
Abstract
Few new drugs are available against methicillin-resistant Staphylococcus aureus (MRSA), because MRSA has the ability to acquire resistance to most antibiotics, which consequently increases the cost of medication. The objective of this study is to evaluate the potentiation of sanguinarine (SN) with selected antibiotics (ampicillin [AC], oxacillin [OX], norfloxacin [NR], ciprofloxacin [CP], and vancomycin [VC]) against MRSA. Minimum inhibitory concentration was determined by using the broth microdilution method and the synergistic effect of AC, OX, NR, CP, and VC in combination with SN was examined by the checkerboard dilution test. The results of the checkerboard test suggested that all combinations exhibited some synergy, partial synergy, or additivity. None of the combinations showed an antagonism effect. The combination of SN plus CP exhibited maximum synergistic effect in 11/13 strains, followed by SN plus NR in 9/13 strains, and AC and OX in 7/13 strains each. The combination of SN with VC, however, mostly showed partial synergy in 11/13 strains. The time-kill assay showed that SN in combination with other antibiotics reduced the bacterial count by 102–103 colony forming units after 4 h and to less than the lowest detectable limit after 24 h. Although in vivo synergy and clinical efficacy of SN cannot be predicted, it can be concluded that SN has the potential to restore the effectiveness of the selected antibiotics, and it can be considered in an alternative MRSA treatment.
Introduction
M
Sanguinarine (SN) is a benzophenanthridine alkaloid derived from the root of Sanguinaria canadensis and other poppy-fumaria species, which possesses potent antibacterial, antifungal, and anti-inflammatory activities (Kim et al., 2008). Studies of SN have also shown some plaque and gingivitis reduction (Ciancio, 1992; Grenby, 1995), killing of animal cells through its action on the Na+-K+-ATPase transmembrane protein (Pitts and Meyerson, 1981). If applied to the skin, SN kills cells and may destroy tissue. In turn, the bleeding wound may produce a massive scab. In plants, SN is synthesized from dihydrosanguinarine through the action of dihydrobenzophenanthridine oxidase (Howell, 1972).
In this study, we evaluated the potentiation of SN with selected antibiotics (ampicillin [AC], oxacillin [OX], norfloxacin [NR], ciprofloxacin [CP], and vancomycin [VC]) against MRSA.
Materials and Methods
Bacterial strains and culture medium
MRSA strain ATCC 33591 (American Type Culture Collection, Manassas, VA) was commercially purchased, and the other 12 clinical isolates used in this study were obtained from different patients at the Wonkwang University Hospital (Iksan, South Korea). Before use, all bacteria were stored in 30% glycerol and frozen at −70°C. The bacteria were cultured in Mueller–Hinton broth (MHB) and Mueller–Hinton agar (MHA) (Difco Laboratories) and incubated at 37°C for 20 h.
Antimicrobial agents
SN, AC, OX, NR, CP, and VC were all purchased from Sigma–Aldrich Co.
Determination of the minimum inhibitory concentrations
We used 12-h broth cultures as microbial inocula and adjusted the turbidity of bacterial suspensions to 0.5 McFarland standard solution. Susceptibility tests were performed using standard broth microdilution method in accordance with the Clinical and Laboratory Standard Institute (CLSI, 2000) guidelines. Each well was briefly loaded with 100 μL of MHB, 10 μL of antibiotics, and 10 μL of the inoculum (approximately 106 colony forming units [CFU]/mL) to achieve a final inoculum concentration of 5×104 CFU/mL in all wells. The minimum inhibitory concentration (MIC) value was the lowest concentration of commercially purchased antibiotics that inhibited visible growth after 24 h of incubation at 37°C.
At the end of the incubation period, the well plates were visually examined for turbidity. Cloudiness indicates that bacterial growth has not been inhibited by the concentration of antimicrobial agent contained in the medium. A colorimetric assay for rapid detection of the presence of bacteria was also performed (see below, Colorimetric assay using 3-(4,5-dimethylthiazol-2-yl)-2,5-diphenyl tetrazolium bromide [MTT] test).
Checkerboard dilution test
Antibacterial effects of the combination of two antimicrobial agents were assessed by the checkerboard test. Serial dilutions of two different agents were mixed in cation-supplemented MHB. Inocula were prepared from colonies that had been grown overnight on MHA. The final bacterial concentration after inoculation was 5×104 CFU/mL. MIC was determined after 24 h of incubation at 37°C.
