
Abstract
More than 100 foodborne salmonellosis outbreaks occur each year in the United States. Contaminated food preparation equipment is implicated in approximately 32% of Salmonella outbreaks with a known source. In April 2009, we investigated reported Salmonella infections at a camp in New Hampshire. Camp attendees were contacted to complete a standard questionnaire. The questionnaire asked about foods eaten while at the camp, symptoms of gastrointestinal illness, visits to healthcare providers, and specimen submission for pathogen testing. Laboratory and environmental investigations were conducted, including testing of foods and food preparation equipment. A total of 133 ill persons, including 47 laboratory-confirmed Salmonella Enteritidis infections, were identified during this investigation. A total of 142 (80%) of 178 camp attendees completed a standard questionnaire and 109 cases of gastrointestinal illness and 33 healthy individuals were identified. Statistical analysis of survey data indicated that people who ate pudding were 15 times more likely to become ill with salmonellosis than those who did not eat pudding (risk ratio, 15.2; 95% confidence interval, 2.3–102.3). Salmonella Enteritidis was identified in leftover pudding and in the internal mixing components of the blender used to mix the pudding. All patient, food, and blender isolates exhibited the same pulsed-field gel electrophoresis pattern. This outbreak of Salmonella Enteritidis was caused by a Salmonella-contaminated hand-held immersion blender used to prepare pudding at a camp. A malfunctioning blender shaft seal is suspected to have resulted in contamination of the blender and subsequently pudding prepared using the blender.
Introduction
S
We describe an outbreak of Salmonella Enteritidis infections at a camp in New Hampshire attributed to pudding contaminated by a Salmonella-contaminated hand-held immersion blender. This outbreak investigation is noteworthy in that the outbreak strain of Salmonella was identified in patient, food, and blender isolates; laboratory confirmation of an outbreak's source occurs infrequently in outbreak investigations and a vehicle is implicated in only 37% of reported foodborne outbreaks in the United States (CDC, 2006a). Further, an unlikely food vehicle was implicated as the pudding contained only two ingredients (pasteurized milk and dry pudding mix) and preparation involved little food service worker hand contact. Ultimate implication of the immersion blender required extensive specimen collection and laboratory testing.
Methods
Detection of the outbreak
On April 19, 2009, an emergency room physician called the New Hampshire Department of Health and Human Services (DHHS) to report gastrointestinal illness in three students who had recently returned from a school trip to a camp. The students had stayed at the camp from April 14 to April 17. Initial laboratory testing of stool specimens from ill students at the emergency department indicated infection with Salmonella enterica serogroup D, which was later confirmed at the New Hampshire Public Health Laboratories (PHL) as S. enterica serotype Enteritidis. A second student group from a different school arrived at the camp on April 20 as the outbreak investigation was beginning, and a group of students from a third school arrived on April 22. By the morning of April 24, campers from the second and third school groups were reporting illness. DHHS also learned of gastrointestinal illness in a private nonschool group that stayed at the property from April 17 to April 19 (groups and timeline outlined in Table 1).
Total ill represents total number of persons reported ill by group organizers during the investigation. Not all ill persons were interviewed to assess illness status or to acquire exposure information.
Standardized survey not administered.
N/A, not applicable.
Case finding and cohort study
Confirmed, probable, and suspect case definitions were developed. A confirmed case was defined as vomiting or diarrhea (≥3 loose stools in 24 hours) within 7 days of consuming foods from the camp in a person whose stool tested positive for Salmonella. A probable case was vomiting or diarrhea within 7 days of consuming foods from the camp in a person whose stool was not tested for Salmonella. A suspect case was any gastrointestinal symptoms (such as nausea) without vomiting or diarrhea within 7 days of consuming foods from the camp in a person whose stool was not tested for Salmonella.
Students and staff from three school groups that attended the camp were enrolled in a retrospective cohort study. Contact information for camp attendees was obtained from school nursing staff, and camp attendees were contacted to complete a standard questionnaire approximately 6 days after onset of illness of the first case. The questionnaire asked about more than 70 food items served and other potential exposures while at the camp, symptoms of gastrointestinal illness in the week before and after arrival at the camp, visits to healthcare providers, and specimen submission for pathogen testing. Information from the private group was solicited from the group organizer. A standard questionnaire was not administered to the private group.
Statistical analyses were conducted using SAS (version 9.1; SAS Institute, Cary, NC). Suspect cases were excluded from risk factor analysis. Univariate methods were used to evaluate attack rates of salmonellosis and to calculate risk ratios with corresponding 95% confidence intervals to assess exposures as potential sources of illness. Multivariate methods were not necessary as only one exposure was significant in the univariate analysis.
