytogenes subtypes with the prevalence of the subtypes isolated from different 13 food sources. The differences in the abilities of the L. monocytogenes subtypes to cause human disease (qi ) and of the food sources to act as a vehicle of infection (aj ) are accounted for by prior distributions. The Hald model also incorporates a food consumption weighting factor. In our adapted model, differences in consumption patterns of the investigated foods in the population were accounted for in aj (as there were no readily available food consumption estimates). Mullner et al. (2009) and Whalstrom et al. (2008) have, however, previously shown that the exclusion of food consumption weights in the model when applied to Campylobacter and Salmonella in New Zealand and Salmonella in Sweden had no major consequences, but noted that the a j became less comparable. For example, in the adapted model a high a j could reflect a high exposure to the food source and not necessarily a high ability of the individual food source to act as a vehicle for disease.
Posterior distributions for the qi
and a
j
factors were estimated by fitting the adapted model to the observed number of cases per L. monocytogenes subtype using a Markov Chain Monte Carlo simulation. The equation used to estimate the number of human cases per food source and L. monocytogenes subtype was defined as follows:
where λji is the expected number of cases per year of type i from source j, pji is the prevalence of subtype i in source j, qi is the subtype-related factor for subtype i, and aj is the food-source-related factor for source j.
The model used the assumptions that all L. monocytogenes serotypes have different qi , and AFLP groups within the same serotypes were assumed to have the same qi. As the qi values are all relative, we fixed the q prior estimate for serotype 1/2a as 1. All other q estimates are relative to this one. Additionally for the pregnant-associated cases scenario, the qi prior distribution for subtype 4b V was defined as an independent prior distribution. The assumption was based on the evidence of a higher likelihood of infection in pregnant women with subtype 4b V (Gillespie and McLauchlin, 2007). No similarities between the aj for each source were assumed.
The model was set to calculate the expected number of cases in each risk group per L. monocytogenes subtype (λji ) according to the above equation. The observed data or number of human cases of type i was then linked with the prior distribution by assuming that the observed cases per L. monocytogenes subtype were Poisson distributed with a parameter value equal to the expected number of cases. The model was set up in the WinBUGS software (Gilks et al., 1994). Five independent Markov chains of 20,000 iterations each were run, and convergence was monitored as described by Gelman and Rubin (1992) and Brooks and Gelman (1998).
Results and Discussion
Adaptation of the Hald et al. (2004) model to quantify the contribution of ready-to-eat food sources to sporadic cases of listeriosis in England and Wales presented a valid means to assess the relative risk from different foods, the results of which are presented in Table 2. For the overall population, the risk model for L. monocytogenes attributed 551 human cases (97.7%), a close match to the observed number of 564 cases; 13 cases (2.3%) could not be associated with any of the food sources. The major sources of infection were multicomponent foods (23.0%), finfish (16.8%), and beef products (15.3%). Similarly in the over-60s population group, the major sources of infection were found to be multicomponent foods (22.0%), finfish (14.7%), and beef (13.6%). Consumption of multicomponent foods—particularly, supplied prepacked sandwiches in hospitals—has been shown to be associated with recent outbreaks of listeriosis in England and Wales (Little et al., 2007; HPA, 2008). However, in the pregnancy-associated cases group, beef (12.3%), milk and milk products (11.8%), and finfish (11.2%) were ranked as important major sources of infection. Multicomponent foods (i.e., sandwiches), sliced meats such as beef, fish, and milk and milk products are considered high-risk foods with regard to L. monocytogenes and thus listeriosis as they have potential for contamination with this pathogen, support its growth to high numbers, can be sold with a long shelf-life under refrigerated conditions, and are consumed as a ready-to-eat food product (Sim et al., 2002; Little et al., 2007, 2009; ACMSF, 2009; HPA, 2008; Wagner and McLauchlin, 2008).
SD, standard deviation; CI, Bayesian credibility interval.
Although the risk of listeriosis is higher when the food is contaminated with high levels of the organism (McLauchlin et al., 2004; EFSA, 2007), the infectious dose of the pathogen is also dependent on the type of food product, strain virulence, and host susceptibility; therefore, relatively lower doses may still cause infection in high-risk populations (McLauchlin et al., 2004). The food-source-related factor (aj ) in the model may account for characteristics of the food item that influence its ability to act as a vehicle for exposure to the pathogen and infection (e.g., general differences in the pathogen load, food characteristics influencing growth behavior, or preparation procedures), and/or food consumption patterns. The highest value for the food-source-related factor (aj ) in the overall population and in both risk population groups was found for “other red meats,” which include meats generally on the market from delicatessen stores (overall population 1.4, 95% Bayesian credibility intervals [CI] 0.04–5.0; pregnancy-associated cases 0.5, 95% CI 0.01–1.7; elderly cases 1.2, 95% CI 0.03–4.3) (Fig. 1).