Interpretation of synergy effect
The synergy effect was evaluated according to the published standards (Odds, 2003; Miranda-Novales et al., 2006; Lee et al., 2008).
The microtiter plates were then incubated at 37°C and MIC was determined after 24 h of incubation. The fractional inhibitory concentration (FIC index) for all the combinations was determined using the following formula,
FIC index=FICA + FICB=[A]/MICA + [B]/MICB
FICA, FICB– FIC of drug A and B respectively. MICA, MICB–MIC of drug A and B respectively. [A], [B]–Concentration of drug A and B respectively.
FIC index by checkerboard method is interpreted as follows: ≤0.5- synergy; >0.5 and ≤4- additivity; and >4- antagonism.
Colorimetric assay using MTT test
A colorimetric assay based on MTT for rapid detection of the presence of bacteria was performed as previously described (Scheuber et al., 1983; Abate et al., 1998; Shi et al., 2008). Briefly, a stock solution of 5 mg/mL MTT (Sigma) was prepared in phosphate-buffered saline and kept at −70°C. A final concentration of 1 mg/mL of MTT was used in the assay. After 24 h of incubation a 37°C, 20 μL of the yellow MTT was added to the 96-well microtiter plate (0.3 mL volume; Nunc) and incubated for an additional 20 min. The presence of a blue color indicates the presence of bacteria.
Time-kill assay
Viable counts for the determination of living-Viable were performed as previously described (Choi et al., 2010) using 100 μL of culture medium. Inocula of 5×104 CFU/mL were exposed to the antibacterial either singly or in combination with SN and incubated at 37°C; 0.1-mL aliquots of the culture were removed at 0, 4, 12, and 24 h of incubation; and serial 10-fold dilutions were prepared in saline as needed. The numbers of viable cells were determined on a drug-free MHA plate after 24-h incubation. Colony counts were performed on plates, and 30–300 colonies were obtained. The lower limit of sensitivity of colony counts was 100 CFU/mL. Antimicrobials were considered as bactericidal at the lowest concentration that reduced the original inoculum by 3 log10 CFU/mL (99.9%) at each time period, and bacteriostatic if the inoculum was reduced by 0–3 log10 CFU/mL.
Results
MIC determinations
The susceptibilities of 13 MRSA strains to the tested antibiotics are shown in Table 1. SN was the most potent; with MICs ranging from 1.56 to 6.25 μg/mL. VC had an MIC of 1.95 μg/mL in 77% of the strains. All strains were resistant to AC, OX, NR, and CP with MICs ranging from 31.25 to 1000 μg/mL. Our in vitro results show that the MIC of these antibiotics is within the range that has been reported by other researchers against S. aureus (Dzink and Socransky, 1985; Kwon et al., 2007; Choi et al., 2010).
AC, ampicillin; OX, oxacillin; NR, norfloxacin; CP, ciprofloxacin; VC, vancomycin; SN, sanguinarine; DPS, clinical isolates from Wonkwang University Hospital.
Evaluation of synergy effect
Checkerboard
When tested against ATCC33591, our data indicated that SN or AC alone only had moderate inhibitory effect on the growth of MRSA (Table 1). However, in the presence of a nongrowth inhibitory dose of AC (31.25 μg/mL) or SN (0.049 μg/mL), SN together with AC was highly effective with a FIC of 0.09 (Table 2). Similar effects were also observed in 12 other MRSA strains (DPS-1 to DPS-12) and other antibiotics (OX, NR, CP and VC), suggesting that SN is an effective agent in suppressing MRSA growth. These results showed that SN in combination with these antibiotics could effectively inhibit MRSA growth. None of the combinations showed an antagonistic effect. For the isolates showing synergistic effect, SN decreased the MICs of the antibiotics by 4–32-fold.
Values obtained from a, b, c, d, and e are MIC of each antibiotic in combination.
MIC of SN in combination with AC/ MIC of AC in combination with SN.
MIC of SN in combination with OX/ MIC of OX in combination with SN.
MIC of SN in combination with NR/ MIC of NR in combination with SN.
MIC of SN in combination with CP/ MIC of CP in combination with SN.
MIC of SN in combination with VC/MIC of VC in combination with SN.
ATCC 33591 (American Type Culture Collection).
FIC, fractional inhibitory concentration; MIC, minimum inhibitory concentration.