Environmental investigation
The New Hampshire Food Protection Section (FPS), DHHS epidemiologists, and the New Hampshire Department of Environmental Services (DES) made four visits to the camp to conduct environmental and food service investigations, including collection of environmental and food samples. Two 100-mL drinking water samples were collected by DES and sent to the DES laboratory for microbiologic analysis. Leftover food samples were collected and delivered to the PHL, including shell eggs, unopened vanilla pudding mix, and prepared vanilla pudding. FPS made a final visit to the camp after statistical and laboratory implication of a particular food item to assess food preparation and equipment sanitation processes relevant to the specific food item and to collect environmental swabs, which were delivered to the PHL for analysis.
Laboratory testing
Stool samples were collected from individual students and staff by private healthcare providers and sent to local clinical microbiology laboratories for analysis. Once identified, the Salmonella isolate was forwarded to the respective state public health laboratory for confirmatory testing using standard biochemical tests (CDC, 2006b, 2006c) and pulsed-field gel electrophoresis (PFGE), a molecular technique used to further differentiate Salmonella into strains, using protocols by PulseNet, the national molecular subtyping network for foodborne disease surveillance (Ribot et al., 2006). Stool samples solicited from ill staff members and food service workers were sent directly to the PHL. Leftover food samples, mouse droppings, and environmental swabs were submitted to the PHL. Food samples and environmental swabs were tested for pathogens using standard Food and Drug Administration (FDA) protocols (FDA, 2007). Mouse droppings were tested in the same manner as human stool specimens. The two 100-mL drinking water samples collected were tested for fecal coliforms at the DES laboratory using standard Environmental Protection Agency protocols (EPA, 1998).
An immersion blender was delivered to the PHL for inspection and testing. Upon arrival, one additional swab was collected from the external surfaces of the blender. The blender was then used to mix a 250-mL sterile lactose broth in the laboratory for 2 minutes. The broth was tested for the presence of Salmonella using standard FDA protocols (FDA, 2007) and isolates underwent PFGE (Ribot et al., 2006). To access the internal components of the blender for inspection and environmental swabbing, the blender was dismantled. Material samples and swabs were tested using standard FDA protocols (FDA, 2007). Salmonella isolates identified were typed using standard biochemical tests (CDC, 2006b, 2006c) and PFGE (Ribot et al., 2006).
Results
Case finding and cohort study
A total of 133 ill persons, including 47 laboratory-confirmed Salmonella Enteritidis infections, were identified during the course of this investigation for an approximate overall attack rate of 60% (Table 1). A total of 142 (80%) of 178 persons from the three school groups completed a standard questionnaire. Of those interviewed, 109 cases of gastrointestinal illness (32 confirmed, 57 probable, and 20 suspect) and 33 healthy individuals were identified. The median age of patients was 12 years (range, 11–14 years). Sixty-one (56%) of 109 patients were girls. Patient illness onset dates ranged from April 15 to April 27 (Fig. 1). The median incubation period from the time the implicated food item was served was 42 hours (range, 1–156 hours). Among 109 patients with clinical information, symptoms reported included abdominal cramps (91%), lethargy (88%), fever (80%), headache (77%), nausea (77%), diarrhea (76%), vomiting (42%), and bloody diarrhea (14%). Reported duration of illness ranged from 1 to 10 days (median, 4 days). Forty-seven (43%) patients sought medical care for their illness. There were five hospitalizations and no deaths.

Illness onset date of reported gastrointestinal illnesses (n = 107a), Salmonella outbreak, New Hampshire, 2009. aThe total includes confirmed, probable, and suspect cases that completed the survey with date of illness onset reported; the exact onset date was not known for two cases.
Statistical analysis of survey data indicated that people likely became infected with Salmonella after consuming Salmonella-contaminated pudding. Pudding was served to the school groups on April 15 and April 22. Eighty-seven (85%) of 103 people that ate pudding on either day became ill compared to 1 (6%) of 18 people who did not eat pudding (risk ratio, 15.2; 95% confidence interval, 2.3–102.3), and 87 (98%) of 89 confirmed and probable cases reported eating pudding. Of the two cases that did not report eating pudding, one specifically denied eating pudding and one was unsure. No other exposures were significantly associated with illness. The private group that stayed at the resort had been served a pastry prepared using leftover pudding served to the first school group on April 15. The coordinator of the private group reported that 8 of the 24 people in the group experienced gastrointestinal illness, including two laboratory-confirmed Salmonella infections. Both confirmed cases from this group reported eating the pudding-containing pastry. Exposure information for the remainder of the group was not collected.
