
Abstract
Besides cardiac and neurological complications of trichinellosis, renal involvement is the most important as regards the cases published and discussed in literature and is generally characteristic of the severe forms of the disease. This article focuses exclusively on the renal disturbances that may occur in this parasitic illness and includes a synopsis of published cases. Our primary goal was to increase the awareness of infectious diseases specialists, nephrologists, and general practitioners about these complications with possible fatal outcome. To our knowledge, this is the first international review dedicated to this topic. Cases for which enough details were available have been analyzed, and the results indicated that the mean age of the affected patients was 31.6 years, with a slightly male predominance (56.2%). The fatality rate was 26.1%. Proteinuria was detected in 84.8% of cases, hematuria in 30.4%, and casts were observed in urine specimens from 23.9% of patients. Renal failure was evidenced in 8.7% of patients, whereas renal lesions were found by biopsy or necropsy in 43.5% of cases. Of the routine laboratory parameters that are relevant for trichinellosis, mean eosinophil count was 32.2% and mean leukocyte count was 17,312 cells/μL. Finally, we emphasize on the necessity of establishing an early and correct diagnosis of trichinellosis to avoid later and severe complications. Additionally, implementation of public health and food safety prophylactic measures against the disease must represent an immediate priority for the affected regions.
Introduction
Renal involvement of this malady, generally characteristic of the severe courses (Lupascu et al., 1970; Nitzulescu and Gherman, 1986; Kociecka et al., 1987; Kociecka, 2000; Enache, 2005), has been evidenced and described since the mid of 19th and beginning of the 20th centuries by Cohenheim (1865), Askanazy (1895), Frothingham (1906), and the famous scientist of Romanian origin, Babes (1906).
The present article focuses exclusively on renal disturbances of trichinellosis and includes a brief overview of selected cases reported in literature. Our primary goal was to increase the awareness of infectious diseases specialists, nephrologists, and general practitioners about these complications with possible fatal outcome. The brief summaries of the published cases may be also very useful for physicians to find them easier from a vast literature, thus adding valuable data to their clinical experience. To our knowledge, this is the first international review dedicated to this topic.
Pathology and Pathogenesis. Renal Alterations in Experimental Trichinellosis
Relevant data on experimental infection were given by Welt (1941), who inoculated Trichinella larvae in monkeys. He noticed the elimination of parasitic antigens in urine for several weeks postinfection.
Pambuccian and Cironeanu (1961), in their study on white rats, characterized the trichinous nephritis by the existence of inflammatory infiltrations and dystrophic alterations of the tubular epithelium.
Following their experience on human and veterinary cases, completed by experimental research on laboratory animals, Lupascu et al. (1970) described the pathologic modifications detected in kidneys during different phases of trichinellosis (Table 1). Nevertheless, precise characterization of the lesions according to different stages of the illness is hardly possible. Glomerular and/or tubular lesions may be noticed in severe and moderate clinical courses of trichinellosis. Renal disturbances developed during the intestinal phase of severe trichinellosis are overviewed in Table 1, and the corresponding dystrophic alterations are shown in Figure 1. It is noteworthy that these modifications were evidenced in both human cases and experimentally infected animals. Renal involvement is completely reversible in patients with moderate trichinellosis regardless of clinical picture and laboratory test results. No alterations of kidneys were seen in case of benign forms.