The combination with the highest rate of synergy is shown in Table 3. In double combinations, synergy occurred at the highest rate with combinations involving SN plus CP (11/13), followed by SN plus NR (9/13), and AC and OX (7/13, each). The combination of SN with VC, however, mostly showed partial synergy (11/13). These results demonstrated that the combination of SN with these antibiotics could be used to suppress MRSA growth.
Combination of SN+AC, sanguinarine plus ampicillin; SN+OX, sanguinarine plus oxacillin; SN+NR, sanguinarine plus norfloxacin; SN+CP, sanguinarine plus ciprofloxacin; SN+VC, sanguinarine plus vancomycin.
MRSA, methicillin-resistant Staphylococcus aureus.
Time-kill curve analysis
To confirm the synergistic effect of SN and the selected antibiotics on MRSA, the time-kill test was performed. The control showed no reduction in CFU counts, and bacterial growth of approximately 102 cells was obtained within 4 h of incubation when exposed to 1/2 MIC of the selected antibiotics. As shown in Figure 1, SN alone (0.78 μg/mL) and AC alone (250 μg/mL) do not induce cell death after 24-h incubation. When used together, SN and AC synergistically caused a reduction in bacterial count from 102 CFU to 103 CFU below the lowest detectable limit after 24 h, indicating potentiation of AC by SN against MRSA. Similar effects were also observed with the other antibiotics (Figs. 2 –5). SN caused a reduction in bacterial count from 102 CFU to 103 CFU after 4 h and a reduction to below the lowest detectable limit after 24 h. However, as shown in Figure 5, when SN was used in combination with VC, the bacterial counts were still detectable after 24 h.
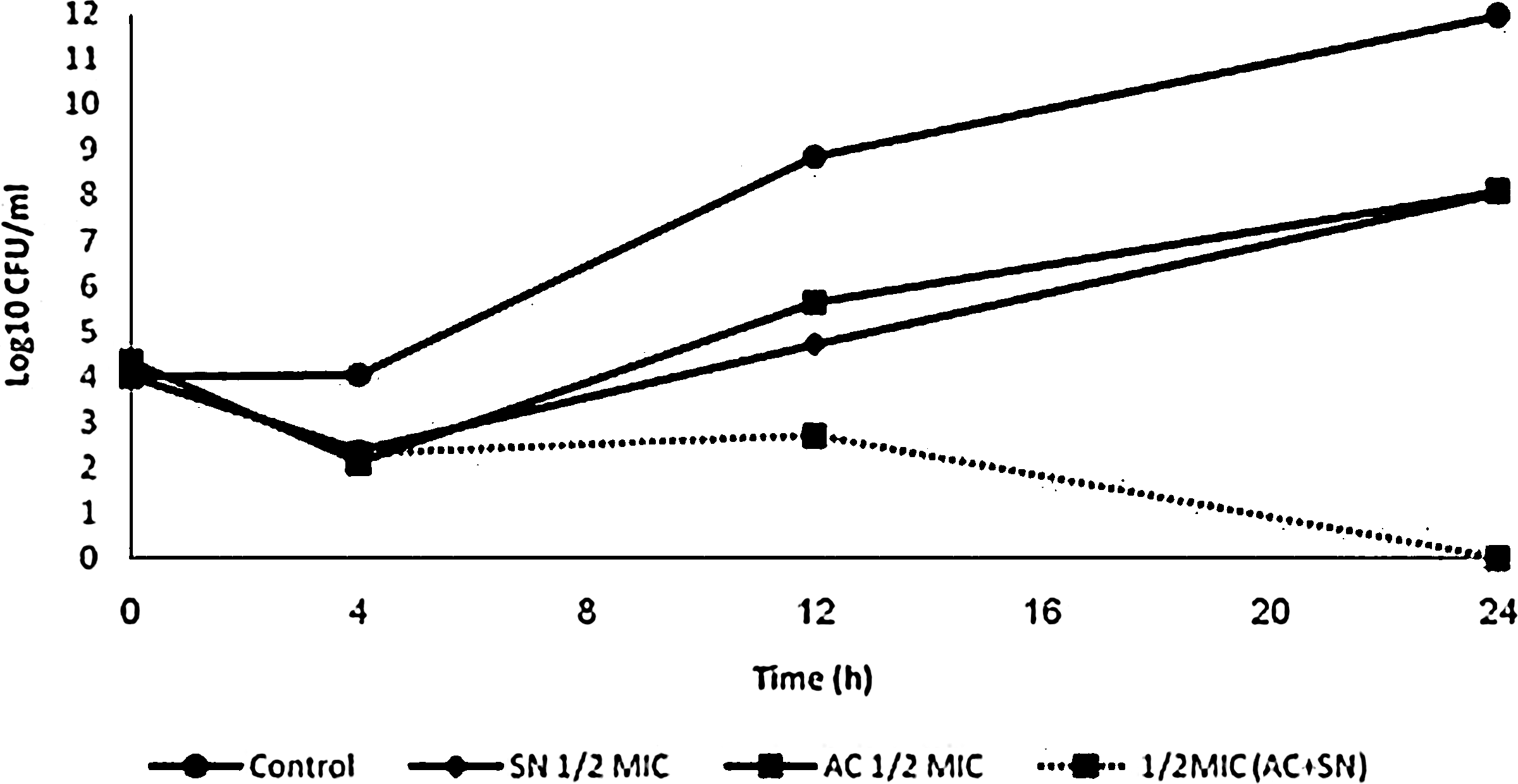
Effect of AC combined with SN on viablecounts of methicillin-resistant Staphylococus aureus (ATCC 33591). AC, ampicillin; SN, sanguinarine; MIC, minimum inhibitory concentration; CFU, colony forming units.
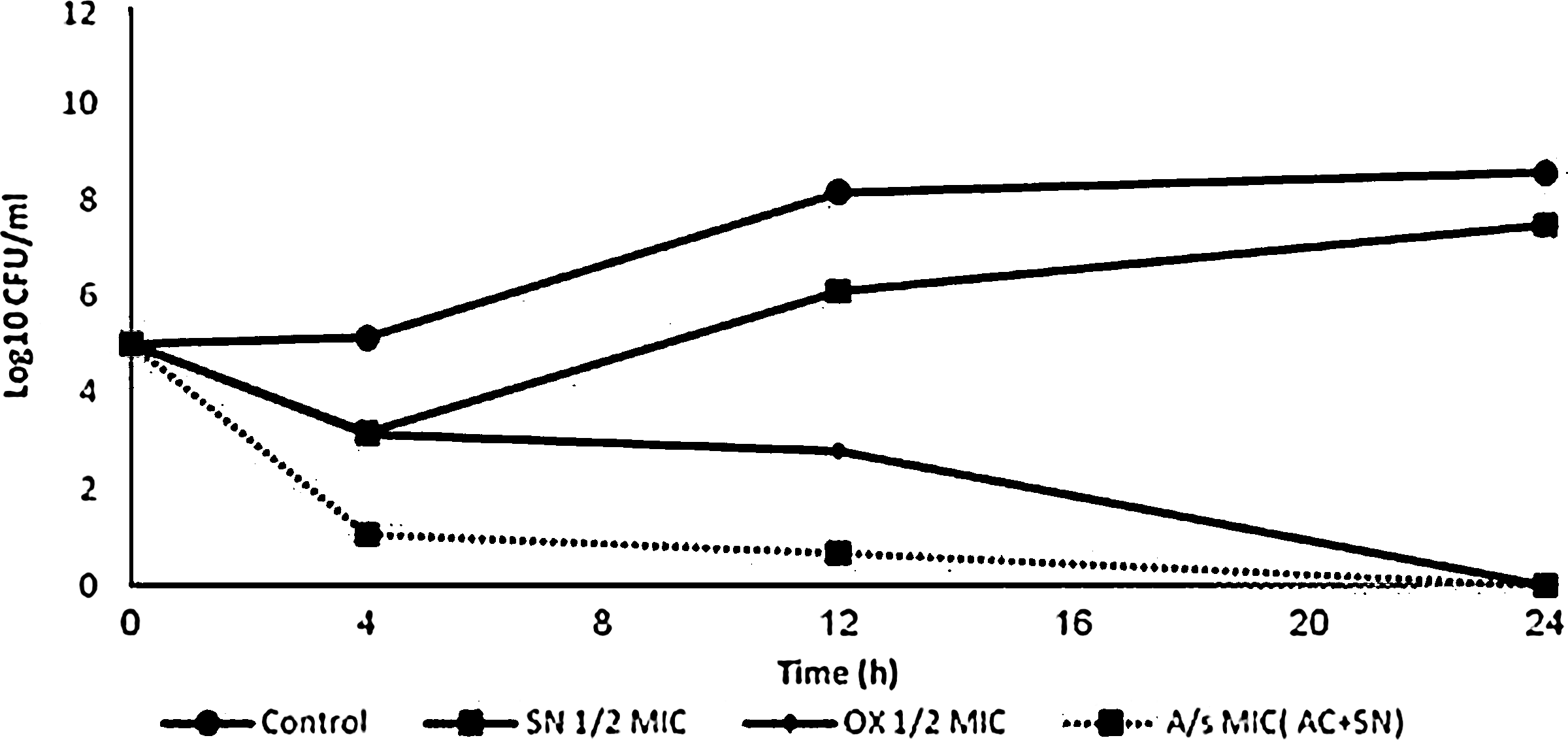
Effect of OX combined with SN on viablecounts of methicillin-resistant S. aureus (ATCC 33591). OX, oxacillin.