Environmental investigation
During the initial visit to the camp, FPS identified two critical violations: evidence of rodent infestation and the dishwasher not sanitizing properly. After the dishwasher's pump was primed, the sanitizer dispensed at the proper concentration. The menu of foods served to the first school group was obtained during this visit. Additional visits were made to the camp to continue environmental and food service investigations. FPS inspectors identified other potential food safety issues such as preparation of many dishes containing raw shell eggs, which were subsequently cooked, but with no documentation of cooking temperatures and hot holding times. Eight food service workers were identified as having prepared foods served to the groups staying at the camp the weeks of April 13 and April 20. Stool specimens for Salmonella testing were requested and provided by all eight food service workers. The resort purchased pasteurized eggs after the first group became ill, which were first used for scrambled eggs served to the second and third school groups. Some rodent feces remained in food storage areas and samples of the droppings were collected.
FPS made a final visit to the camp to ask additional questions and to collect environmental samples after epidemiologic data from the first school group showed a significant association between illness and eating pudding and the sample of leftover prepared pudding grew Salmonella in the laboratory. Food service staff were queried about pudding preparation. Pasteurized milk was added to a pouch of dry pudding mix and then blended using a hand-held immersion blender. The pudding was poured into several large bowls and refrigerated immediately until served. The immersion blender was also used to blend raw shell eggs and soup. The blender was manufactured by a major food equipment manufacturer in the United States and was certified by an independent, not-for-profit organization that offers voluntary certification for food equipment.
The process for cleaning the blender was described by food service staff, who reported that food contact surfaces of the blender were immersed in hot water and run for an unmonitored amount of time, and then immersed in a sanitizing bleach solution and run for an unmonitored amount of time, and then either wiped dry with a cloth or left to air-dry. The blender could not be disassembled for cleaning. The cleaning process was described by staff and not verified through observation or records. FPS obtained a copy of the operation manual for the blender, which recommended a cleaning process whereby the blender is immersed in a washing solution and run for 2 minutes, immersed in clean rinse water and run for 2 minutes, immersed in a sanitizer and run for 2 minutes, and then left to dry. The cleaning process described by staff was not consistent with manufacturer's recommendations as it was missing the washing solution step and the length of run time was not monitored. The blender was purchased approximately 2 years before the outbreak and had been used and cleaned in the same manner since without causing an outbreak. DHHS requested the implicated handheld immersion blender, which was delivered to the PHL for further examination and testing.
Laboratory testing
Forty-seven stool specimens from ill persons tested positive for Salmonella Enteritidis. A total of 47 patient Salmonella isolates were sent to public health laboratories in Maine, Massachusetts, and New Hampshire for PFGE, and all exhibited the JEGX01.0004 first enzyme (XbaI) pattern. Of those, 35 were tested using the second enzyme (BlnI) and all exhibited the JEGA26.0002 pattern.
Stool specimens collected from seven of the eight food service workers were negative for Salmonella and one food service worker's stool tested positive for the outbreak strain of Salmonella. The food service worker became ill during the outbreak around April 27 and reported eating the contaminated pudding before her illness. Additionally, three nonfood service staff members from the camp submitted stool specimens for testing after becoming ill with gastrointestinal illness and the outbreak strain of Salmonella was identified in the stool specimens of all three. These three staff members reported eating the contaminated pudding before illness.
Because initial epidemiologic analysis of survey data implicated pudding as the source of the outbreak, the pudding and shell eggs were tested immediately and all other foods were held untested pending results of the pudding and egg testing. A total of 160 shell eggs collected from the camp were tested for Salmonella, which was not found. Prepared leftover pudding from April 22 tested positive for the same strain of Salmonella identified in the patient specimens. An unopened package of the dry pudding mix was tested and Salmonella was not found. The remaining food specimens were not tested. Salmonella was not found in the mouse droppings collected from the food storage area. No fecal coliform bacteria were identified in the drinking water samples collected by DES.
Salmonella was not found in the four external swabs of kitchen surfaces (outer surface of the immersion blender, outer surface of a floor mixer, outer surface of a juice dispenser, and surface of a cutting board). After the external swab collected on-site of the blender used to mix the contaminated pudding did not detect Salmonella, one additional external swab was collected from the external surfaces of the blender upon arrival in the PHL, which was negative for Salmonella. Sterile lactose broth mixed with the blender in the laboratory yielded the outbreak strain of Salmonella. Once the blender was dismantled (Fig. 2), a crack on the bottom of the plastic motor housing was observed. Dried yellow residue, consistent in appearance with blended egg or dried pudding, was found on the top and bottom of the interior motor housing near the vent holes; the outbreak strain of Salmonella was isolated from a sample of this material. Once the cutting blade shaft seals were removed, dark brown-blackish granular material was found inside the internal shaft seal; the outbreak strain of Salmonella was isolated from a swab of this material and from an approximately 0.5 × 0.5 cm piece of the material. No obvious cracks were observed in the shaft seal.