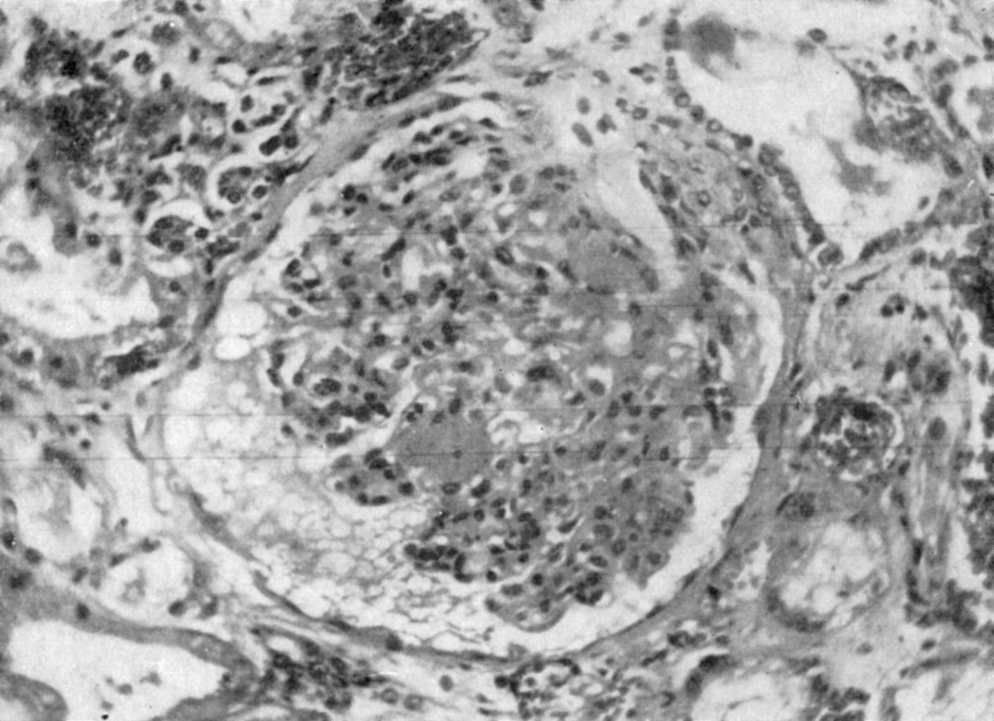
Glomerulitis with subcapsular exudates; dystrophic alterations of the tubular epithelium with cytoplasmatic vacuolation and lumen dilatation; interstitial hyperemia. Reproduced from Lupascu et al. (1970), courtesy to the Romanian Academy's Publishing House, Bucharest (EAR, Editura Academiei Romane).
During larval dissemination, lesions involve the whole nephron. Askanazy (1895) considered that glomerular and tubular lesions were due to parasite's toxic effect but could not find an evidence for the presence of Trichinella larvae in kidneys of experimentally infected animals. Frothingham (1906) detected a pronounced intracapsular and intratubular edema accompanied by a slight interstitial one and congestion of the vessels of pyramids. The specific features of glomerulitis occurring in this phase are shown in Figure 2.
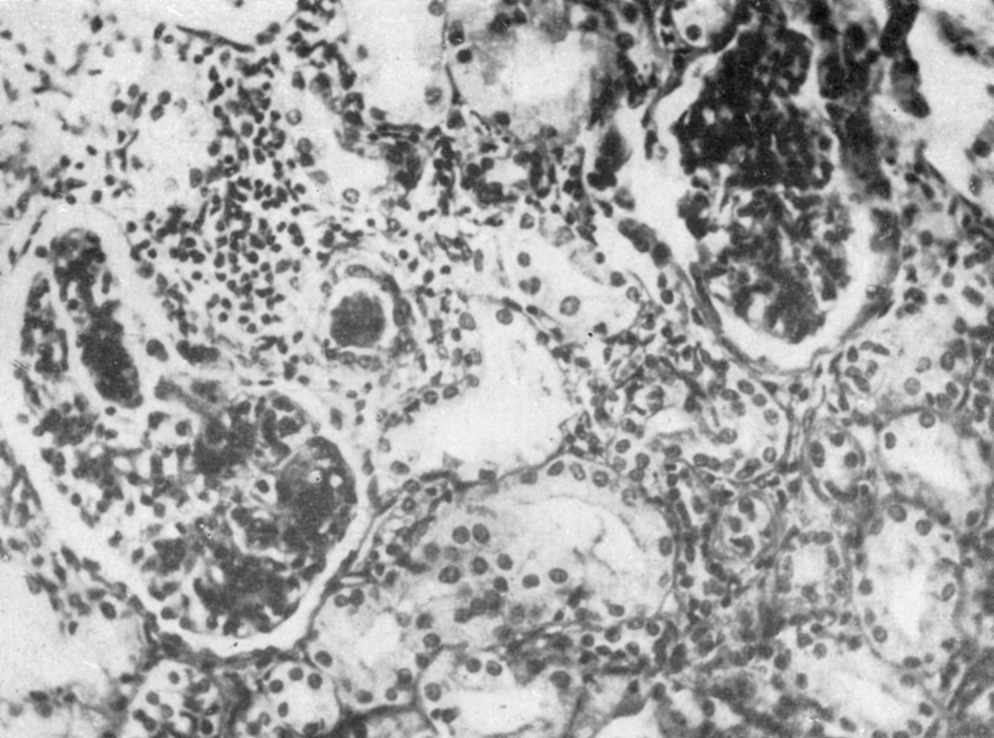
Glomerulitis with increased cellularity and alterations of the capsular epithelium; interstitial inflammatory infiltrate; cells of the tubular epithelium with vacuolation and nuclear karyopyknotic modifications. Reproduced from Lupascu et al. (1970), courtesy to the Romanian Academy's Publishing House, Bucharest (EAR, Editura Academiei Romane).
