
Abstract
Background:
A number of countries have estimated the prevalence of acute gastroenteritis by asking survey respondents to recall past episodes of diarrhea; however, the recall period used varies between studies. We conducted a survey to examine the effects of 7-day and 1-month recall periods on the estimated annual episodes of acute gastroenteritis. Further, we examine whether asking first about illness in the previous 7 days affects a person's response to a 1-month recall period.
Methods:
The Foodborne Diseases Active Surveillance Network (FoodNet) conducted a population-based telephone survey that included asking respondents about the occurrence of gastrointestinal symptoms. From February through April 2007, we randomly split respondents into two groups to examine effect of recall periods and question order. One group was first asked about symptoms in the 7 days before interview and then asked about symptoms in the month before interview. The other group was asked only about symptoms in the month before interview.
Results:
Overall, the monthly prevalence of acute diarrheal illness (≥3 loose stools in 24-hours, lasting >1 day, or restricting daily activities) was 7.7%. This proportion was consistent among the respondents who were first asked about a 7-day recall period (n = 1436) and those asked only about symptoms in the past month (n = 2132). Extrapolation from the reported 7-day prevalence of 3.1% to an annual rate of 1.6 episodes per person, however, was almost twice the rate of episodes estimated when extrapolating from the month recall period. Similar findings were found with acute gastroenteritis (acute diarrheal illness or vomiting without respiratory symptoms).
Conclusions:
First asking respondents about a 7-day recall period did not affect the prevalence of acute gastroenteritis reported for a 1-month recall period. Recall period length did, however, have a major impact on estimates of acute gastroenteritis. Retrospective studies using different recall periods may not be comparable.
Introduction
Generally, studies of the incidence of acute gastroenteritis for estimating the burden of foodborne illness fall into two categories: prospective cohort study or retrospective cross-sectional study. Cross-sectional studies are relatively less expensive and easier to implement than prospective cohort studies. Although it is not clear which study provides the most accurate estimate, prospective cohort studies consistently report a lower frequency of acute gastroenteritis than cross-sectional surveys (Roy et al., 2006). The case definition used also has been shown to have an important impact on disease estimates (Majowicz et al., 2008).
Evidence also exists that length of the recall period may impact estimates of the incidence of acute gastroenteritis, with a higher incidence of diarrhea being reported among both adults and children in developing countries when asked about shorter, more recent time periods (Ramakrishnan et al., 1999; Melo et al., 2007; Feikin et al., 2010). To examine the impact of recall period on estimates of the incidence of acute gastroenteritis in the United States, we designed the 2006–2007 The Foodborne Diseases Active Surveillance Network (FoodNet) Population Survey to address two specific questions: Would a 7-day recall period result in a higher prevalence of acute gastroenteritis than a 1-month recall period? If yes, would asking first about the illness in the past 7 days affect the respondent's response to a 1-month recall period?
Materials and Methods
FoodNet is the principal foodborne disease component of the Centers for Disease Control and Prevention's (CDC) Emerging Infections Program and is a collaborative program among the U.S. Department of Agriculture, the U.S. Food and Drug Administration, and participating state health departments. FoodNet included 10 sites (Connecticut, Georgia, Maryland, Minnesota, New Mexico, Oregon, Tennessee, and selected counties in California, Colorado, and New York), covering 44.9 million persons or 15% of the U.S. population in 2006.
One of FoodNet's primary objectives is to determine the overall burden of foodborne illness in the United States. To achieve this, FoodNet supplements active, population-based surveillance for laboratory-confirmed cases of infection with surveys of the general population to determine the prevalence of acute gastroenteritis and associated medical care-seeking behaviors. The FoodNet Population Survey is a telephone survey of residents of the FoodNet sites administered using methods developed by CDC's Behavioral Risk Factor Surveillance System (CDC, 2002). Survey participants are selected through a two-stage process. First, a random household is selected; then, an individual from that household is selected at random using a computer-generated model that takes into account the number of males and females in a household. All persons residing in the FoodNet catchment are eligible with proxy interviews of parents or guardians used for those persons <12 years of age. A professional survey research company conducted the interviews using a computer-assisted telephone interviewing system, with the goal of 120 to 150 complete interviews per site each month.
To assess the impact of different recall periods when estimating the prevalence of acute gastroenteritis, the 2006–2007 FoodNet Population Survey used two different recall periods during its fourth quarter (February to April, 2007) when questioning participants about their history of diarrhea. The survey included a 7-day and 1-month recall period, and also changed the sequence of questions to assess the impact of question order (Fig. 1). Respondents were randomly assigned into one of two groups. The first group was asked, “In the past month, did you have vomiting?” and “In the past month, did you have diarrhea?” The second group of respondents was asked, “In the past 7 days did you have vomiting?” and “In the past 7 days, did you have diarrhea?” followed by “In the past month, did you have diarrhea?” The survey included additional questions on symptoms and illness severity, such as cough and sore throat, number of loose stools in 24 hours, duration of illness, and number of days missed from work or school.
