
Abstract
Salmonella species cause an estimated 1.2 million infections per year in the United States, making it one of the most commonly reported enteric pathogens. In addition, Salmonella is an important cause of travel-associated diarrhea and enteric fever, a systemic illness commonly associated with Salmonella serotypes Typhi and Paratyphi A. We reviewed cases of Salmonella infection reported to the Centers for Disease Control and Prevention's (CDC) Foodborne Diseases Active Surveillance Network (FoodNet), a sentinel surveillance network, from 2004 to 2008. We compared travelers with Salmonella infection to nontravelers with Salmonella infection with respect to demographics, clinical characteristics, and serotypes. Among 23,712 case-patients with known travel status, 11% had traveled internationally in the 7 days before illness. Travelers with Salmonella infection tended to be older (median age, 30 years) than nontravelers (median age, 24 years; p<0.0001), but were similar with respect to gender. The most common destinations reported were Mexico (38% of travel-associated infections), India (9%), Jamaica (7%), the Dominican Republic (4%), China (3%), and the Bahamas (2%). The proportions of travelers with Salmonella infection hospitalized and with invasive disease were inversely related to the income level of the destination (p<0.0001). The most commonly reported serotypes, regardless of travel status, were Enteritidis (19% of cases), Typhimurium (14%), Newport (9%), and Javiana (5%). Among infections caused by these four serotypes, 22%, 6%, 5%, and 4%, respectively, were associated with travel. A high index of clinical suspicion for Salmonella infection is appropriate when evaluating recent travelers, especially those who visited Africa, Asia, or Latin America.
Introduction
We describe cases of Salmonella infection reported to the Centers for Disease Control and Prevention's (CDC) Foodborne Diseases Active Surveillance Network (FoodNet), a population-based sentinel surveillance network, from 2004 to 2008. We compared travelers with Salmonella infection to nontravelers with Salmonella infection with respect to demographics, clinical characteristics, and serotypes.
Materials and Methods
FoodNet is part of CDC's Emerging Infections Program and is a collaboration among the CDC, the U.S. Department of Agriculture's Food Safety and Inspection Service, the U.S. Food and Drug Administration, and 10 state health departments (Scallan, 2007). FoodNet conducts active surveillance for laboratory-confirmed Salmonella infections in Connecticut, Georgia, Maryland, Minnesota, New Mexico, Oregon, and Tennessee, and selected counties in California, Colorado, and New York. In 2008, the total population of FoodNet's catchment area was ∼44.5 million people or 15% of the U.S. population. FoodNet personnel routinely contact each of the ∼650 clinical laboratories that serve the populations under surveillance to ascertain all cases of Salmonella infection among residents from all specimen sources (e.g., stool and blood). For each Salmonella infection reported during 2004–2008, FoodNet epidemiologists collected demographic and clinical information using a standard case report form, including information on whether the case-patient traveled outside the United States in the 7 days before illness began, and if so, to which country or countries.
“Travel” in this analysis is synonymous with “international travel outside the United States.” All case-patients with known travel status (“yes” or “no”) were included in the analysis; those with unknown travel status were excluded. For analyses of travel destination, only case-patients reporting travel to a single country were included. Travel destination data were available for case-patients from seven FoodNet sites, California Colorado, Connecticut, Georgia, Maryland, Minnesota, and Tennessee.
Travel destinations were grouped into six geopolitical regions using World Health Organization's (WHO) Global Foodborne Infections Network classification scheme (Galanis et al., 2006). To determine if Salmonella infections acquired in countries with different levels of economic development vary by serotype and the clinical characteristics of the resulting illness, travel destinations were also grouped by level of economic development (high, upper middle, lower middle, and low income), using the 2008 World Bank's List of Economies (
Case-patients were classified as “hospitalized” if they were admitted to a hospital within 7 days of the specimen collection date. A Salmonella infection was classified as “invasive” if the isolate was obtained from blood, cerebrospinal fluid (CSF), or another normally sterile site. Salmonella serotypes Typhi and Paratyphi A were classified as typhoidal, as these serotypes are genetically monomorphic and cause clinically identical illnesses (Gupta et al., 2008; Crump and Mintz, 2010). Serotypes other than Typhi, Paratyphi A, and Paratyphi B and C (excluded from analysis because of incomplete surveillance data) were classified as nontyphoidal.