In the muscular phase, allergic glomerular nephropathy as well as different renal modifications may develop during the prolonged clinical course of the disease (Table 1). Renal impairment triggers the onset of significant compensatory mechanisms in the kidney (Lupascu et al., 1970). The specific lesions of the tubular epithelium that occur in the muscular phase of trichinellosis and are accompanied by partial atrophy are depicted in Figure 3.
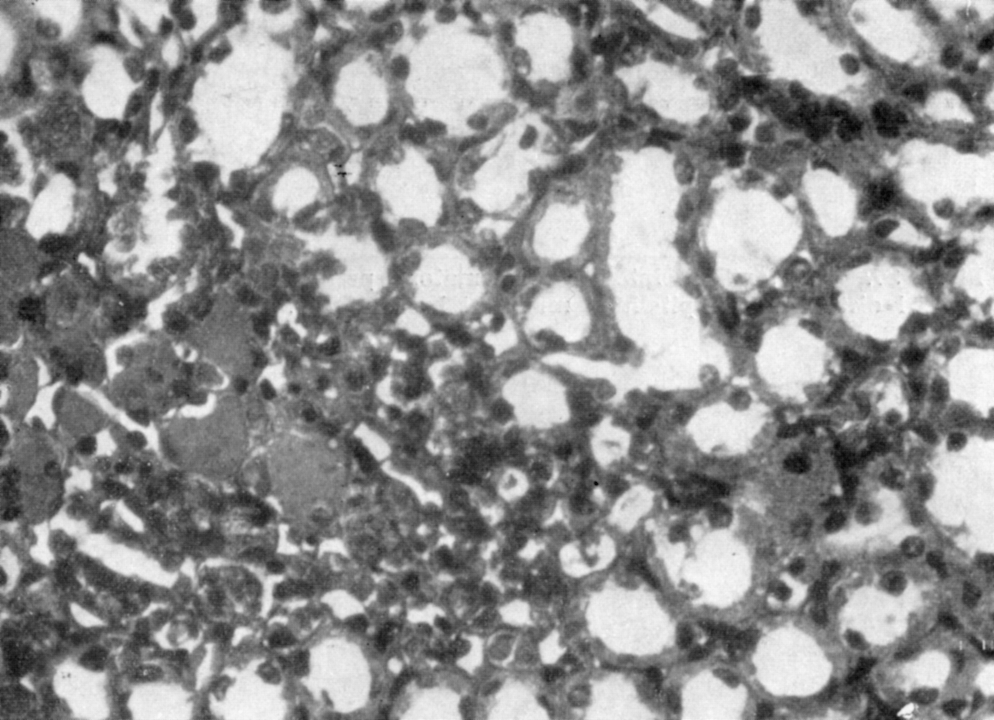
Alterations of the tubular epithelium with partial atrophy and presence of hyaline casts in some lumens. Reproduced from Lupascu et al. (1970), courtesy to the Romanian Academy's Publishing House, Bucharest (EAR, Editura Academiei Romane).
Mikhail et al. (1978) carried out an experimental study on 154 rats. They induced light (inoculation of 100 larvae) and heavy (inoculation of 500 larvae) infections in two groups of animals, aiming to determine the relationship between the intensity of infection and development of organ alterations. Examinations were made after 4 days and continued up to 18 months after the experiment. Significant modifications occurred in kidneys at 6 months postinfection and consisted of a moderate interstitial nephritis characterized by mild focal and diffuse interstitial infiltrations. At this time, no outstanding tubular or glomerular alterations were evidenced. Lesions denoting a mesangioproliferative glomerulonephritis were seen after 18 months. According to authors' opinion, the latter could finally lead to renal failure. Main pathologic changes comprised increased cellularity in the glomeruli, lobulation of the glomerular tufts due to mesangial proliferation, and a minor increase of cellular elements in the mesangial matrix. Capsular adhesions of the glomeruli and cloudy swelling with atrophic epithelial lining in the convoluted tubules were also detected. Additionally, the tubules were full with albumin casts. A diffuse infiltration of the interstitial tissue with lymphocytes was observed. Because lesions developed late in the course of infection and no larvae were detected, the possibility of an immune reaction was considered. This hypothesis could also be supported by Welt's (1941) experiments and by the clinical cases reported in literature that showed an association between trichinellosis and allergic manifestations, as periarteritis nodosa (Reimann et al., 1943; Mikhail et al., 1978; Frayha, 1981).