Effect of NR combined with SN on viablecounts of methicillin-resistant S. aureus (ATCC 33591). NR, norfloxacin.
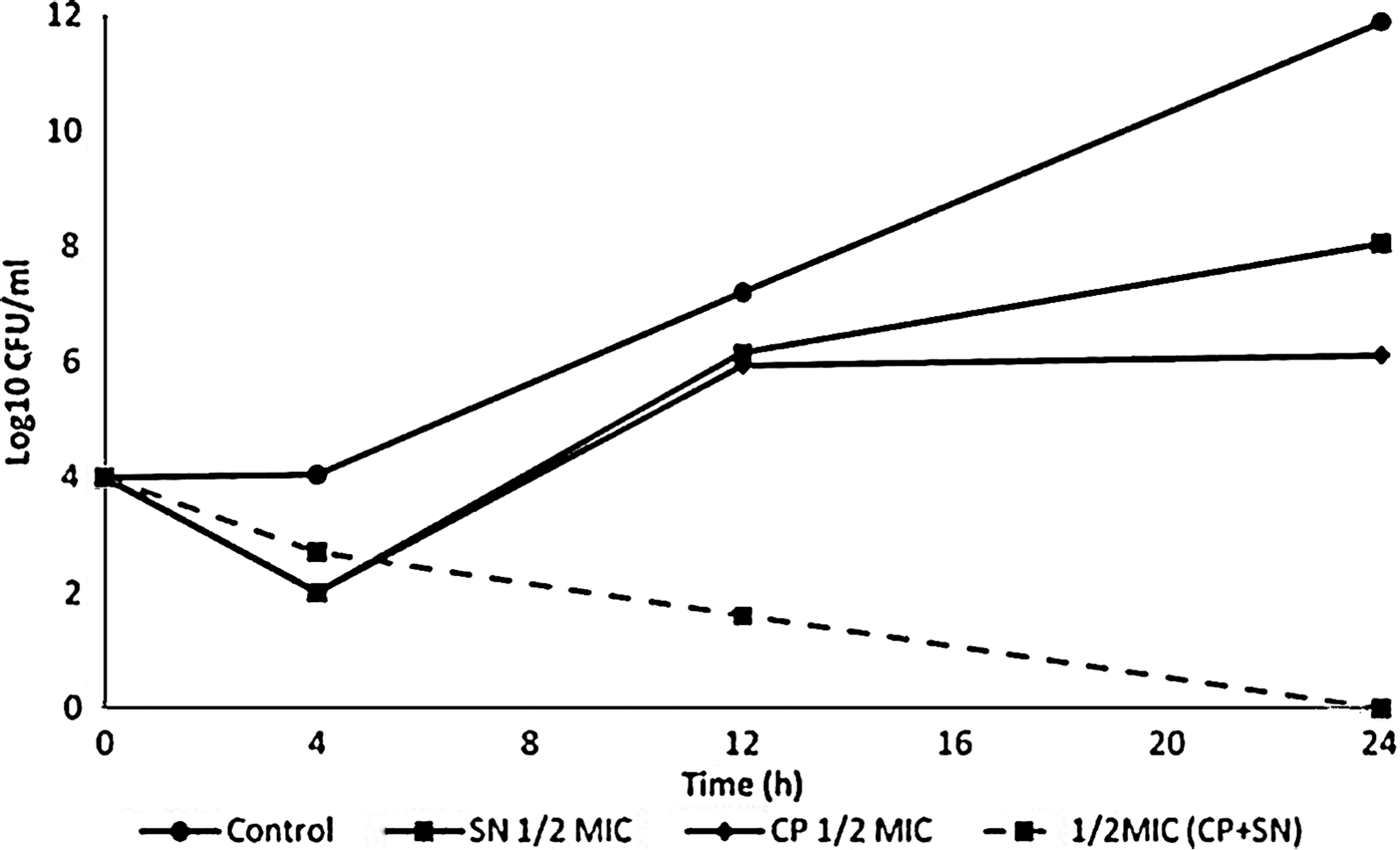
Effect of CP combined with SN on viablecounts of methicillin-resistant S. aureus (ATCC 33591). CP, ciprofloxacin.
