
Abstract
Anisakis simplex is a parasite that, if present in uncooked and contaminated saltwater fish, can invade the human gut. Two different clinical situations are recognized: the first, known as a gastrointestinal disease, varying from an asymptomatic episode to vomiting and diarrhea, and the second, classified as an adverse reaction to food, characterized by a wide spectrum of allergic reactions like rhinitis, conjunctivitis, or even anaphylaxis causing hypotension and/or shock. The intestinal epithelium, the major defense system against external molecules, represents an open gate for toxins and allergens if its protective function is compromised. Previous data have demonstrated a strict relationship between an altered intestinal permeability (I.P.) and worsening of the clinical manifestations in patients with adverse reactions to the food. In this article we evaluated the sensitization to A. simplex among patients who referred clinical symptoms of allergy. All subjects underwent commonly used alimentary skin prick test for food allergens, to which Ani s1, an A. simplex allergen, was added. In addition, in A. simplex–sensitized subjects, I.P. was determined upon their enrolment to the study (time 0) and after 6 months of consuming a raw fish-free diet (time 6). Five hundred and forty subjects were screened, and 170 had a positive skin prick test, 87 (51.2%) of whom were positive to Ani s1. Increased I.P. was evidenced in A. simplex–sensitized subjects with worse clinical symptoms, which receded after 6 months' elimination of raw seafood. With our data we demonstrated that the alimentary habit to eat raw fish represents a high risk for the integrity of the intestinal mucosa, and we suggest that this pathological situation may constitute an ideal, under-estimated, open gate for molecules that predispose to other, more important pathologies.
Introduction
Eating raw or undercooked fish (such as sushi and sashimi in Japan, marinated anchovies in Italy, boquerones en vinagre in Spain, and green herring in Germany) is becoming more common all over the word, causing a progressive increase of Anisakis infestation (Gómez et al., 1998; Purello-D'Ambrosio et al., 2000). Between the 1960s and 1997 in Japan, about 32,300 cases of anisakiasis were recorded, representing more than 90% of the cases recorded in all countries (Audicana and Kennedy, 2008); for this reason, this parasitic disease is considered endemic in Japan. The remaining 10% of the cases is distributed among the Netherlands, Germany, France, Spain, and Italy.
The diagnosis of anisakiasis is obtained through anamnestic data and needs to be considered especially in patients presenting with abdominal pain who had consumed raw or undercooked seafood in the past 72 hours. Two different clinical situations of anisakiasis are recognized: The patient presents with gastrointestinal symptoms that may vary from a mild gastroenteritis to sharp abdominal pain, vomiting, and diarrhea, corresponding to acute abdominal syndrome (Pellegrini et al., 2005). The clinical manifestation is mainly determined by IgE-mediated reactions (Ventura et al., 2008), whereby patients, sensitized by previous contact with A. simplex antigens, present allergic reactions like rhinitis, asthma, or even anaphylaxis (Del Pozo et al., 1997; Daschner et al., 1998; Domínguez Ortega et al., 2000; Audicana et al., 2002; Daschner and Pascual, 2005; Barbuzza et al., 2009). Usually it is diagnosed by skin prick test (SPT) that includes Ani s1 allergen (López Peñas et al., 2000), and serum-specific IgE determination against Ani s1 (radioallergosorbent tests) (Arilla et al., 2008).
Of particular interest are the data reported by Armentia et al. (2006), who referred that subjects who are sensitive for A. simplex had allergic symptoms after the consumption of chicken meat. They hypothesized that sensitization to A. simplex might be related to the presence of raw fishmeal in the chicken diet. Indeed, A. simplex–sensitized subjects who consumed chicken meat fed only with cereals did not refer allergic symptoms.
In various countries, specific studies have been performed to detect the relevance of anisakiasis, testing specific IgE against A. simplex. In Japan it has been shown that specific IgE against A. simplex is present in 33% of the patients with atopic dermatitis, 75% of the patients with urticaria, and 10% of the healthy control subjects (Lindqvist et al., 1993).
In Spain studies carried out on a healthy population, evaluating the prevalence of specific IgE antibodies against Ani s1, have reported conflicting data (elevated IgE serum levels ranging from 6.6% to 27.5% of subjects) (Del Pozo et al., 1996; Fernandez et al., 1997; García et al., 1997; Audicana et al., 2000; Purello-D'ambrosio et al., 2000).
