
Abstract
Trichinella sp. larvae are released from the intestine and usually migrate through the liver into the general circulation. Nevertheless, hepatic involvement does not represent a leading feature of human trichinellosis. This narrative systematic review focuses exclusively on hepatic complications of trichinellosis and includes a brief overview and analysis of selected cases reported in the literature. Our major goals were to gather important data to understand the substrate of trichinous liver injury and to provide helpful clinical hints for practitioners. To our knowledge, this is the first international review dedicated to this topic. Thirty two cases were detailed enough to allow pooled analysis. The mean age of the analyzed group was 30.5±17 years old with most cases aged 19 to 29 years (29%). Hepatomegaly was noticed in 34.4% of cases, hypoalbuminemia in 40.6%, and hypoproteinemia in 34.4%. Our systematic analyses demonstrated that hepatic complications were mainly evidenced in fatal cases of trichinellosis (65.6%). The most frequent necroptic findings were parenchymatous and/or fatty degeneration of the liver (59.4%). Although less discussed in the literature than other complications, hepatic involvement should be considered more carefully because of its significant consequences on protein metabolism and liver function. Difficult to be revealed intra vitam, hepatic involvement may represent an additional concern to the classical clinical picture of trichinellosis and other life-threatening complications, especially in severe cases of infection. Consequently, physicians should be aware of any possible liver involvement to ensure adequate management of their patients.
Introduction
Trichinella sp. newborn larvae (NBL) are released from the intestine and generally migrate through the liver (hepatic portal vein) into the general circulation (Wang and Bell, 1986; Wang, 1997). In the liver, trichinae penetrate the sinusoids and may produce inflammatory mesenchymal reactions with consequent abundance of liver granulomas (Kuntz and Kuntz, 2006). Nevertheless, hepatic involvement does not represent a leading feature of human trichinellosis (Murrell and Bruschi, 1994).
This narrative systematic review focuses exclusively on hepatic involvement of trichinellosis and includes a brief overview and analysis of selected cases reported in the literature. Our major goals were to gather important data to understand the substrate of trichinous liver injury and to provide helpful clinical hints for practitioners. To our knowledge, this is the first international review dedicated to this topic. The work was all the more necessary, as most of the textbooks/treatise chapters and reviews focused on trichinellosis do not mention these possible complications.
Pathogenesis
Liver alterations were noticed either during or after the intestinal phase of trichinellosis (Lupascu et al., 1970). The lesions may be caused by direct larval injuries or indirectly (e.g., through eosinophils or immunologic reactions) (Neghina et al., 2010).
During severe infections, significant modifications may occur in the liver. Some of them were attributed to the toxic and allergic mechanisms (Guattery et al., 1956; Lupascu et al., 1970; Zanc, 2001). Liver, frequently enlarged in these cases, is generally subjected to dystrophic lesions such as fatty degeneration. Hypoproteinemia occurs commonly and may be explained by the hepatocellular dysfunction, allergic capilaropathy (induced by eosinophils), and deficitary digestion and absorption of the proteins consequent to the alterations of the intestinal mucosa (Kushlan, 1953; Zanc, 2001). Total protein decrease is based on the decrease of the albumin fraction (hypoalbuminemia). Moreover, increase of the globulin fraction leads to a significant decrease of the albumin globulin (A/G) ratio (Lupascu et al., 1970).
After the systemic dissemination of the parasites, besides their localization in the skeletal muscle, the larvae may also locate in other tissues and organs (central nervous system, heart, eyes, liver, and lungs) where they cannot continue their evolution and generally cannot encyst but, on the contrary, are destroyed. Their lysis leads to the release of increased amounts of structural antigens that cause hyperergy. Consequently, this allergic mechanism facilitates the development of extensive systemic pathologic modifications consisting of local inflammatory reactions and necroses. Moreover, the destruction of the larvae is accompanied by lesions of tissues and organs (mentioned above) and release into the circulation of modified self-proteins. Such altered proteins act as autoantigens and lead to autoantibody production. Therefore, autoimmune phenomena may play an important role in the pathogenesis of trichinellosis (Zanc, 2001). This hypothesis was also supported by the association between trichinellosis and allergic conditions such as periarteritis (polyarteritis) nodosa (Reimann et al., 1943; Frayha, 1981).
According to Guattery et al. (1956), inadequate nutrition, generally exacerbated by persistent gastrointestinal symptoms such as vomiting and diarrhea, may also trigger liver damage.