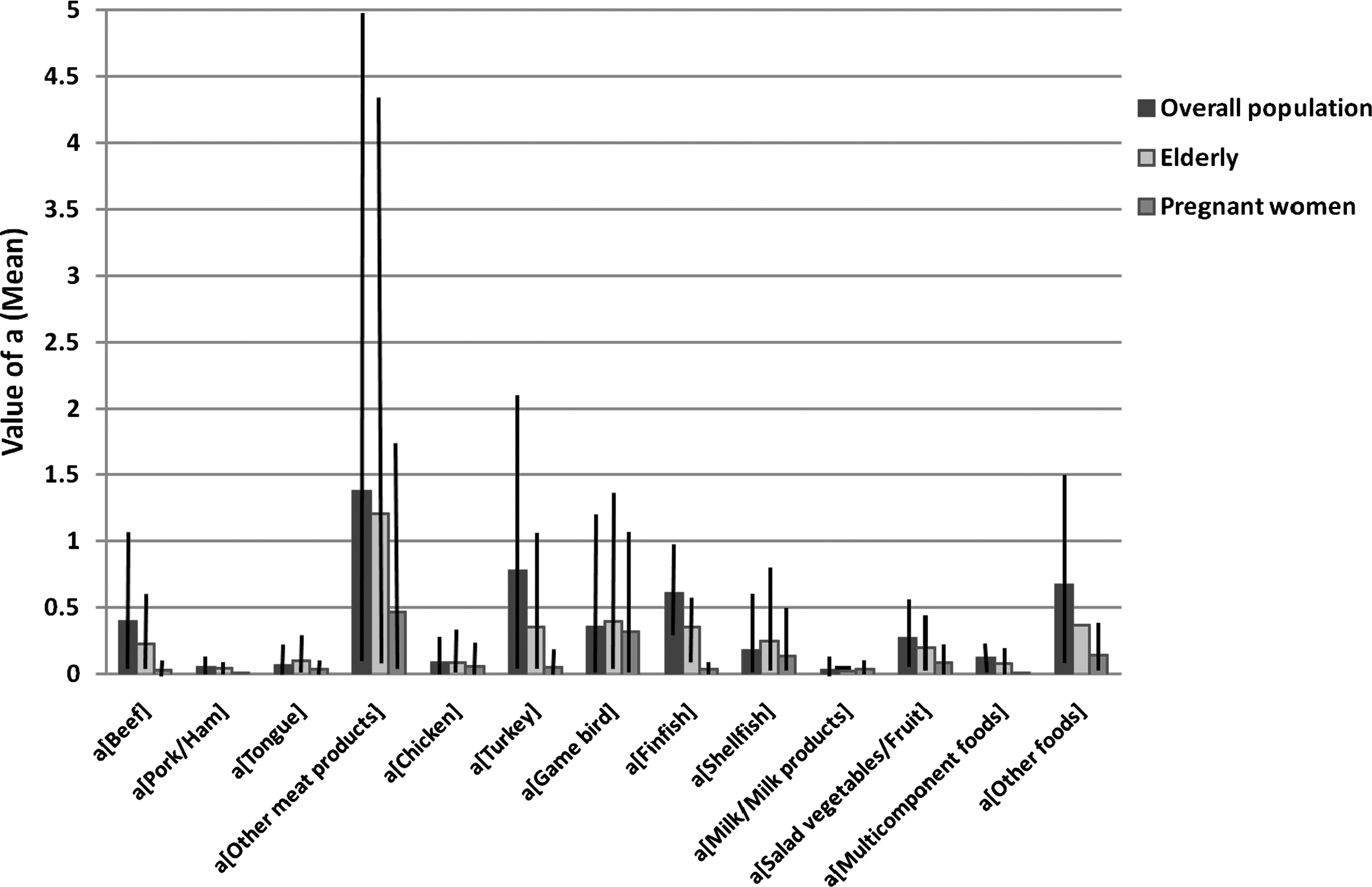
Estimated values and 95% credibility intervals of the ready-to-eat food-source-related factors (aj ).