Buendia and coworkers referred the presence of A. simplex–specific IgE in 23% of the healthy control subjects, in 36% of the patients with mixed symptoms like urticaria and/or angioedema, and in 56% of children with elevated total serum IgE (Buendia, 1997).
Food represents the major cause of intestinal antigenic challenge during lifetime. The intestinal epithelium with a healthy, full-grown mucosa and intact epithelial tight junctions represents the major defense organ against external antigens, toxins, and macromolecules that reach the intestinal lumen. When this defensive system is compromised, the intestinal permeability (I.P.) becomes altered (Ventura et al., 2006).
In the early 1980s, Andre and collaborators (1987), focusing on I.P. evaluation in subjects reporting IgE-mediated reactions, reported an increase of I.P. after food allergen ingestion. We recently demonstrated that patients with allergic reactions to food manifest an altered I.P. (Ventura et al., 2006).
To our knowledge, sporadic data are present in literature referring sensitization to A. simplex in Italy. Mainly the authors refer A. simplex clinical cases accidentally observed in the operative room or during gastrointestinal endoscopy (Montalto et al., 2005; Foti et al., 2006; Biondi et al., 2008), and probably some cases may not have been diagnosed because the infestation may have been asymptomatic or had healed spontaneously. For this reasons we believe that it could be important to determine the prevalence of anisakiasis in a region of Italy where the habit to eat raw seafood is common.
In this article we report the data obtained by evaluating patients with clinical symptoms of adverse reaction to food. A. simplex sensitization was determined by alimentary SPT and, when possible, serum-specific IgE levels were measured (López Peñas et al., 2000). In addition, the degree of I.P. in A. simplex–sensitized patients was determined before (time 0) and after a 6-month period of raw fish-free diet (time 6).
Materials and Methods
Subjects and study protocol
The study was carried out on 540 subjects who attended the Health Centre of the Allergy Department of the University of Bari referring an adverse reaction to food. These patients were tested with common alimentary SPT to which Ani s1 (Alk-Abellò, Horshomlm, Denmark) was added. Ani s1 is a major allergen of A. simplex and indicates nematode infection and is useful for the diagnosis of Anisakiasis (Moneo et al., 2000; Valls et al., 2003; Kobayashi et al., 2008). Specific IgE serum levels determination, when possible, were evaluated (Del Rey Moreno et al., 2006; Arilla et al., 2008). The medical history of the allergic symptoms, the correlation with the consumption of raw or undercooked seafood, the quantity of seafood ingested, and the time between ingestion and symptom onset were examined.
Fifty healthy volunteers, matched for age and sex, selected from the medical staff (19 men and 31 women; mean age 40 years; range 18–70 years), with no symptoms or signs of gastrointestinal disease, for at least 2 weeks, were included as control. All subjects revealed negative allergic tests to food (alimentary SPT) and did not use raw or undercooked fish in their diet.
The study protocol was approved by the Ethics Committee of the Azienda Ospedaliero-Universitaria “Policlinico Hospital” of Bari. All the participants provided their written informed consent.
As stated by the European Academy of Allergology and Clinical Immunology position paper on IgE-mediated food allergy, the diagnosis of food allergy was confirmed by positive SPT (European Academy of Allergology and Clinical Immunology, 1989) and by radioallergosorbent tests (Paganelli et al., 1998), which were determined in patients upon their enrolment to the study (time 0). In Ani s1+ SPT patients, I.P. was determined at the beginning of the study (time 0) and, when I.P. was altered, after 6 months of raw or undercooked fish-free diet (time 6). Further, all subjects from the control group were tested for I.P. at the time of their enrolment to the study (time 0).
Allergological tests
Skin prick test
A positive control (histamine, 10 mg/L) and a negative control (glycerinated saline) with a panel of food allergens (tuna, salmon, mackerel, sardine, shrimp, and octopus), inhalants (Dermatophagoides pteronyssinus, Acarus siro, Lepidoglyphus destructor, Tyrophagus putrescentia), and A. simplex, Ani s1, allergen (Alk-Abellò) were tested and interpreted according to the European Academy of Allergology and Clinical Immunology Subcommittee on Allergen Standardization and Skin test. If the diameter of the reaction was more than 3 mm than the one provoked by the negative control, the response was considered positive. SPT, similarly to specific IgE serum level in vitro determination, is considered a highly sensitive method for the diagnosis of A. simplex sensitization (Lorenzo et al., 2000).