Pathology
Early findings of hepatic involvement in trichinellosis were reported by Cohnheim (1865), who noticed an enlargement of the liver similarly to the yellowish fatty degeneration occurring in phosphorus poisoning. Since that time, fatty degeneration has been often detected (Van Cott and Lintz, 1914; Cummins and Carson, 1916; Hassin and Diamond, 1926; Horlick and Bicknell, 1929; McDonald and Waddell, 1929; Pund and Mosteller, 1934; Most and Abeles, 1937; Terry and Work, 1940; Houston and Ross, 1941; McCabe and Zatuchni, 1951; Guattery et al., 1956; Ozere et al., 1962; Bell and Murphy, 1967; Andy et al., 1977). However, such alterations were not commonly found during necropsies or in experimentally infected animals (Askanazy, 1895; Gould, 1945; Lupascu et al., 1970). Frothingham (1906) evidenced, probably for the first time, the presence of the parasitic larvae in the liver sinusoids. Busila et al. (1960) considered that hepatomegaly in the late stages of trichinellosis was produced both directly (after remission of gastrointestinal symptoms) and indirectly through cardiac failure (liver blood stasis). It has also been speculated on the late development of hepatic cirrhosis subsequent to hepatocyte dystrophy. Generally, it was considered that the hepatic alterations occurring during late trichinellosis are less pronounced than those developed in phosphorus poisoning (Lupascu et al., 1970).
After their experience on human and veterinary cases, completed by experimental research on laboratory animals, Lupascu et al. (1970) described the pathologic modifications of the liver during different phases of trichinellosis (Table 1). According to their opinion, the liver may exhibit various lesions depending on the severity of the illness. Thus, the most severe hepatic alterations occurred especially in cases with peritonitis. The extremely soft consistency of the liver was considered a macroscopic index of its parenchymatous alteration.
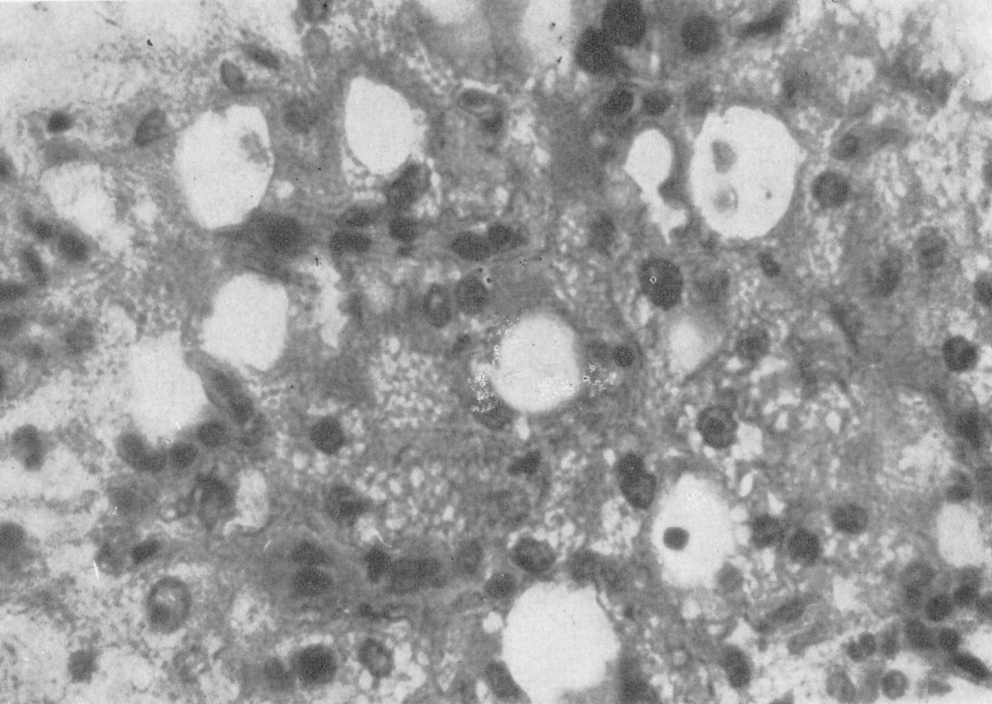
Liver: Fatty liver degeneration with vacuolation and nuclear modifications (anisokariosis and pyknosis). Hematoxylin and eosin (HE) stain; magnification×400. Sudanophilia was positive. Reproduced from Lupascu et al. (1970) courtesy to the Romanian Academy's Publishing House, Bucharest, Romania (EAR, Editura Academiei Romane Bucuresti).