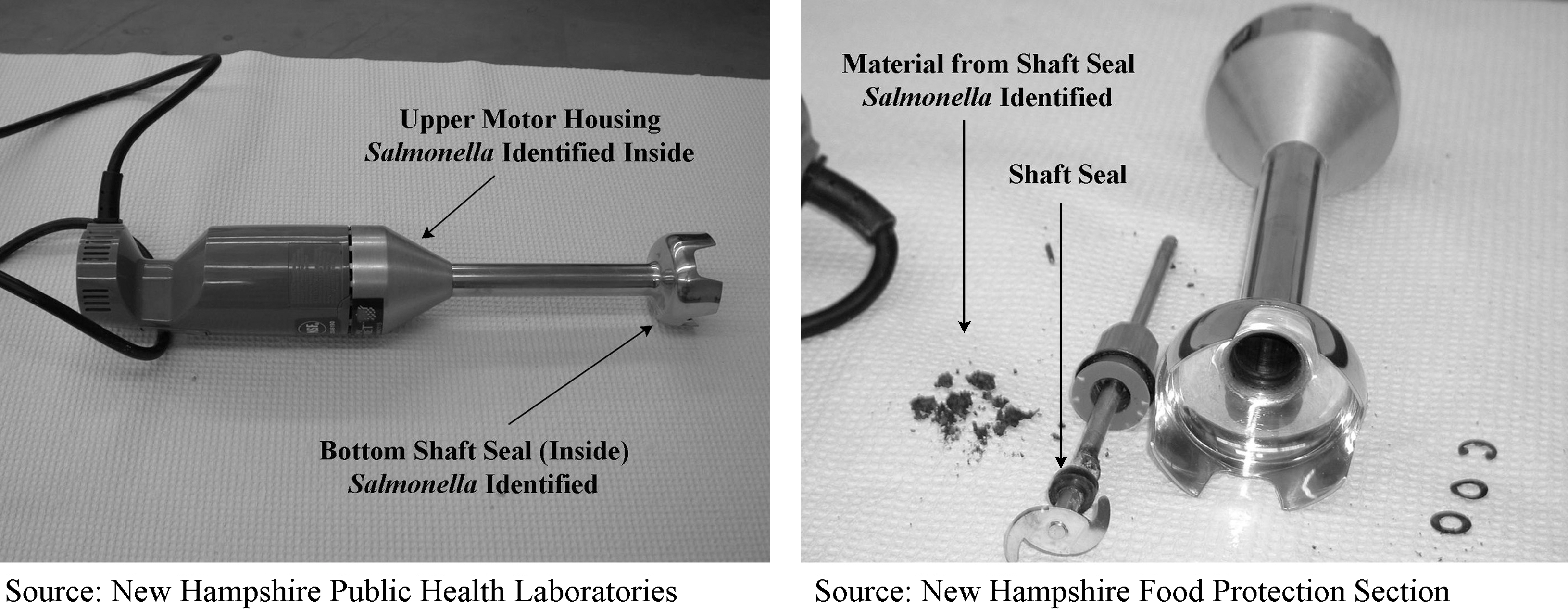
Photographs of the Salmonella-contaminated immersion blender, Salmonella outbreak, New Hampshire, 2009.
Discussion
A contaminated immersion blender used to prepare pudding caused this outbreak of salmonellosis, which resulted in 133 illnesses including 47 laboratory-confirmed Salmonella infections. The epidemiologic, environmental, and laboratory investigation determined the source of the Salmonella infections was a contaminated blender used to prepare pudding. The same strain of Salmonella identified in the human cases was also identified in prepared pudding, sterile broth mixed with the blender that mixed the pudding, and material and swabs from internal components of the blender.