Radioallergosorbent tests
UniCAP system (Pharmacia, Uppsala, Sweden) was used to detect specific IgE serum levels against A. simplex, considering positive any value higher than 0.35 kUA/L (Del Rey Moreno et al., 2006; Arilla et al., 2008).
I.P. test
I.P. has been determined as previously described in literature (Generoso et al., 2003; Ventura et al., 2006). Briefly, the subjects fasted overnight and then ingested 200 mL of tap water containing 2 g of Mannitol (Ma) and 5 g of Lactulose (La). Urine samples were collected before ingestion of the probes to ensure their endogenous absence, and during the following 5 hours. Anion-exchange chromatography on each urine sample was performed, the percentage of ingested La and Ma evaluated, and their ratio (La/Ma) calculated. Each La/Ma value has been multiplied by 100 (detected La/Ma value ×100). Each sample was analyzed three times.
Statistical analysis
The data of I.P. are been reported as arithmetic mean ±standard deviation (AM ± SD). Student's t-test for unpaired values was used to compare the data obtained from the different groups of subjects. The correlation between the severity of the symptoms and the La/Ma ratio levels was evaluated by the rank correlation test for nonparametric data (Spearman test). A p < 0.05 was considered statistically significant.
Results
Table 1 reports the alimentary SPT data. Five hundred and forty patients were screened, and the test result of 370 patients was negative (SPT−). Among the 170 STP-positive subjects (SPT+), the result of 87 (51.2%) was Ani s1+ and 83 (48.8%) Ani s1−.
Among the 170 alimentary STP+ patients, 87 resulted Ani s1 sensitized.
Table 2 reports the detailed allergen positivity of 87 Ani s1+ SPT patients. Sixty three subjects revealed the sensitization only to Ani s1, whereas 24 patients resulted sensitized by other food-derived allergens besides Ani s1. Fifteen, among the 24 multifood-derived allergen SPT+ patients, showed sensitization to seafood-derived allergens from intermediates paratenic hosts of A. simplex life cycle.
Among the 87 Ani s1-sensitized patients, 78 showed SPT positive to Ani s1 alone or to other seafood-derived allergens, beside Ani s1.
SPT, skin prick test.
In 38 of 87 A. simplex–sensitized patients specific IgE were evaluated in serum samples drawn at the time of their enrolment (time 0). In 21 subjects (55%) high levels of Ani s1–specific IgE (28.01 ± 7.84 kUA/L) were detected; the remaining 17 patients showed normal Ani s1–specific IgE values (0.15 ± 0.08 kUA/L).
Table 3 shows the characteristics and the clinical symptoms of Ani s1+ SPT patients. The mean age of patients was 44 years (range 14–75 years); male patients were almost half of the female patients. The clinical manifestations of these patients range from simple pruritus (Grade 1 group) to angioedema and anaphylaxis (Grade 4 group).
Figure 1 reports the age distribution of the 87 A. simplex–sensitized patients collected by decades. Most of the subjects aged 30–50 years, 6.89% aged less than 20 years, and more than 35% were older than 50 years.