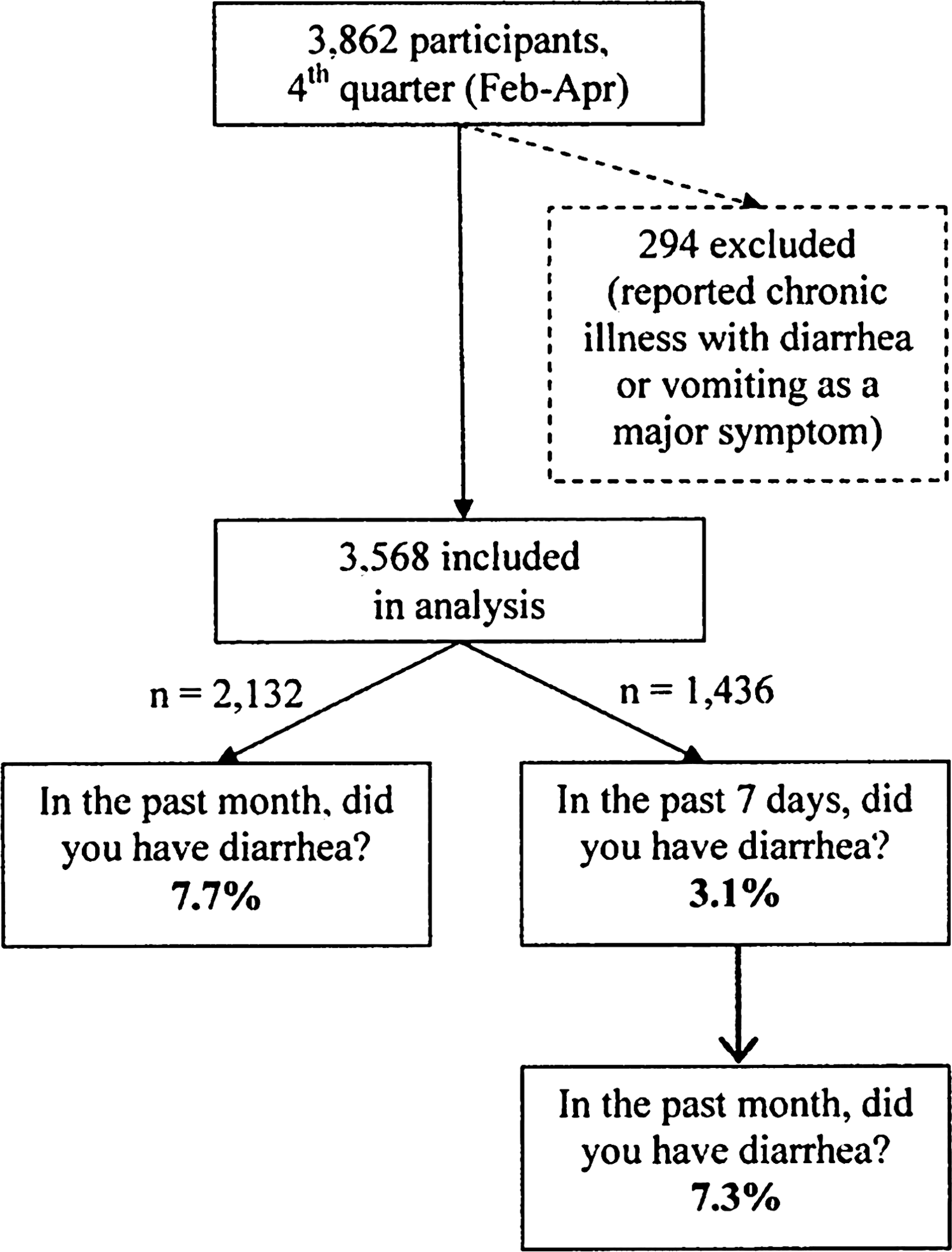
Weighted prevalence of acute diarrheal illness in the past 7 days and past month and varied question order, Foodborne Disease Active Surveillance Network (FoodNet) Population Survey, 2006–2007.
We tested differences in estimates with two definitions recently used in studies of foodborne disease in the United States. Acute diarrheal illness (ADI) was defined as diarrhea (≥3 loose stools in a 24-hour period) lasting >1 day or with restriction of daily activities (Jones et al., 2007). Acute gastrointestinal illness was defined as diarrhea (≥3 loose stools in a 24-hour period) or vomiting, lasting >1 day or resulting in the restriction of daily activities, and excluding those who reported symptoms of cough or sore throat (Scallan, unpublished data, 2009). All analyses excluded persons reporting a chronic illness in which diarrhea or vomiting was a major symptom. To compare the month and week recall periods, we multiplied the weekly proportion by 4 for an estimated monthly prevalence and calculated an annual rate from each recall period (number of episodes per person per year). We calculated frequencies, with corresponding 95% confidence intervals, and weighted all estimates to the FoodNet population to adjust for age, sex, and study design. SAS 9.0 survey procedures were used for analysis (SAS v9.0, Cary, NC).