Salmonella is a common cause of foodborne outbreaks, accounting for approximately half of foodborne outbreaks with a bacterial etiology in the United States; serotype Enteritidis is involved more often than any other serotype (CDC, 2006a). Salmonella Enteritidis infections have historically been associated with shell eggs, and Salmonella Enteritidis was the most common serotype of Salmonella in the United States in the 1980s and 1990s; however, incidence has decreased over the last 15 years after implementation of control efforts to reduce Salmonella Enteritidis in poultry on the farm and during egg production (Hogue et al., 1997). More recently, Salmonella Enteritidis outbreaks in the United States have been caused by a variety of commodities, including eggs and chicken, but also produce, deli meats, ground beef, and desserts (CDC, 2009). The JEGX01.0004/JEGA26.0002 pattern combination identified in this outbreak is the most common pattern of Salmonella Enteritidis identified in the United States and has historically been associated with shell eggs (Peter Gerner-Smidt, Centers for Disease Control and Prevention, personal communication, 09/04/2009).
Food blenders have previously been implicated in foodborne outbreaks, in which blender contamination was most commonly the result of inadequate or no disinfection in these investigations (Kiddy et al., 1987; Salamina et al., 1996; al-Ahmadi et al., 1998; Taylor et al., 1998). Blended foods may be at higher risk for contamination and food-blender-associated outbreaks have been identified as a serious problem in settings that serve food to vulnerable populations, such as long-term care facilities (Kirk et al., 2010).
The source of Salmonella in the blender in this outbreak is not known; however, the most likely cause of contamination was a malfunctioning shaft seal that allowed food, such as raw shell eggs, to enter and exit the shaft. Two components of the blender were contaminated with Salmonella. The upper housing containing the dried yellow residue had a row of vents through which food may have entered during mixing. The shaft seal, which contained the dark brownish-black granular material, was also contaminated. Identification of Salmonella in the broth mixed with the blender in the laboratory suggests that Salmonella inside the shaft was released through the seal into the liquid being mixed. The fact that the blender was also used to mix raw shell eggs and the identification of a common egg-associated PFGE pattern in the blender suggests shell eggs were a likely source. We were unable to detect Salmonella in the shell eggs collected for testing; however, this testing was limited by the following: (1) the shell eggs collected were not used before the outbreak when the blender likely became contaminated, and (2) the prevalence of Salmonella in shell eggs is low (Ebel and Schlosser, 2000) and the number of shell eggs tested may have been insufficient to identify one contaminated egg.
Inadequate blender sanitation is not thought to be a significant contributing factor in the described outbreak. The cleaning and sanitation of the blender did not meet licensing requirements [NH DHHS, 2003] nor the manufacturer's recommended procedure as the blender was reportedly not run for 2 minutes each in a washing solution, rinse, and sanitizing solution. Because the Salmonella-contaminated material was up inside of the shaft seal where it should not have been if the seal was functioning properly, it is unlikely that using a washing solution and running the blender for exactly 2 minutes during cleaning would have had any effect on this internal contamination. It is not clear whether the suspected malfunctioning shaft seal was the result of normal wear and tear, misuse, or damage to the blender, or a manufacturer defect. The shaft seal was not observed to have any noticeable damage; however, the blender was inspected by PHL and FPS staff who were not trained in assessing integrity of internal components of this type of equipment.
Although statistical and laboratory implication of the blender was well supported, the described outbreak investigation was limited by our inability to determine exactly how and when the blender became contaminated. The epidemiologic investigation was successful in statistically implicating a single source, and 80% of individuals in the cohort study were interviewed, which limited selection bias in interpretation of the data. Recall bias was limited by our ability to interview the majority of camp attendees within 1 week of leaving the camp.
This outbreak demonstrates the importance of collaboration between epidemiologists, food sanitarians, and laboratorians, which was critical to determining the outbreak's source. Aggressive investigation, including interviewing over 100 ill persons, multiple visits to the camp, and extensive and creative laboratory testing resulted in identification of Salmonella inside the implicated blender. Food service operators should properly disinfect and periodically inspect food service equipment in accordance with manufacturer's recommendations. Food service operators may also consider using separate equipment for raw and ready-to-eat foods when using equipment that cannot be disassembled for cleaning.
Footnotes
Acknowledgments
We thank the following persons for their contributions to study design, data collection, and specimen collection and testing: Brian Bernier (Maine Department of Health and Human Services); Emily Harvey and Tracy Stiles (Massachusetts Department of Public Health); Adam Torrey (New Hampshire DES); and Claudia Alvarado, Heather Barto, Bradley Boisvert, Royann Bossidy, Dianne Donovan, John Dreisig, Jill Drouin, Ken Dufault, Trisha Ingraham, Pamela Hill, Denise Krol, Sarah Krycki, Wendy Lamothe, Charles Metcalf, Lisa Roy, Jody Smith, and Sharon Wogaman (New Hampshire DHHS).
Disclosure Statement
No competing financial interests exist.