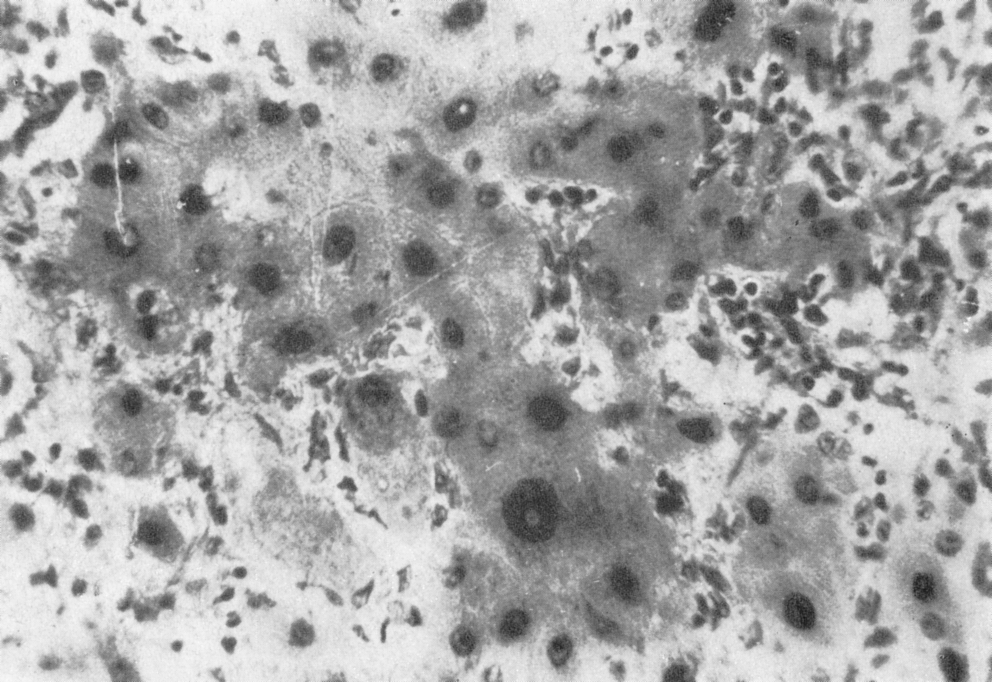
Liver: Inflammatory infiltrate of lymphocytes (various density); Hepatocellular dystrophic alterations with pronounced anisokariosis and nuclear pyknosis. Hematoxylin and eosin (HE) stain; magnification×400. Reproduced from Lupascu et al. (1970) courtesy to the Romanian Academy's Publishing House, Bucharest, Romania (EAR, Editura Academiei Romane Bucuresti).
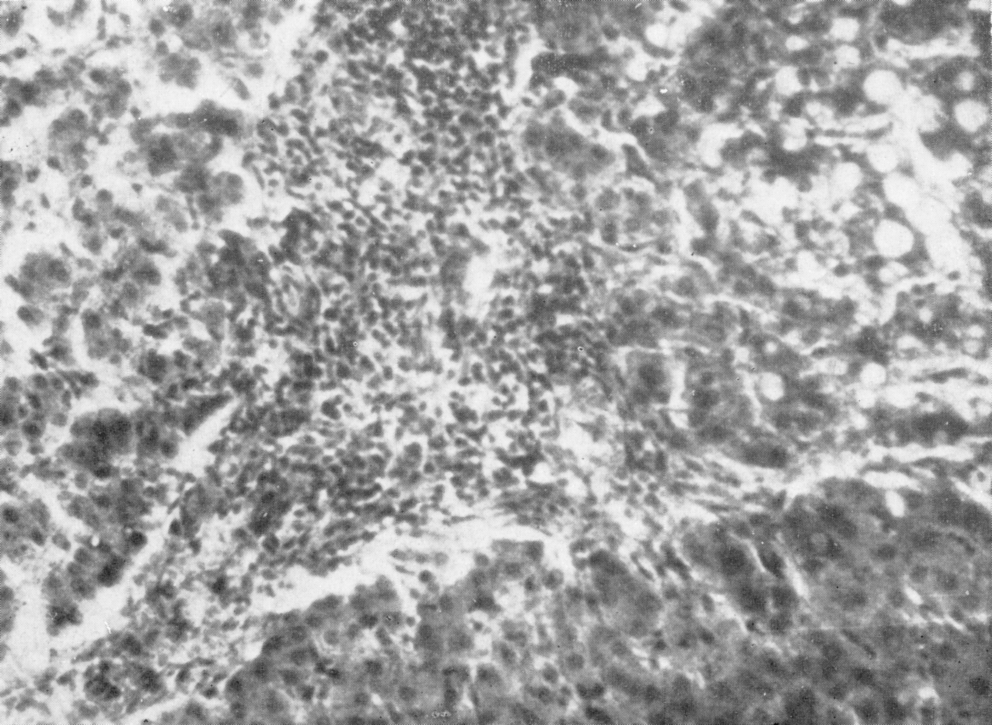
Liver: Lymphocytic inflammatory infiltrate; hepatocellular fatty degeneration in different areas of the parenchyma. Hematoxylin and eosin (HE) stain; magnification×200. Reproduced from Lupascu et al. (1970) courtesy to the Romanian Academy's Publishing House, Bucharest, Romania (EAR, Editura Academiei Romane Bucuresti).