Analyses were performed using SAS, version 9.1 (SAS Institute, Cary, NC). The univariate procedure was used for continuous variables. The Chi-square test statistic was calculated for categorical variables. The Mann–Whitney test was used to compare median ages of travelers and nontravelers. The Cochran-Armitage test of trend using the exact permutation method for a nonnormal distribution was used to analyze the proportion of travelers to countries of each World Bank income level who were hospitalized and who had invasive disease. A p-value of <0.05 was considered statistically significant.
Results
A total of 33,964 culture-confirmed Salmonella infections were reported to FoodNet from 2004 to 2008. Information as to whether the case-patient had traveled was available for 23,712 (70%), of whom 2659 (11%) reported travel outside the United States in the 7 days before illness began. By year, the proportion of Salmonella infections that was travel-associated remained relatively constant (ranging from 9% in 2008 to 13% in 2005), but the proportion that was travel-associated varied by site, from 6% in Georgia to 19% in Colorado.
Travelers with Salmonella infection were somewhat older (median age, 30 years) than nontravelers (24 years; p<0.0001) (Table 1). Among travelers, 4% and 6% were <1 year old or >65 years old, respectively, compared with 11% and 12% of nontravelers. Travelers and nontravelers were similar with respect to ethnicity (defined as Hispanic or non-Hispanic) and gender but not with respect to race; Asians represented 11% of travelers and 4% of nontravelers with Salmonella infection. Conversely, 5% of travelers and 11% of nontravelers were black (Table 1).
Missing age data for case-patients with known travel status: 166 travelers, 1207 non-travelers, 1373 total.
Missing gender data for case-patients with known travel status: 6 travelers, 46 non-travelers, 52 total.
A.I., American Indian; A.N., Alaska Native; P.I., Pacific Islander; N.H., Native Hawaiian.
Destination information was available for 1692 (64%) travelers. Among the 1645 travelers who visited a single destination, 107 countries were reported. The most common destinations reported were Mexico (38% of travel-associated infections), India (9%), Jamaica (7%), the Dominican Republic (4%), China (3%), and the Bahamas (2%).
Overall, 20% of travelers and 29% of nontravelers with a Salmonella infection were hospitalized (p<0.0001), although 14% of travelers and 6% of nontravelers had invasive infections (p<0.0001). Typhoidal infections were more common among travelers than nontravelers (10% vs. <1%, p<0.0001) (Table 2). Similarly, hospitalization and invasive disease were more common among typhoidal infections. Among those infected with typhoidal serotypes, 67% of travelers and 65% of nontravelers were hospitalized, whereas 84% of travelers and 75% of nontravelers had invasive disease. Among those with infections caused by nontyphoidal serotypes, 15% of travelers and 28% of nontravelers were hospitalized, and 6% of travelers and 5% of nontravelers had invasive disease. The lower the World Bank income level of the destination, the higher the proportion of travelers with Salmonella infection who were hospitalized, ranging from 17% for high-income destinations to 37% for low-income destinations (p<0.0001) (Fig. 1). This trend became nonsignificant when stratifying by typhoidal versus nontyphoidal serotypes. For example, for nontyphoidal infections only, 34 (16%) of 214 travelers returning from a high-income destination were hospitalized, compared with 92 (11%) of 833 travelers to upper middle-income countries, 48 (16%) of 301 to lower-middle-income countries, and 26 (27%) of 97 to low-income countries. Similarly, the lower the World Bank income level of the destination, the higher the proportion of travelers with invasive disease, ranging from 3% for high-income countries to 33% for low-income countries (p<0.0001) (Fig. 2).