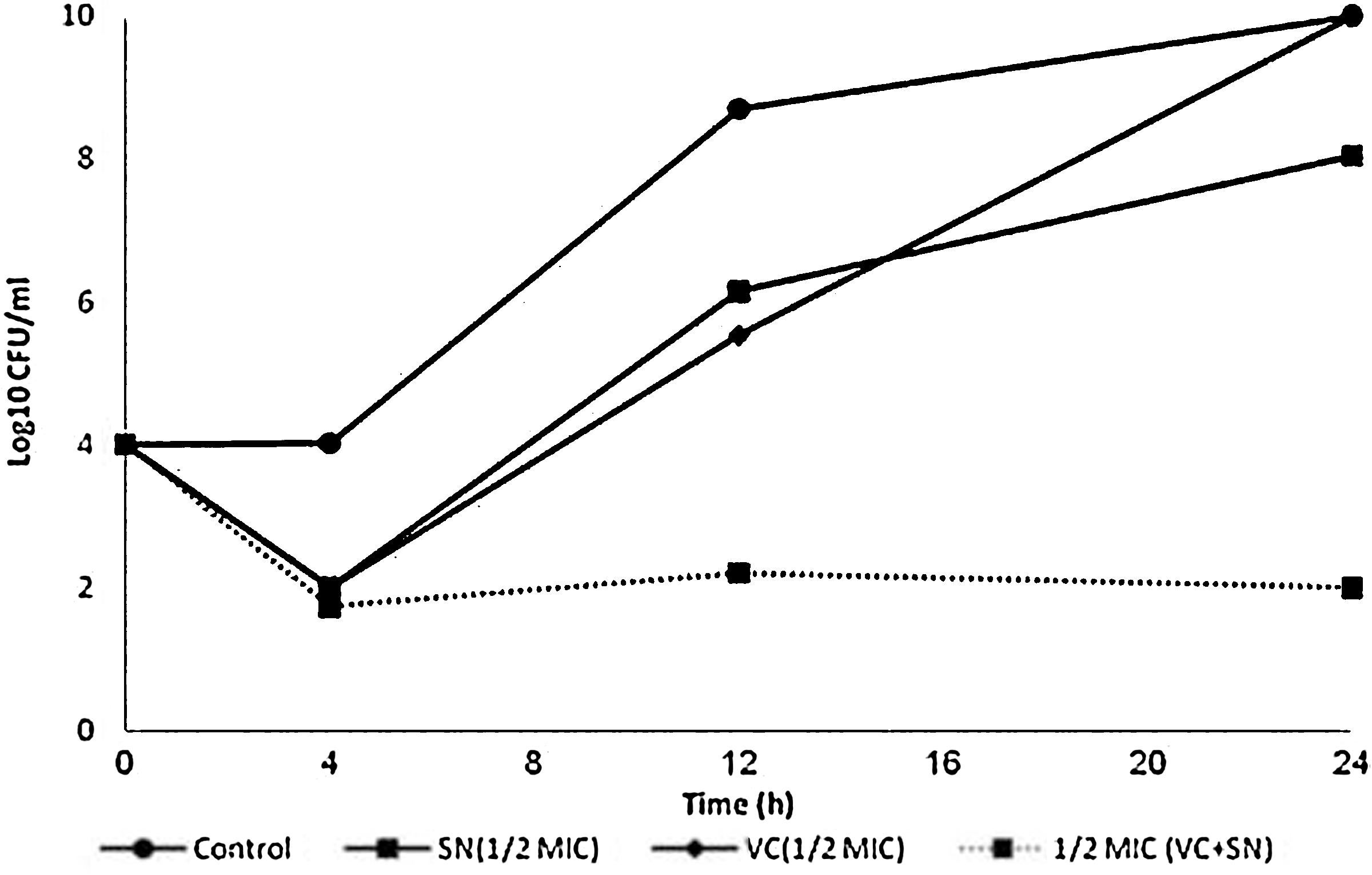
Effect of VC combined with SN on viablecounts of methicillin-resistant S. aureus (ATCC 33591). VC, vancomycin.