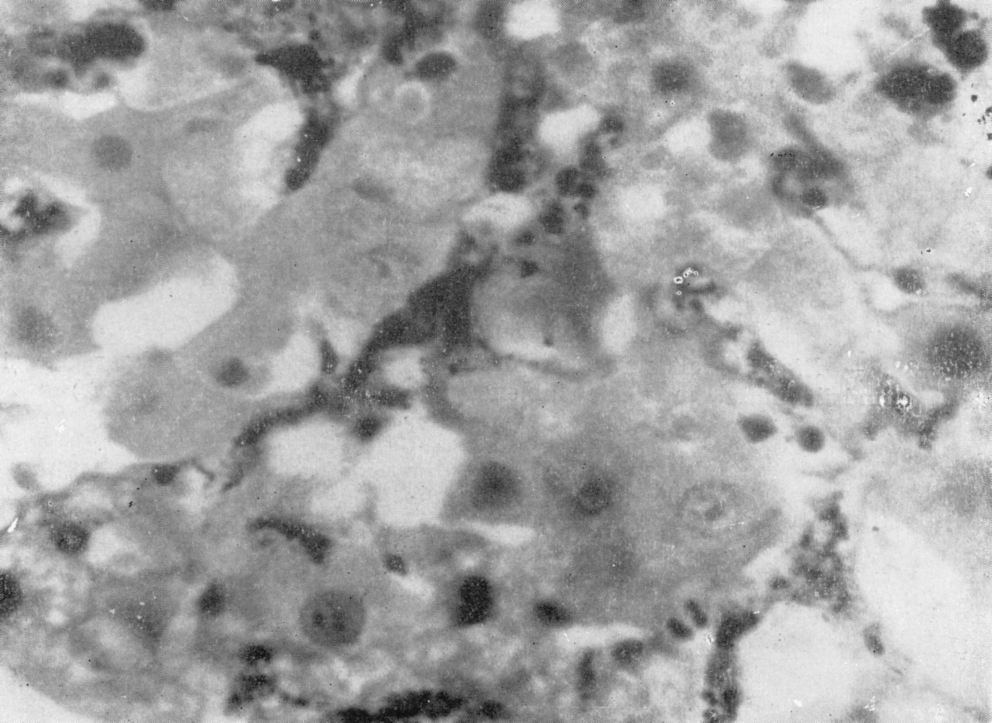
Liver: Hepatocellular alterations (vacuolation); Kupffer cell hyperplasia. China ink injection; magnification×400. Reproduced from Lupascu et al. (1970) courtesy to the Romanian Academy's Publishing House, Bucharest, Romania (EAR, Editura Academiei Romane Bucuresti).
The most relevant and interesting studies regarding hepatic alterations in experimental trichinellosis (Mikhail et al., 1978; Wang and Bell, 1986; Reina et al., 1989; Martinez et al., 1999; Reina et al., 2000; Bliss et al., 2003; Bliss et al., 2007; Douglas et al., 2010) are briefly overviewed in Supplementary Table S1 (Supplementary Data are available online at
Diagnosis
Jaundice (extremely rare) and hepatomegaly are the clinical signs that indicate hepatic involvement in trichinellosis (Guattery et al., 1956; Mikhail et al., 1978).