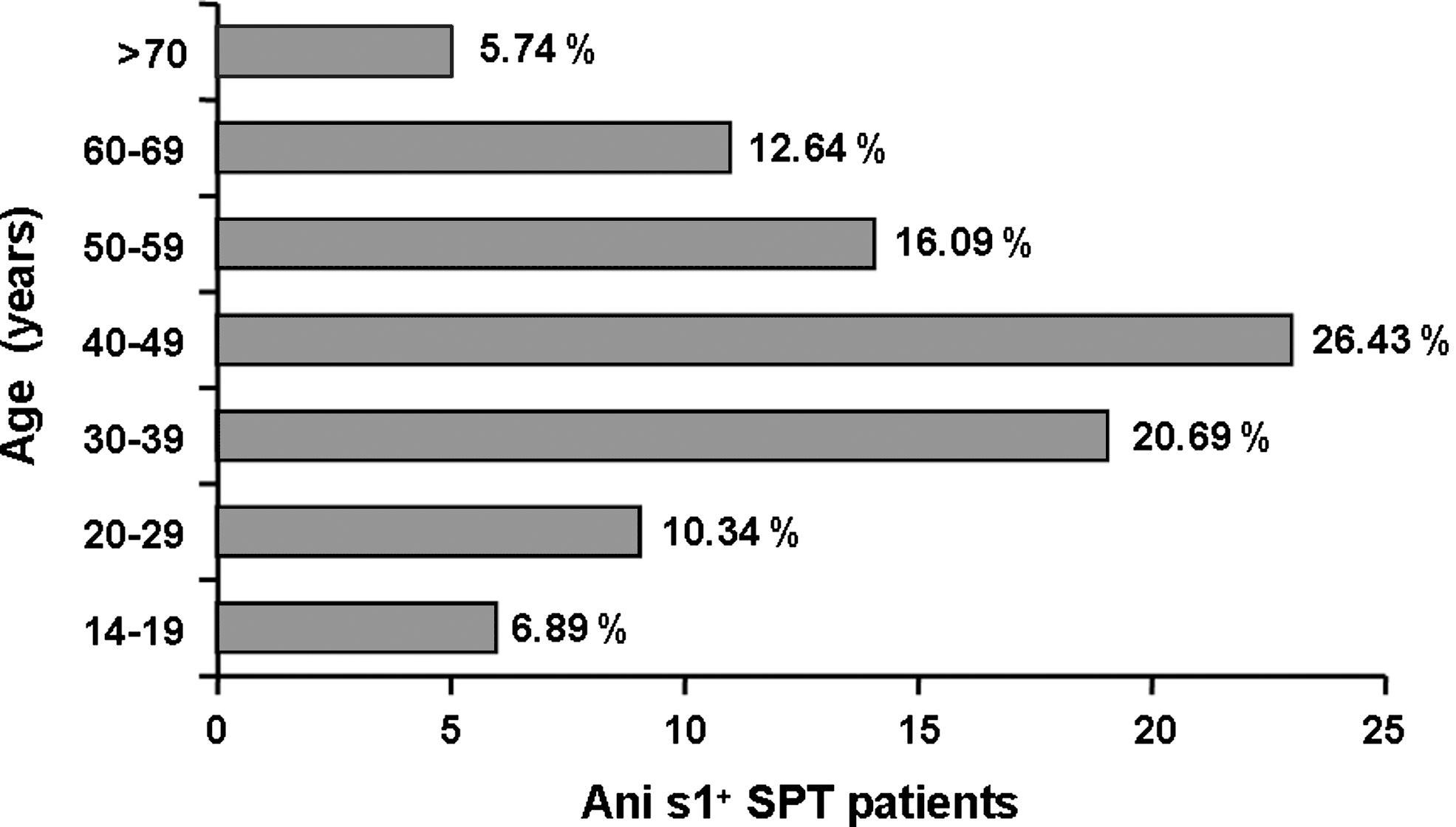
Anisakis simplex–sensitized patients. About 87 patients (age range 14 to 75 years) positive to Ani s1 antigen were grouped and divided by decades. The most representative class was between 40 and 50 years old even if 6.89% was younger than 19 years and more than 33% older than 50.
Figure 2 reports La/Ma ratio determined in control subjects and A. simplex–sensitized patients divided into four groups following the clinical manifestations as referred at time 0 and reported in Table 1. I.P. levels of normal control subjects (La/Ma = 1.73 ± 1.12, AM ± SD) were similar to that already present in the literature (Generoso et al., 2003; Ventura et al., 2006). The data from the A. simplex–sensitized patients, stratified according to the clinical symptoms (Table 3), revealed a progressive increase in the La/Ma ratio, in the groups 1 and 2 (La/Ma: 2.5 ± 0.9 and 2.43 ± 0.88, respectively, AM ± SD), not statistically different when compared to the control group value; on the other hand, I.P. from people of groups 3 and 4 was found to be statistically higher (AM ± SD) when compared to normal control subjects (for group 3: La/Ma = 5.66 ± 1.06, p = 2.6 × 10−9, normal group vs. group 3; for group 4: La/Ma = 10.83 ± 8.6, p = 1.63 × 10−7, normal group vs. group 4).