Meats, including delicatessen meats and pates, have been shown to be important sources of L. monocytogenes in the United Kingdom and elsewhere (Lianou and Sofos, 2007; Gormley et al., 2009; Little et al., 2009). Ready-to-eat food may be contaminated at point of consumption because contamination was not eliminated entirely earlier in the production chain or as a result of postprocess cross-contamination. The U.S. microbiological risk assessment categorized delicatessen meats at the highest level of risk of causing serious illness and death associated with consumption of ready-to-eat foods potentially contaminated with L. monocytogenes, on both a serving and per annum basis (FDA, 2003). Continuous efforts should be made to improve food safety by adequate cooking and appropriate hygienic measures to avoid contamination, and through use of appropriate refrigeration temperatures to prevent growth of L. monocytogenes in these products.
The subtype-related factor (qi ) represents differences in the survivability of the L. monocytogenes subtypes along the food chain, and differences in their virulence and pathogenicity to humans. The estimated values for the L. monocytogenes subtype-related factors (qi ) suggest that the ability of serotype 4b to survive food processing and/or cause disease in the overall population, pregnancy-associated cases, and the elderly group is higher than that of other serotypes (Fig. 2). Moreover, in the pregnancy-associated group, subtype 4b V was estimated to have a higher ability to cause disease; the estimated qi value for this subtype was 63.9 (95% CI 24.6–147.7); the remaining AFLP types within serotype 4b were estimated to have a qi value of 3.3 (95% CI 1.7–5.8), followed by types 1/2b (qi = 1.1, 95% CI 0.3–2.6) and 1/2c (qi = 0.4, 95% CI 0.04–1.1) (Fig. 2). In concordance with these results, the L. monocytogenes serotypes most often causing infection in England and Wales from 2000 to 2008 are 4b (47%), 1/2a (18%), and 1/2b (8%) (HPA, unpublished data), and among pregnancy-associated cases subtype 4b V is predominant (Gillespie and McLauchlin, 2007).
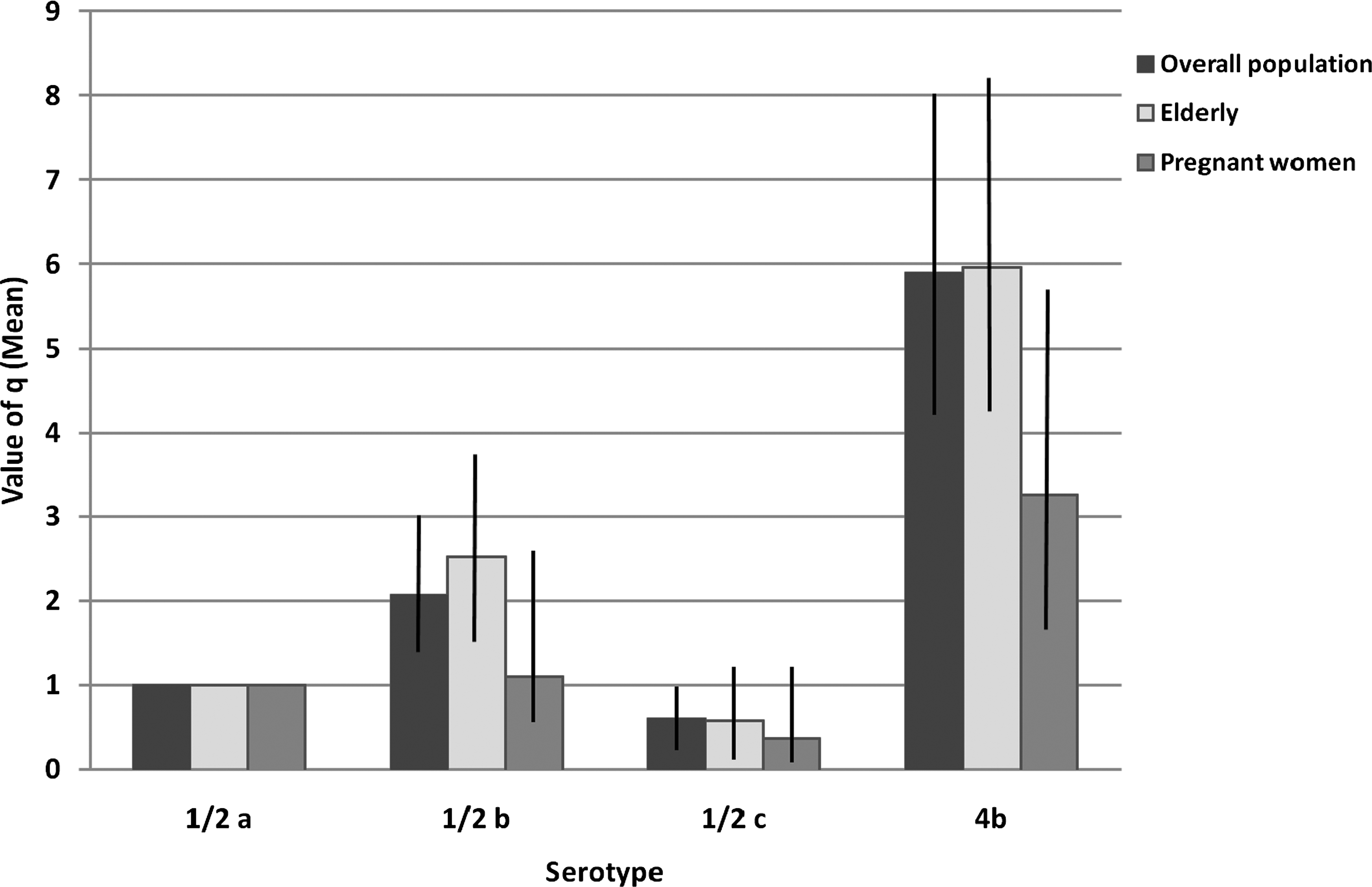
Estimated values and 95% credibility intervals of the Listeria monocytogenes serotype–related factors (q). As the qi values are all relative, the q prior estimate for serotype 1/2a was fixed as 1.
Although monitoring of convergence of the adapted model provided satisfactory results, our risk attribution results presented wide 95% CI. The wide CIs may reflect the epidemiology of L. monocytogenes and the resulting uncertainty on dose response. Dose–response relationships are not well understood for human L. monocytogenes infection. These relationships comprise three major components, each with major uncertainties. The three components are the environment (the food matrix and storage conditions that allow contaminating Listeria to grow to hazardous levels), the pathogen (virulence), and the host (susceptibility and immune status) (McLauchlin et al., 2004). The relative contributions of host and environmental factors in acquiring listeriosis require further study.