Discussion
The ability of MRSA to acquire resistance to most antibiotics has significantly increased the worldwide mortality caused by MRSA infection (Gibbons, 2004; Dancer, 2008). The use of two drugs in combination is a good alternative to slow the process of developing drug resistance and to restore the effectiveness of drugs that are no longer prescribed. Combination therapy is the most commonly recommended empirical treatment for bacterial infections in intensive care units, where monotherapy may not be effective against all potential pathogens, and for preventing the emergence of resistant mutants (Drago et al., 2007). The findings of the present study have potential implications in delaying the development of resistance as the antibacterial effect achieved with lower concentration of antibiotics used in combination with SN (Table 2). In various MRSA strains, SN or the selected antibiotics alone moderately inhibited bacteria growth. When combined together, these antibiotic effects were dramatically increased. These effective combinations could be new promising agents in the management of MRSA. For antimicrobial drugs, the clinical application of a combination of inhibitory agents often begins with in vitro tests that show positive interactions for inhibiting the growth of target microorganisms (Odds, 2003). Different drug combinations are reported to treat infections caused by pathogens (Liu et al., 2000; Maranda-Novales et al., 2006; Drago et al., 2007; Vidaillac et al., 2010). To our knowledge, this is the first report investigating the potentiation of AC, OX, NR, CP, and VC by SN against MRSA.
Unlike AC, OX, NR, and CP, VC, and SN showed inhibitory effects against all strains. The ability of MRSA to acquire resistance and the limited choice of antimicrobial agents suggested that continual monotherapy may increase resistance and further decrease the choice among already limited prescribed drugs. Consequently, the mortality rates will continue to increase rapidly. Further, the overall consumption of penicillin was associated with MRSA acquisition at a group level, whereas fluoroquinolone exposure increased the risk of MRSA acquisition by individual patients (Dancer, 2008).
The fluoroquinolones used in this study are NR and CP. In comparison to its combination with β-lactam antibiotics (AC and OX), SN combined with CP showed maximum synergistic effect, followed by its combination with NR. Fluoroquinolones and β-lactams have different mechanisms of action. β-Lactams selectively inhibit bacterial cell wall biosynthesis (Bycroft and Shute, 1985), whereas fluoroquinolones such as NR function by inhibiting DNA gyrase (a type II topoisomerase) and topoisomerase IV (Drlica and Zhao, 1997); enzymes that unwind bacterial DNA and inhibit cell division. Although the mechanism of SN-induced apoptosis and the sensitizing effect of SN on TRAIL-induced breast cancer has been investigated (Kim et al., 2008), it will be premature to suggest a possible mechanism of action of SN in combination with other antimicrobials against MRSA based on its synergistic effect. However, in all cases, even those in which synergy were not observed, SN markedly reduced the MICs of all selected antibiotics up to 32-fold. The results obtained through the checkerboard test suggested that the combination of fluoroquinolone antibiotics and SN can be used in very low doses, which decreases the toxicity associated with their usage on mammalian cells in culture (Hussy et al., 1986).
The time-kill curves shown in Figures 1 –5 confirmed the ability of SN to synergistically reduce the bacterial counts below the lowest detectable limit after 24 h, with exception of its combination with VC. Therefore, SN in combination has the ability to restore the effectiveness of AC, OX, NR, and CP.
Although in vivo synergy and clinical efficacy of SN cannot be predicted, it can be concluded that SN has the potential to restore the effectiveness of the selected antibiotics and it can be an alternative to conventional MRSA treatment. Studies to determine the possible mechanism of SN action on MRSA are in progress. The synergistic effect or even the additive activity of such compounds could be an alternative to monotherapy, especially in developing countries where the availability of new drugs is limited.
Footnotes
Acknowledgment
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (NRF-2009-351-E00044).
Disclosure Statement
No competing financial interests exist.