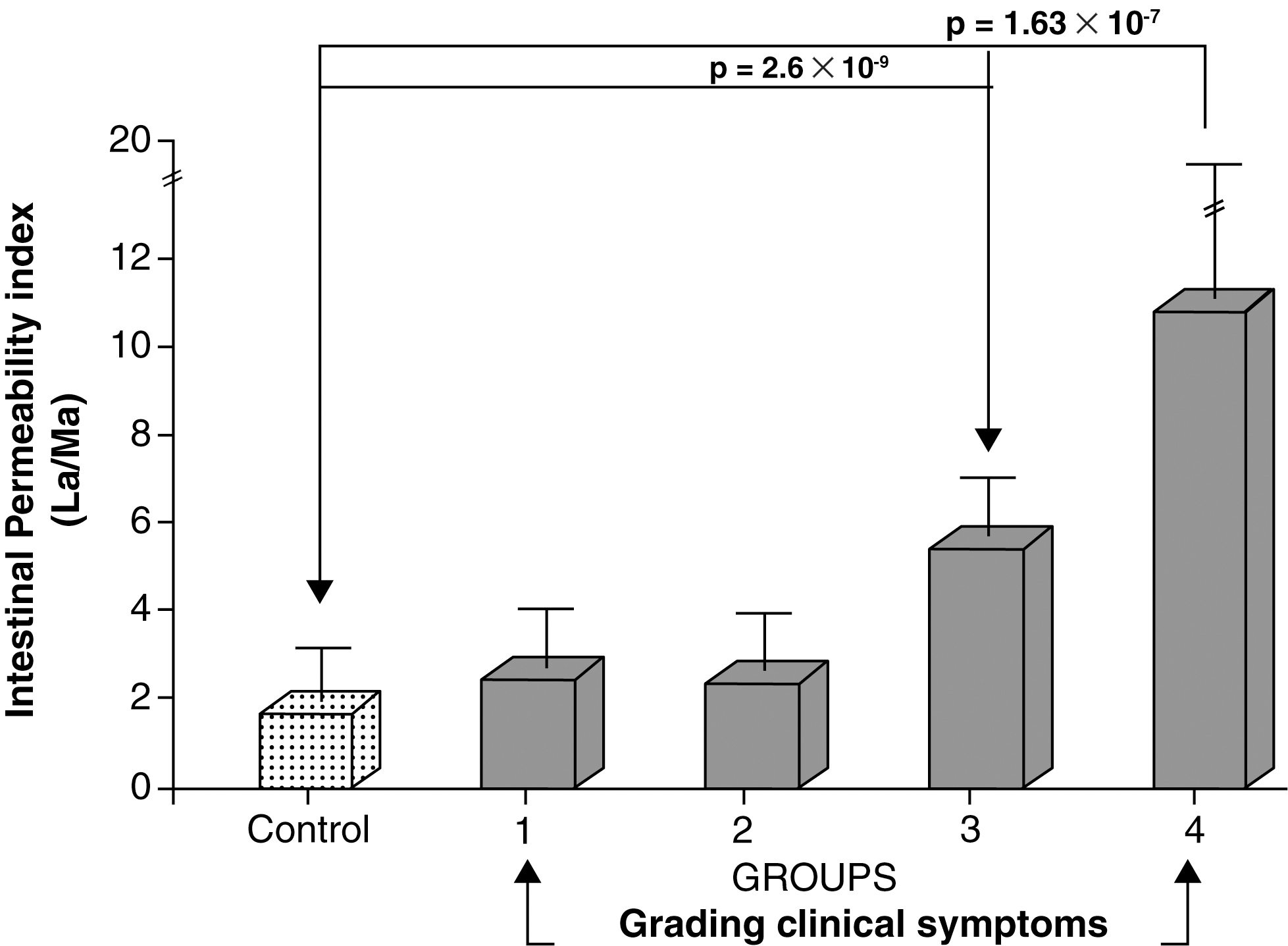
Levels of La/Ma urinary excretion of A. simplex–sensitized patients grouped by severity of clinical symptoms. The intestinal permeability (I.P.) of A. simplex–sensitized patients grouped according to the clinical symptoms was compared to normal control group subjects. A significant alteration of La/Ma excretion ratio was detected in those patients who referred generalized urticaria, diarrhea, asthma (group 3), or angioedema and anaphylaxis (group 4).
Figure 3 reports the correlation analysis between I.P. data from A. simplex–sensitized patients and the severity of the clinical symptoms referred by patients at time 0. The significant relationship (ρ = 0.7069) between these two parameters demonstrates that worse allergic symptoms are strictly related to higher I.P. levels.