Another limitation of our source attribution model was the small size of the dataset with 564 human cases compared with 41,264 Salmonella cases from England and Wales used in the Hald model (Gordon L. Nichols, HPA, pers. comm.). The original Hald Salmonella model itself also utilized a greater number of cases (3268). A similar observation in CIs was also noted in the New Zealand adaptation of the Hald model to Campylobacter where 481 cases were included (Mullner et al., 2009). Increasing the number of Listeria cases in the model may improve precision of the estimates, but compared to Campylobacter and Salmonella in England and Wales, listeriosis is a rare disease with currently around 200 cases reported per annum. The food isolate data included in the model were obtained from food surveys and investigations carried out during 2004–2007. It is conceivable that there could be some foods that contribute a risk for listeriosis which are not represented in this dataset and whose effect will be underestimated as a result. The rationale for the development of a European surveillance network and community food surveys for listeriosis (Denny and McLauchlin, 2008; EFSA, 2009) would, however, present an opportunity to collate pan European data on listeriosis cases, prevalence and levels of L. monocytogenes in different foods, and on L. monocytogenes subtypes both from cases and food sources that could be analyzed using this modified Hald model. Such an approach could provide an improved estimate of the burden of disease and the presence of this pathogen in the food chain.
Conclusions
The modified Hald model for L. monocytogenes provides a valid and useful approach for the attribution of the burden of listeriosis to the specific food sources, and for the prioritization of effective food safety interventions. Further emphasis needs to be given to the reduction of L. monocytogenes in high-risk foods, such as multicomponent foods (prepacked sandwiches and prepacked mixed vegetable salads), which are consumed without any further treatment. High-quality ingredients, hygienic manufacture, appropriate shelf life, and correct refrigerated storage are critical to minimize the potential for L. monocytogenes to be present at the point of consumption at levels hazardous to health. Although listeriosis continues to occur in association with pregnancy, it is now predominantly an infection of the older population. Intervention measures including dietary advice were previously predominantly targeted toward the pregnant woman. However, because of the change in the age distribution of cases, together with a demographic shift in the population as a whole, intervention measures now will therefore be most effective when targeted toward the elderly population.
Footnotes
Acknowledgments
This work was supported in part by a grant from the Med-Vet-Net Short Term Mission/Scientific Exchanges. Med-Vet-Net is a European Network of Excellence for Zoonoses research, working for control and prevention of zoonoses and foodborne diseases. The authors thank Tine Hald, Technical University of Denmark, from Workpackage 28 in Med-Vet-Net for support.
Disclosure Statement
No competing financial interests exist.