Liver function may be assessed by different laboratory tests, of which detection of total protein, albumin, and globulin in serum is of major importance in trichinellois. In case of liver involvement, the results may generally indicate hypoproteinemia, hypoalbuminemia, and increase of alpha-1 and alpha-2 globulins. Serum transaminases (alanine transaminase [ALT] and aspartate transaminase [AST]) may also be increased in some cases; therefore, these tests should be always performed (Ozere et al., 1962; Zanc, 2001). Detection of abnormal coagulation test results could also be relevant.
In an extensive study on 200 patients with trichinellosis, Rachon et al. (1968) found that total serum proteins (especially albumin) registered the lowest values during the fourth and the fifth week of illness, being directly related to the severity of infection. Moreover, gamma globulins also increased simultaneously with abnormal thymol turbidity—a test considered in the past as an efficient liver function indicator.
Overview and Analysis of Cases/Cluster of Cases Reported in the Literature
Methods
A literature search was initially performed in PubMed, Embase, and ISI Web of Knowledge databases using as keywords the association of the following terms: “trichinellosis OR trichinosis OR Trichinella” and “hepatic OR liver.” Additionally, we searched the online archives of several international journals with a long tradition and relevant books dealing with this parasitic condition. Bibliographies of related works were assessed for appropriate data.
Statistical evaluation was performed using the software package SPSS version 17.0 for Windows (SPSS Inc., Chicago, IL). Descriptive statistics (percentage, mean, and standard deviation) were calculated for each variable as appropriate. Comparisons between patient groups were made by means of standard binomial tests for differences in proportions and Mann-Whitney U statistics for quantitative data. A p-value of less than 0.05 was regarded as statistically significant.
Results
Cases are overviewed in the Supplementary Table S2. Emphasis was given to demographic and epidemiological characteristics (sex, age, profession, source of infection, and country), hepatic abnormal findings, relevant laboratory parameters, and patient outcome.
Thirty two cases were detailed enough (in terms of sex, age, clinical characteristics, routine laboratory parameters, outcome, and necropsy findings) to allow pooled analysis (Table 2).
Percent of the total number of patients for whom data were available (32 cases unless otherwise specified); breported in 31 cases; cin one male patient, the age was not specified; dbased mainly on laboratory tests that are not commonly used nowadays (e.g., thymol turbidity, bromsulfalein retention, and cephalin flocculation).
N, number of patients.
The mean age of the analyzed group was 30.5±17 years old (range 1–69) with most cases aged 19 to 29 years (29%) followed by those aged 11 to 18 years (25.8%). Adults predominated within the affected cases (71%, p<0.01).
There was no significant difference between patients' mean age with respect to their outcome (recovery: 32.2±15.7 years old, range 13–62; death: 29.6±18, range 1–69).
Patients who died had significantly lower eosinophil counts (18.2±18.5%, range 0.5–61) as compared with those who made complete recovery (45±25.4%, range 1–76, p=0.01).
Brief Discussion and Conclusion
Although less discussed in the literature than cardiac, neurological, pulmonary, and renal involvement of trichinellosis, hepatic complications should gain more importance because of their significant consequences on protein metabolism and liver function. At the same time, liver involvement may represent a helpful diagnostic clue in atypical cases of trichinellosis (Robin et al., 1960). Our systematic analyses demonstrated that hepatic complications were mainly evidenced in fatal cases of trichinellosis (65.6%) during necropsy. Since death is quite rare in trichinellosis (∼0.2%) (Pozio, 2007) and clinical and laboratory tests are not always conclusive, these complications are easily overlooked by physicians. Liver injury may occur soon after the initial larval invasion, and a long debilitating course of disease may result in irreversible liver damage (Guattery et al., 1956). Noteworthy is that the deceased patients presented significantly lower eosinophil counts than survivors. This confirms earlier observations (Meyer, 1918; Dalessio and Wolff, 1961; Neghina et al., 2010) indicating that there is usually an inverse relationship between eosinophil counts and the severity of the clinical course. Moreover, poor prognosis (and often death) was found to be associated with the absence or sudden decrease of the eosinophil rates (Pund and Mosteller, 1934; Most and Abeles, 1937; Kramer and Aita, 1972). Although some mechanisms and factors involved in the pathogenesis of trichinellosis (in general) and of hepatic alterations (in particular) were clearly described, further studies are required to fully clarify this issue.
Difficult to be revealed intra vitam, hepatic involvement may represent an additional concern to the classical clinical picture of trichinellosis and other life-threatening complications, especially in severe cases of infection with this nematode. Consequently, physicians should be aware of any possible liver involvement to ensure adequate management of their patients.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.