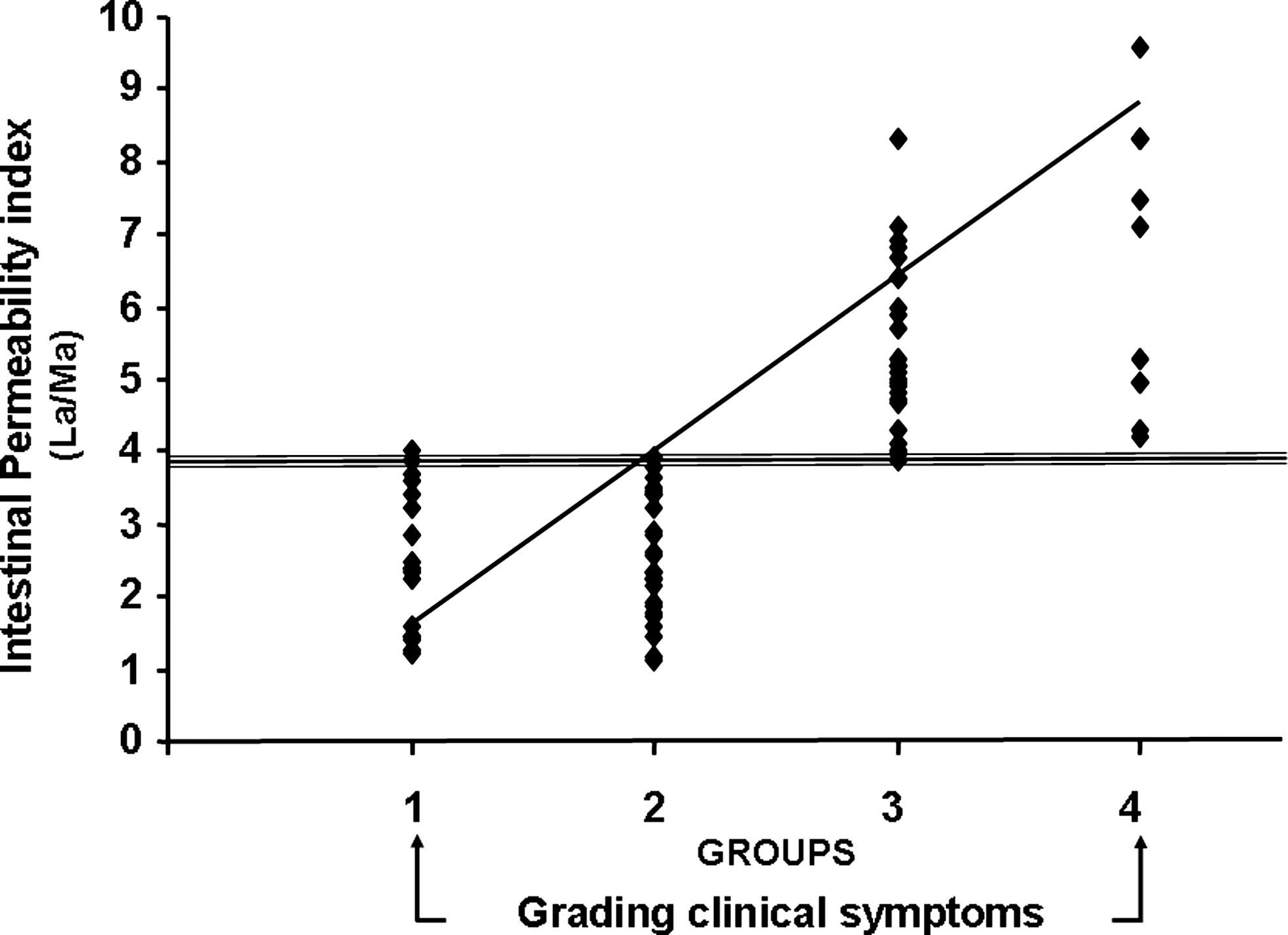
Correlation between La/Ma urinary excretion of A. simplex–sensitized patients and clinical symptoms. The rank correlation test for nonparametric data applied to the La/Ma urinary ratio from A. simplex–sensitized patients shown to be strictly related to the severity of the clinical symptoms referred by the patients.