Trandafirescu et al. (1979) suspected the immunological nature of the renal involvement of trichinellosis and examined the biopsy samples by immunofluorescence. They evidenced intense granular deposits of immunoglobulin G and β1-globulin on the glomerular basement membranes, which supported the hypothesis that circulating immune complexes could be responsible for the occurrence of renal lesions. Additionally, the decrease of serum complement sustained their assumption. Related to these findings, Coulaud et al. (1976) previously noticed that the course of the disease was more severe and proteinuria was more pronounced in patients affected by trichinellosis who had higher circulating immune complex concentrations in serum.
Experiments carried out later revealed other interesting aspects toward clarification of the renal pathogenesis in trichinellosis. Thus, histochemical studies performed by Etewa et al. (1992) in animals showed that absorption and excretion disturbances of the renal tissue are due to the presence of endmetabolites and parasites' products in host's blood.
Cristea (1998) infected pigs and detected lesions of hyperplastic glomerulitis with metaplasia in the Bowman's capsule at 8 weeks postlarval inoculation. He also evidenced the intense positive periodic acid Schiff reaction of the vascular endothelium.
Hiranyachattada et al. (2000) induced Trichinella infection (300 larvae) in 8 rats to study possible impairment of the renal function. Additionally, they used a control group of 10 rats. Four weeks after infection, blood urea nitrogen was the only parameter that was significantly higher in the infected rats compared with the control group. This was attributed either to deficient regulation of the renal tubular urea transport or to increased muscle breakdown.
Reina et al. (2000) produced experimental disease in eight goats by using ∼10,000 larvae for each animal. As regards modifications developed in kidneys, they noticed membranoproliferative glomerulonephritis, tubular degeneration, interstitial edema, and later interstitial nephritis.
Last but not least, other valuable contributions (Gabryel et al., 1981; Weatherly, 1983; Todorova et al., 1988) confirmed the development of membranoproliferative and endotheliomesangial proliferative glomerulonephritis.
Diagnostic Key Features Regarding Renal Complications of Trichinellosis
Physicians consider that edema with abnormal urinary findings is highly associated with the diagnosis of nephritis (Mikhail et al., 1978). The trichinous nephropathy generally evolves with oliguria, proteinuria, hematuria, and presence of the casts (Kaufman, 1940; Mikhail et al., 1978; Barsoum, 1999). Involuntary urine loss was frequently reported, especially in elderly and children (Enache, 2005). The acute nephritic syndrome developed in trichinellosis may progress in some cases to acute renal failure (Barsoum, 1999).
Pathologic changes present in the kidney are revealed by needle biopsy (Mikhail et al., 1978). The most common alteration is cloudy swelling (Gould, 1945). Different studies reported the occurrence of glomerulonephritis in its acute (Guattery et al., 1956; Oziereckovskaia and Wichert, 1960; Trandafirescu, 1974; Charmot et al., 1976; Durand, 1977; Trandafirescu et al., 1979; Sitprija et al., 1980; Kociecka et al., 1987), subacute (Schoenfeld and Edis, 1967; Thompson, 1910), or chronic (Reimann et al., 1943) form. Other authors (Van Cott and Lintz, 1914) found acute diffuse nephritis or amyloid degeneration of kidneys in their patients.
Overview of Selected Cases or Cluster of Cases Reported in Literature
Methods
A literature search was initially performed in PubMed, Embase, and ISI Web of Knowledge databases using as keywords the association of the following terms: “trichinellosis,” “trichinosis,” “trichiniasis,” or “Trichinella” and “renal,” “glomerulitis,” or “nephritis.” Additionally, the archives of several high-ranking journals, different books, and other sources were searched.
Results
The most useful, complete, and relevant data on this topic were brought by cases presented by Guattery et al. (1956), Schoenfeld and Edis (1967), Trandafirescu et al. (1979), Sitprija et al. (1980), and Kociecka et al. (1987). Associations between trichinellosis and polyarteritis (periarteritis) nodosa, involving also the kidneys, are described in two articles (Reimann et al., 1943; Frayha, 1981). Case presentations with main interest for neurological (Van Cott and Lintz, 1914; Cummins and Carson, 1916a; Most and Abeles, 1937; Roehm, 1954; Dalessio and Wolff, 1961), cardiac (Roehm, 1954; Chase, 1957; Clausen et al., 1996), or other (Kushlan, 1953) complications, but only with marginal interest to the present topic, were also considered. Some reports regarding epidemics of trichinellosis (Sheldon and Lond, 1941; Thibaudeau and Gagnon, 1969) or those describing sporadic and cluster cases (Cummins and Carson, 1916b; Kaufman, 1940; Enache, 2005) with brief outlines of renal symptoms added useful data to the present analysis.