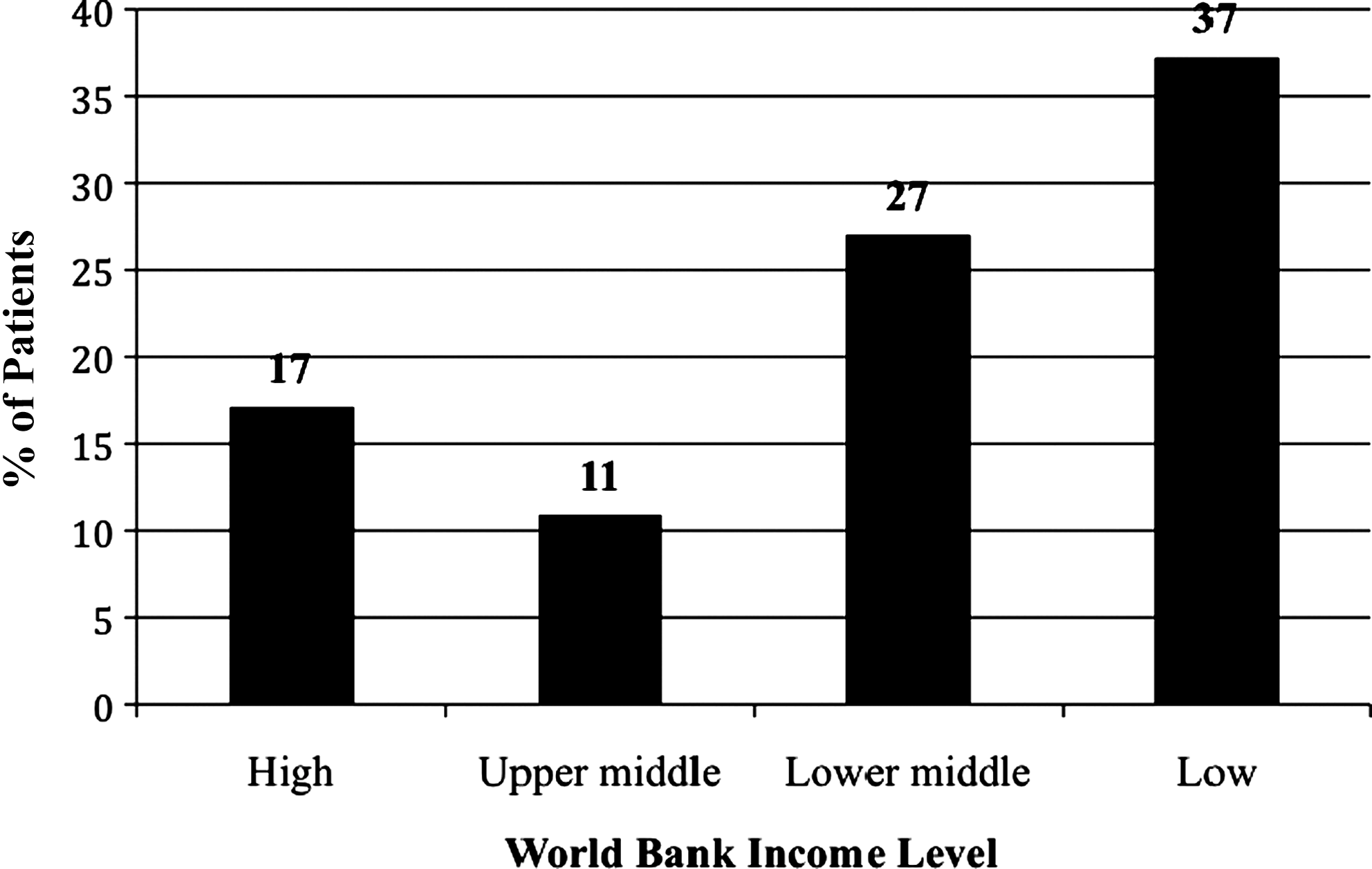
The percent of patients hospitalized among travel-associated Salmonella infections reported to FoodNet from 2004 to 2008, by World Bank income level (n=1594).
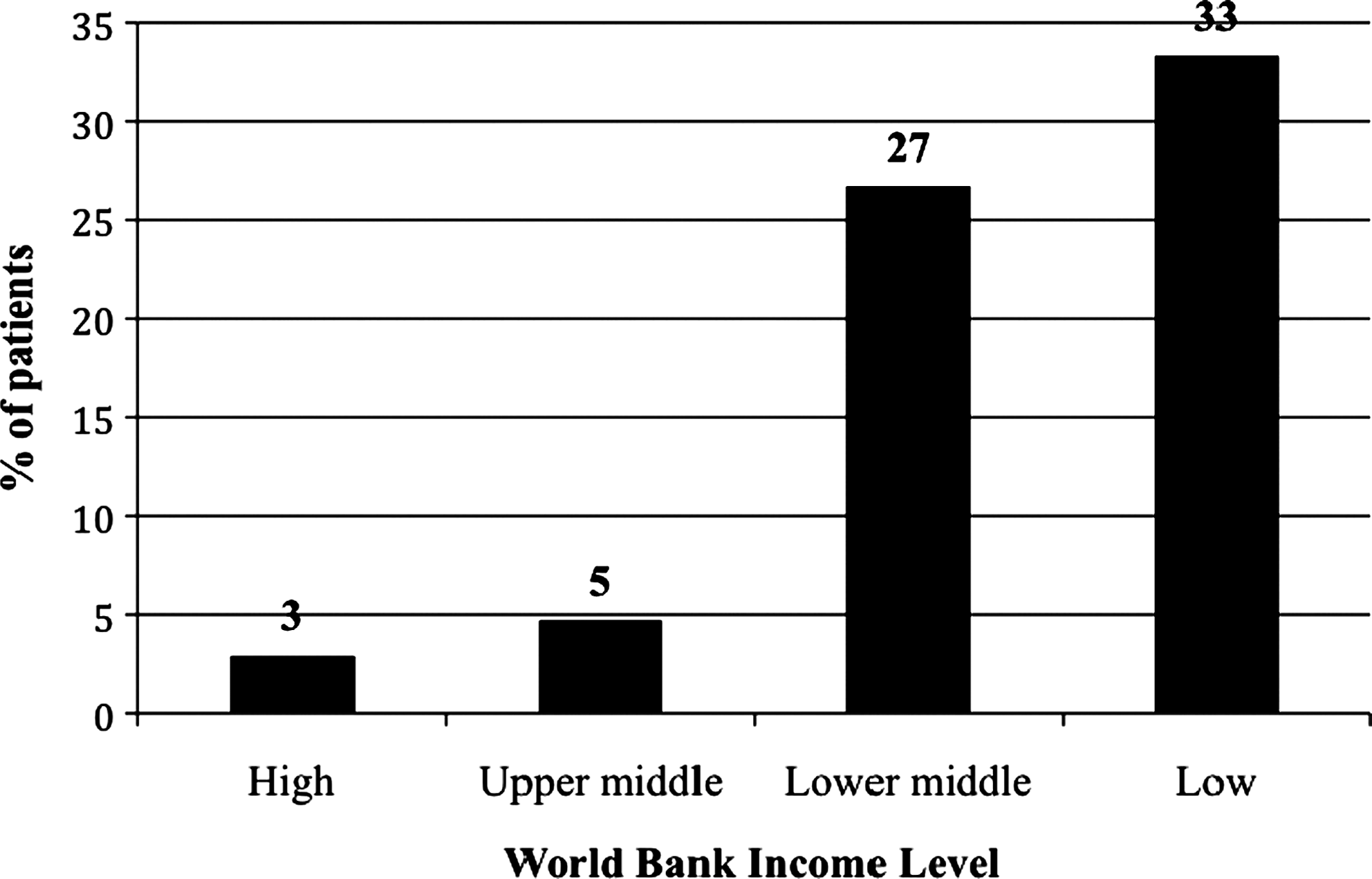
The percent of patients with invasive disease among travel-associated Salmonella infections reported to FoodNet from 2004 to 2008, by World Bank income level (n=1680).
There were also 15 or more cases of salmonellosis reported to FoodNet in travelers to the following countries: Nigeria (n=25), Spain (n=25), Canada (n=20), Ghana (n=19), Italy (n=17), Vietnam (n=17), and Ethiopia (n=16).
The Latin America/Caribbean region includes Mexico.
Proportions of travelers hospitalized and with invasive disease were analyzed by region and travel destination. By region, of the 12 travelers returning from Africa with a typhoidal Salmonella infection, 10 (83%) were hospitalized, whereas 26 (27%) of 95 travelers with a nontyphoidal Salmonella infection were hospitalized. Of 113 travelers returning from Asia with a typhoidal Salmonella infection, 70 (62%) were hospitalized, whereas 34 (15%) of 229 travelers with a nontyphoidal Salmonella infection were hospitalized. All seven travelers (100%) returning from Latin America and the Caribbean region with a typhoidal infection were hospitalized, whereas 118 (12%) of 998 travelers with a nontyphoidal infection were hospitalized. By country, of the 143 travelers returning from India with Salmonella infection, 80 (56%) had invasive disease. Of the 28 returning from Pakistan with Salmonella infection, 16 (57%) had invasive disease (Table 2). In contrast, none of the 46 cases in returning travelers from China and 35 cases in returning travelers from the Bahamas was invasive. The total number of deaths among travelers and nontravelers (2 and 71, respectively, or 0.3% of reports) was too small to analyze any differences in mortality.