In Figure 4, I.P. levels of A. simplex–sensitized subjects, evaluated at time 0 and after a 6-month period of raw fish-free diet (time 6), are reported. The data of patients from groups 3 and 4 were contemporary considered since, at time 0, La/Ma values were significantly higher than normal control subjects (Fig. 2). Taken together, the data obtained at time 0 (groups 3 and 4: La/Ma = 7.3 ± 5.4; AM ± SD) confirmed the statistical difference (p = 1.5 × 10−7), as compared to normal control subjects (La/Ma = 1.73 ± 1.12; AM ± SD). I.P. evaluated in the same patients at time 6 revealed a statistically significant (p = 6.5 × 10−8) reduction (La/Ma = 1.81 ± 0.99; AM ± SD).
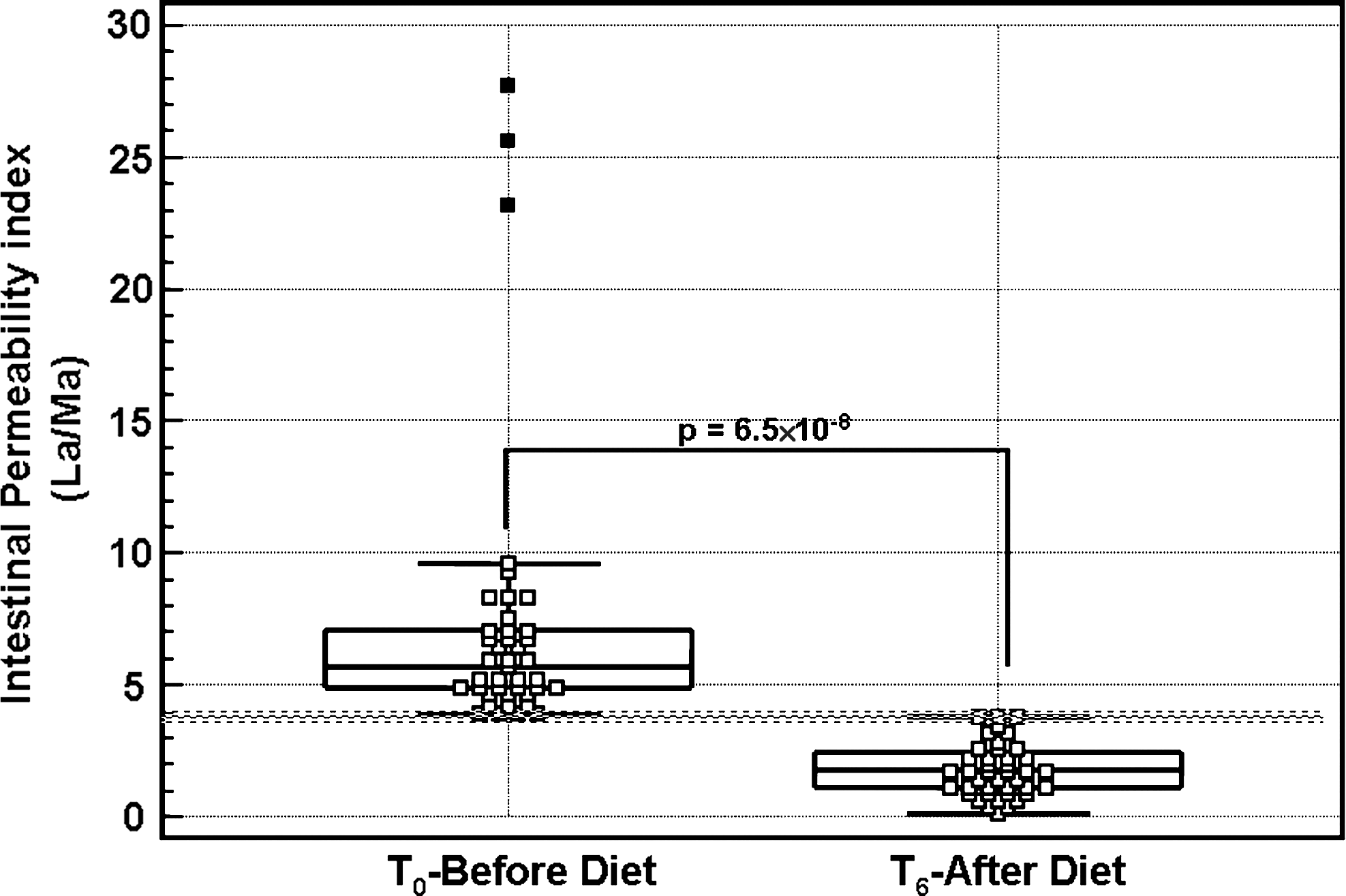
Effect of raw-fish-free diet on La/Ma urinary excretion of A. simplex–sensitized patients. I.P. was measured after 6 months of raw-fish-free diet (time 6) in A. simplex–sensitized patients who presented altered La/Ma urinary excretion at time 0. A statistically significant reduction was observed, reaching the normal value, showing a comeback in each patient to the I.P. normality (hatched line).