Results
The FoodNet Population Survey included 3862 interviews in the fourth quarter when both recall periods were asked. The participants were 59.6% female, 85.3% white, 6.5% black or African American, and 6.6% Hispanic, and median age was 51 years (range, <1–99 years). After excluding persons reporting a chronic illness with diarrhea or vomiting as a major symptom, further analyses included 3568 participants.
These participants were split into two groups, and among the 2132 participants asked only about the past month, 7.7% of reported ADI in the past month. Of the remaining 1436 respondents in the second group, 3.1% reported having ADI in the past 7 days. These 1436 respondents were then asked about diarrhea in the past month; 7.3% reported having ADI during this time frame (Fig. 1). When extrapolated to estimate the number of episodes of ADI per person per year, there were 1.6 episodes per year for a 7-day recall period, compared with 0.9 episodes per year for a 1-month recall period (Table 1).
Data from two independent samples are displayed for the 2006–2007 survey. One group was asked about diarrhea in the month before interview, and the other was asked about diarrhea in the 7 days before interview.
CI, confidence interval.
When examining the impact of the recall periods using the definition of acute gastrointestinal illness, the prevalence was 6.4% for a 1-month recall period and 5.2% for a 7-day recall period, resulting in annual estimates of 0.8 episodes per person per year for a 1-month recall period and 2.7 episodes per person per year for a 7-day recall period (Table 1). Estimates from a 7-day recall period were consistently higher than from a 1-month recall period when examined by sex and also by age groups.
The prevalence of ADI in the past month (7.7%) among those asked only about a 1-month recall period was similar (7.3%) to that reported by the other half of participants who were asked first about a 7-day recall period and then about diarrhea in the past month (Fig. 1).
Discussion
Recall period length has a major impact on estimates of the prevalence of ADI and gastrointestinal illness, and estimates derived using different recall periods may not be comparable. Retrospectively asking respondents about illness in the past 7 days produced higher estimates than asking respondents about illness in the past month, regardless of order in which recall periods were asked. In fact, annual rates of ADI derived using 7-day prevalence estimates were twice the rate estimated using monthly prevalence estimates, and annual rates of acute gastrointestinal illness were 1.8 to 3.4 times higher when using a 7-day recall period instead of a 1-month recall period. These findings were consistent when applying either the ADI definition or the acute gastrointestinal illness definition. To compare the burden of ADI or gastrointestinal illness among retrospective cross-sectional studies, a common recall period should be used. Standardizing these methodological choices is also important if studies are to contribute to valid estimates of the global burden of ADI.
We determined that first asking respondents about a 7-day recall period did not affect the prevalence of acute gastroenteritis reported for a 1-month recall period. We had hypothesized that responding to the question about a short recall period (7 days) would influence the respondent's answer to the long (1 month) recall period. That is, the initial question would have the effect of bounding the respondent's recall, therefore acting as a recall aid and increasing the accuracy of respondent recall. For example, a study by Loftus et al. (1990) found that respondents reported fewer health procedures over a 2-month period when first asked about the number of health procedures undergone over a 6-month period. We did not find such an effect in this study. The 1-month prevalence of ADI in the 2006–2007 Population Survey was the same in the two independent groups despite one being asked first about a 7-day recall period.
Without verification of the reports of illness, we are unable to determine which timeframe gives a more accurate estimate. Lee and Brown (2004) suggest that when people need to guess the date of an event within a given timeframe, the tendency is to take the midpoint. Further studies are needed to determine if there is a consistent ratio between a 1-week and 1-month estimate. This ratio could then be applied to the estimates so that studies that used different timeframes could be compared. In the absence of such studies, only studies using the same timeframe can be compared. Because we could not determine which recall period is more accurate, the FoodNet Population Survey and other studies should continue to ask about both periods. The authors recommend additional studies or a future FoodNet Population survey that further examines timeframe effects, including a 1-day recall period commonly used in less industrialized countries, where households are visited several times per week (Kosek et al., 2003).
Conclusions
The findings of this study impact the design and analyses of retrospective studies that aim to estimate the burden of acute gastroenteritis. They underscore the need to consider the timeframes used in studies when comparing estimates and suggest that a 1-month recall period underestimates the global burden of foodborne illness.
Footnotes
Acknowledgments
This study was funded by the Centers for Disease Control and Protection Emerging Infections Program, the U.S. Department of Agriculture Food Safety and Inspection Service, and the Food and Drug Administration Center for Food Safety and Applied Nutrition. The authors acknowledge the staff in the 10 FoodNet sites and the FoodNet working group for their efforts in the FoodNet Population Survey.
Disclosure Statement
No competing financial interests exist.