Salmonella serotype data were available for 94% of the cases, with 515 unique serotypes isolated. The four most commonly reported serotypes, regardless of travel status, were Enteritidis (19% of cases), Typhimurium (14%), Newport (9%), and Javiana (5%). Among travelers, the most common serotypes reported were Enteritidis (35%), Typhimurium (8%), and Typhi (7%), whereas among nontravelers the most common serotypes were Typhimurium (19%), Enteritidis (17%), and Newport (9%) (Table 3). Four serotypes were reported primarily in travelers: Corvallis (11 of 14 isolates, 79%), Paratyphi A (78 of 108, 72%), Concord (13 of 18, 72%), and Typhi (190 of 280, 68%). Of the 46 case-patients with travel-associated serotype Paratyphi A infection and a known travel destination, 42 (91%) had traveled to the Indian subcontinent (34 to India, 5 to Pakistan, and 3 to Bangladesh). Of the eight case-patients with travel-associated serotype Concord infection and a known travel destination, all had traveled to Ethiopia.
By region, Salmonella Typhi was most commonly isolated from travelers returning from Asia (21% of infections in travelers to this region) and Africa (15% of infections in travelers to this region) (Table 4). In contrast, serotype Enteritidis was particularly common in travelers to Europe (69% of infections in travelers to this region) and Latin America and the Caribbean (44% of infections in travelers to this region) (Table 4). By country, travelers to India, Pakistan, and Ghana accounted for 70% of the total serotype Typhi cases in travelers. Certain serotypes were only found in returning travelers from one or two of the most commonly reported travel destinations. For instance, 11 (32%) of the 35 cases in returning travelers from the Bahamas were caused by serotype Braenderup, whereas 9 (28%) of the 32 cases in travelers to Thailand and 9 (28%) of the 32 cases in travelers to the Philippines were caused by serotype Stanley (Table 4). These serotypes caused <5% of cases in returning travelers from the other common destinations.
No other serotypes were associated with >1 case.
Discussion
We describe important differences in the demographics, clinical characteristics, and serotype distribution of Salmonella infections acquired by travelers to different destination countries. Travel-associated Salmonella infections were most commonly reported from travelers to lower-income countries with lower-income levels, and infections in travelers to lower-income countries were more likely to result in hospitalization and invasive disease. Our data include Salmonella infections diagnosed after travelers returned to the United States, which is likely an underestimate of the true burden of travel-associated Salmonella infections as many travelers may seek medical care while abroad or may have a self-limiting illness that resolves by the time they return from their travels. These findings are relevant both to pretravel preparation, including typhoid fever vaccination, and to post-travel clinical evaluation of gastroenteritis and febrile illness.
Of culture-confirmed Salmonella infections reported to FoodNet from 2004 to 2008 for which the travel status was known, 11% were associated with travel outside the United States. According to 2008 data from the U.S. Office of Travel and Tourism Industries, 92% of U.S. travelers traveled with adults only, whereas 8% traveled with children (USDOC, 2008). While the mean age of U.S. travelers is 44.5 years (USDOC, 2008), travelers with Salmonella infection in our study were generally younger than this, perhaps reflecting a tendency for younger travelers to visit destinations associated with high Salmonella incidence, to practice behaviors that increase their risk for infection, or both. Our findings that travelers were more likely to be Asian and less likely to be black and that travelers tended to be older than nontravelers likely reflect the demographics of international travelers, that is, those more likely to travel and therefore to be exposed to Salmonella, not those more susceptible to Salmonella infection given exposure.
Our finding that travelers were less likely to be hospitalized than nontravelers may seem counterintuitive, as the cases in travelers reported to FoodNet more frequently involved invasive serotypes that often require hospitalization. However, this may reflect that travelers tend to be a healthier subset of the population, and that they are less likely to be at the extremes of age, which are the populations most susceptible to Salmonella infection requiring hospitalization. Other differences we observed between travelers and nontravelers could have been due to differences in care seeking in these two groups, as well as the possibility that clinicians may have a higher index of suspicion for salmonellosis and a lower threshold for stool or blood culture when evaluating a patient with a “suggestive travel history” (CDC, 2001).
Our finding that invasive infections were reported more than twice as frequently in travelers than in nontravelers is driven by the fact that nearly all Salmonella Typhi and Paratyphi A cases were invasive, and these serotypes were more frequently reported in travelers. We also found that travelers to low- and middle-income countries were more likely than those who had traveled to high- and upper-middle-income countries to have invasive disease, and there was a large difference in the percent of travelers with invasive disease who had returned from upper-middle-income countries versus lower-middle-income countries.