Discussion
In this article we (1) report the degree of A. simplex sensitization evaluated in a population of Italy, where the use of raw or undercooked saltwater fish is frequent, and (2) demonstrate that A. simplex–sensitized subjects have altered I.P. integrity, which returns to normal values when seafood is not included in their diet.
The present analysis has been conducted evaluating the commonly used allergens for alimentary SPT and Ani s1, the major allergen of A. simplex, an indicator of true nematode infestation and useful for the diagnosis of anisakiasis without cross reactions to other allergens (Moneo et al., 2000; Valls et al., 2003; Kobayashi et al., 2008).
The data reported indicate that 31.5% of the subjects tested by alimentary STP resulted positive; among these, 51.2% were positive to Ani s1 (Table 1). More dramatic are the data reporting that 63 (72.4%) of A. simplex–sensitized patients showed SPT positivity to Ani s1 allergen alone (Table 2).
Of interest are the data obtained by analyzing the A. simplex–sensitized patients grouped into decades: more than one-third of the subjects were older than 50 years and, when questioned, did not know to be allergic to the A. simplex. It is known that A. simplex sensitization increases with age in patients who consume frequently raw fish, but in our analysis we believe that such patients in previous alimentary SPT tests had been diagnosed as “not allergic,” even though the anamnestic clinical symptoms of allergy (pruritus, urticaria, and/or rhinitis) suggested for an allergic syndrome. We believe that the presence of Ani s1 antigen in the SPT performed in the present study, and absent in the previous examinations, gave us the opportunity to reveal, for such patients, the cause of their clinical symptoms. In addition with our data we indirectly demonstrated that anisakiasis is, probably, an under-estimated infection.
As described in Figure 1, young people were also present in the study, which is not surprising, considering the habit to consume raw or undercooked seafood in this part of Italy.
A. simplex–sensitized patients were also evaluated for intestinal mucosa integrity (Generoso et al., 2003; Ventura et al., 2006) at their enrolment to the study (time 0). Only the subjects referring worse clinical symptoms (Table 3, groups 3 and 4) showed elevated I.P. values (Figs. 2 and 3). As already reported in literature, other forms of adverse reactions to food (Ventura et al., 2006) showed a significant correlation between the severity of the clinical symptoms and the La/Ma urinary levels (Fig. 3). I.P. levels investigated in the same subjects after 6 months of a raw or undercooked saltwater fish exclusion from the diet (time 6) revealed a statistically significant reduction of La/Ma urinary ratio, reaching the normal-group values (Fig. 4). This datum seems to be in contrast with the demonstrated thermostability of A. simplex allergens (Audicana and Kennedy, 2008). Data from literature demonstrated that Ani s1 allergen, in particular, seems to be highly resistant to heat (Caballero and Moneo, 2004; Shimakura et al., 2004) and that an A. simplex homologous allergen, present in Ascaris, maintains its allergenicity even after high-temperature denaturation and consequent cooling (Christie et al., 1993; Kennedy et al., 1995; Xia et al., 2000). Many could be the interpretations of such apparent discordance with the literature: first of all, it is important to point out that most of the subjects who underwent I.P. determination after the diet referred a total elimination of seafood from their diet. On the other hand, those subjects who did eat seafood cooked it for more than 10 minutes at 60°C. It should be point out that I.P. became normal when the clinical symptoms were not present any longer, as referred by the patients, suggesting that the recovery of I.P. may be related to and determined by the same physiological events still not totally investigated and, probably more important, the proteins responsible for the allergenic sensitizations could be different of those which regulate the intestinal integrity.
In conclusion, our findings strongly support the necessity to eliminate raw or undercooked saltwater food from the diet, which, besides inducing allergenic reactions, may also determine a leak in the intestinal mucosa, which often is unrecognized and it can predispose to other, more important pathologies.
Disclosure Statement
No competing financial interests exist.