All relevant cases are overviewed in Table 2. Emphasis was given to epidemiological aspects (sex, age, profession, and country), renal and urinary abnormal findings, routine laboratory parameters (eosinophil and leukocyte count) relevant to the diagnosis of trichinellosis, and patient outcome.
In this patient, interpretation of nephritis was clouded by history of a streptococcal infection prior to hospital admission.
This patient developed 3 weeks before death an acute otitis media caused by β-hemolytic streptococcus and treated with penicillin. Nevertheless, urinary abnormalities were present before this condition was diagnosed.
These two cases were not detailed in the cited work.
Cells/μL.
F, female; L, leukocyte count (cells/μL); M, male; Eo, eosinophil count (%); NA, not available; routine lab (max.), routine laboratory test results (maximum registered value); UTI, urinary tract infection.
Analysis of cases
Cases for which enough details were available have been analyzed and the results are shown in Table 3.
Percentage of the total number of patients for whom data were available.
Discussion and Conclusions
Besides cardiac and neurological complications of trichinellosis, renal involvement is the most important as regards the cases published and discussed in literature. The hypothesis that parasites belonging to genus Trichinella may be the cause of nephropathy was supported by the simultaneous occurrence of the clinical picture highly suggestive for both trichinellosis and renal affections, necropsy reports of people deceased because of trichinellosis, and renal biopsies performed in patients diagnosed with this condition (Trandafirescu et al., 1979).
Trichinellosis is one of the most misdiagnosed diseases because of involvement of different organs and systems. Pathologic manifestations related to kidneys and urinary system may also be a source for such errors. An extensive surveillance on 699 patients with trichinellosis showed that wrong diagnosis was initially established in 45.3% of cases of whom 4.1% had renal disturbances (Nemet, 1998). One of the possible explanations may be the association between edema and abnormal urinalyses. According to our experience (Neghina et al., 2009a, 2009b, 2010a, 2010b), edema occurs frequently in trichinellosis (45.3%–64.8% of cases), and this symptom is common for both Trichinella infections and renal diseases.
Regarding the background of these complications, a brief discussion related to possible pathologic mechanisms may be stimulating. Sitprija et al. (1980) emphasized that hypercoagulability status may lead to glomerular deposition of fibrin in trichinellosis. Dystrophic lesions (sometimes lipid-related) and tubuloglomerular alterations may explain the progression to acute glomerulonephritis with signs of renal failure (Zanc, 2001). The various types of modifications were attributed to intensive parasitic invasion, substantial release of antigens, tissue destruction, increased catabolism, or hypovolemia (Kociecka et al., 1987), but the pathogenesis has not been fully understood yet. Nevertheless, it seems that the mechanism responsible for the development of renal lesions is based upon toxic and allergic manifestations (Zanc, 2001). The following evidences support the allergic status of trichinellosis: increased levels of immunoglobulin E (Zanc, 2001; Dupouy-Camet et al., 2002; Dupouy-Camet and Bruschi, 2007; Pate et al., 2010), especially between the third and fourth weeks of illness (Zanc, 2001), development of the eosinophilic capillaropathy (Zanc, 2001), and symptoms such as urticaria or periorbital angioedema (Pate et al., 2010).
Worth to be mentioned may be some peculiarities related to the clinical picture and diagnosis. Oliguria as a unique sign of renal involvement has been rarely reported in literature. It may be due to dehydration produced by diarrhea, a typical symptom of the intestinal phase of trichinellosis (Enache, 2005). Interestingly, Trandafirescu et al. (1979) showed that the clinical picture is not always correlated with the laboratory parameters and pathologic modifications (revealed by biopsy). In contrast to the results obtained by Lupascu et al. (1970) on experimental animals, Trandafirescu et al. (1979) noticed in human cases the association between mild clinical and biological picture and severe renal alterations.
Finally, concerning the therapeutic aspects, it must be emphasized that proper management of the infection may consequently lead to disappearance of the urinary sediment abnormalities (Sitprija et al., 1980; van Velthuysen and Florquin, 2000).
The analysis of the cases reported in literature has shown that more than a quarter of the patients found with renal complications have fatal outcome. Besides official statistics, the estimations indicate that >10 million people could be affected by trichinellosis worldwide, and these figures continue to increase (Dupouy-Camet et al., 2002). Consequently, numerous cases are probably undiagnosed or misdiagnosed because of myriad uncommon presentations.
In light of these facts, the present review stresses the need to establish an early and correct diagnosis of trichinellosis to avoid later and severe complications. Moreover, implementation of public health and food safety prophylactic measures against the disease must represent an immediate priority for the affected regions.
Footnotes
Disclosure Statement
No competing financial interests exist.