Our result that different serotypes (e.g., Corvallis, Paratyphi A, Concord, and Typhi) occurred primarily in travelers may be due to specific geographic links. For instance, multidrug-resistant strains of Salmonella Concord have been identified among Ethiopian adoptees and their caretakers in the United States (Henriksen et al., 2009). Most patients with Salmonella Typhi infection had traveled internationally, including 70% of those to India, Pakistan, or Ghana, which is consistent with other studies (Steinberg et al., 2004; Connor and Schwartz, 2005; Lynch et al., 2009) and supports current recommendations for vaccination of travelers to developing countries (Davis and Snider, 1994). Among travel-associated cases, the global distribution of serotypes in our study was very similar to the worldwide distribution reported by the WHO Global Foodborne Infections Network. Therefore, it appears that travelers to overseas destinations tend to acquire Salmonella infections with the predominant serotypes in that country or region of the world. Data on the serotype or the recent travel destination of a person with Salmonella infection may help piece together an epidemiological investigation and identify a potential source of exposure for that individual or a group of individuals in a cluster. As certain serotypes are rare in the United States, identification of infections with such serotypes may prompt further investigation of a travel history or contact with someone who has recently traveled.
This study had several limitations. Despite attempts to complete missing records, complete data were missing for several variables, including travel destination, travel status, and clinical characteristics of some case-patients. Patients without reported travel status were the same as those with reported travel status with regard to gender but were slightly younger (median age 19 years). More than half of missing records were from a single FoodNet site; if we removed this site from the analysis, the findings did not change. Similarly, if we did the analysis including all cases with unknown travel status as “no travel,” our conclusions did not change.
Because the World Bank List of Economies is a composite index of development, countries within a given category may have quite different standards of food safety, water quality, sanitation—and risk of salmonellosis. We excluded the 3% of persons who had traveled to multiple destinations, but we do not know whether travel to multiple destinations was underreported. Although FoodNet serves as a sentinel surveillance system for the nation, FoodNet data may not be representative of the U.S. population as a whole. Studies of the demographic composition of FoodNet surveillance areas have shown that the FoodNet population is similar to the general population in terms of age and sex, but that Hispanic persons and those living below the poverty line are somewhat underrepresented in the FoodNet sites (Hardnett et al., 2004). We could not calculate risk or crude incidence of Salmonella infection by travel destination because we lacked a robust denominator of travelers from FoodNet surveillance areas. Finally, we could not examine travel behaviors such as duration or purpose of travel, pretravel typhoid fever vaccination, activities and lodging during travel, or possible source of exposure because FoodNet does not collect those data. Therefore, individual risk is not calculable for this type of study, and due to differences in many factors, including uptake of pretravel counseling (LaRocque et al., 2010), it is also not homogenous for the travelling population, even to the same destination.
Conclusions
We described travel-associated Salmonella infections reported in FoodNet sites. Expending collection of travel-specific data (e.g., travel behaviors, typhoid fever vaccination status) through FoodNet or through collaboration with other surveillance networks that evaluate illness in returning travelers (e.g., GeoSentinel) has both clinical and public health relevance and would provide valuable insight into the optimal prevention and management of Salmonella infection in travelers. Such data could help clinicians more effectively counsel travelers on reducing their risk of Salmonella exposure, including advising on pretravel typhoid fever vaccination and antibiotics for self-treatment during travel, and recognizing the often-nonspecific signs and symptoms of typhoid fever. Clinicians should maintain a high index of suspicion for Salmonella infection in patients with diarrhea or fever who have recently traveled internationally, particularly to Asia, Africa, or Latin America. Astute clinicians who ask patients with gastrointestinal complaints or fever about recent travel may have lower thresholds for stool culture or hospitalization for supportive care if the patient has recently returned from a destination or region that was associated with higher proportion of invasive disease. Although clinicians are unlikely to receive timely information on a patient's infecting serotype, a better understanding of the global epidemiology of Salmonella infections could strengthen epidemiological investigations of sporadic cases and outbreaks involving serotypes uncommonly found in the United States.
Footnotes
Acknowledgments
FoodNet Travel Working Group Members at the CDC, the U.S. Department of Agriculture's Food Safety and Inspection Service, the U.S. Food and Drug Administration, and the 10 FoodNet sites (California, Colorado, Connecticut, Georgia, Maryland, Minnesota, New Mexico, New York, Oregon, and Tennessee). Pauline Han from CDC's Division of Global Migration and Quarantine, Travelers' Health Branch, for assistance with traveler data. This work was financially supported by Centers for Disease Control and Prevention, U.S. Department of Agriculture's Food Safety and Inspection Service, and the U.S. Food and Drug Administration.
Disclosure Statement
All authors: no conflicts of interest.