
Abstract
An outbreak of gastrointestinal illness was identified among attendees at a large community barbeque at a Sydney sports club on 30 January 2009. A retrospective cohort study was initiated, and attendees were identified through hospital emergency department gastroenteritis presentations, snowball recruitment through known cases, responders to linguistically specific press, and those returning to the venue the next week. A symptom and food history was collected from attendees, and stool samples were provided for microbiological investigation. An environmental investigation and trace back of implicated foods was also undertaken. Attendance estimates at the barbeque ranged from 100 to 180, and the food was prepared by a family that was not registered as a food business. Seventy one of the 87 attendees identified met the case definition. Thirty attendees (42%) had laboratory confirmed Salmonella Typhimurium phage-type 108/170, all with the same multilocus variable number of tandem repeat analysis typing. Burden of illness was high with 76% of cases seeking medical attention and 18% admitted to hospital. Microbiological evidence confirmed that a number of food items were contaminated with Salmonella Typhimurium 108/170, with the raw egg mayonnaise used in a Russian salad being the most likely primary food vehicle (adjusted odds ratio=10.3 [95% confidence interval 1.79–59.5]). Further, having Russian salad on the plate even if it was not consumed increased the relative risk of illness, thus suggesting that other food items may have been contaminated when they came into contact with it on the plate. This Salmonella outbreak highlighted the risks associated with the improper handling of food in private residences, which are then sold at a large public event.
Introduction
Materials and Methods
Epidemiological investigation
A retrospective cohort study was undertaken. A suspected case was defined as a person who consumed a meal purchased at the barbeque on Friday, 30 January 2009 and subsequently developed diarrhea and one or more of nausea, vomiting, abdominal cramps, fever, joint pains, or headache. A case was confirmed if Salmonella enterica Typhimurium (Salmonella Typhimurium) was isolated from a stool sample.
Since there was no sign-in process for those who attended the barbeque, several methods were used to identify and contact attendees. Active case finding was undertaken by alerting hospital EDs and General Practitioners in the SESI and SSW regions of the outbreak and asking them to notify the PHU of cases of gastroenteritis in attendees. The Public Health Real-time Emergency Department Surveillance System (Muscatello et al., 2005) was also used to detect suspected cases in all metropolitan EDs. An advertisement was placed in the Spanish media, and a notice was displayed at the club asking anyone returning to the club who had attended the event to contact the PHU whether they were ill or not. Finally, all attendees were asked when interviewed to provide contact details for people they knew who attended the barbeque to increase cohort ascertainment.
A standard questionnaire was used to conduct telephone interviews with people who had attended the event. Information collected included demographics, food history, and the illness profile (onset time and date, duration, nature of symptoms) of suspected cases. A member of the outbreak investigation team was a Spanish speaker who conducted interviews for those with limited English.
Data were entered into and the univariate analysis was performed using SPSS version 17.0 (SPSS Inc., Chicago, IL). Information on all interviewed attendees was included in the analysis. Univariate risk ratios (RRs) were calculated for each food item, and the Fisher's exact test was used to determine statistical significance (p<0.05). All implicated food items from the univariate analysis were entered into a multiple logistic regression model using proc logistic in SAS version 9.1.3 (SAS Institute Inc., Cary, NC) to estimate the odds of illness for individual items adjusted for all other implicated foods.
Laboratory investigation
Stool specimens were cultured to identify the presence of any enteric pathogens. Specimens where Salmonella Typhimurium was identified were sent to the Institute of Clinical Pathology and Medical Research at Westmead Hospital, Sydney, for multiple loci variable number of tandem repeats analysis (MLVA) (Lindstedt et al., 2004; Wang et al., 2008) and to the Microbiological Diagnostic Unit at The University of Melbourne for phage typing.
Environmental investigation
The NSWFA visited the family residence of the caterers and obtained several leftover food samples as well as a cloth that was used to cover cooked barbeque meats. An initial inspection of the club was made, and while confirming that there were no leftover foods from the barbeque in storage, several swabs of the kitchen and outside the barbeque facility were obtained. The grocery store from where the eggs used to prepare the mayonnaise had been purchased was identified, and egg samples were obtained. The eggs were traced back through the supplier to the originating egg farm, which was also inspected. A range of samples and environmental swabs were obtained at the premises and submitted for Salmonella testing.
Results
Setting
The barbeque was a community gathering held every Friday evening and run by a family who provided entertainment and a selection of salads and barbequed meats. It was initially reported that all foods were prepared in the club kitchen on the night of the event. However, the environmental investigation indicated that at least some storage of the salad items had occurred before the event in the kitchen of the family's private residence. Estimates of the number of people attending the event provided by the organizing family and the club staff ranged between 100 and 180 guests.
Epidemiological investigation
A total of 87 attendees were identified; however, two confirmed cases were unable to be interviewed and excluded from the epidemiological investigation. Of the 85 interviewed attendees, 38 (45%) were men and 47 (55%) were women. The median age of the interviewed attendees was 35 years (range 1–70 years), the same as that of the cases. Seventy-one (84%) interviewed attendees met the suspected or confirmed case definition.
The incubation period was used to plot the epidemic curve for this outbreak. The epidemic curve was consistent with a point source outbreak (Fig. 1), with a median incubation period of 17 hours and a range of 4–82 hours.
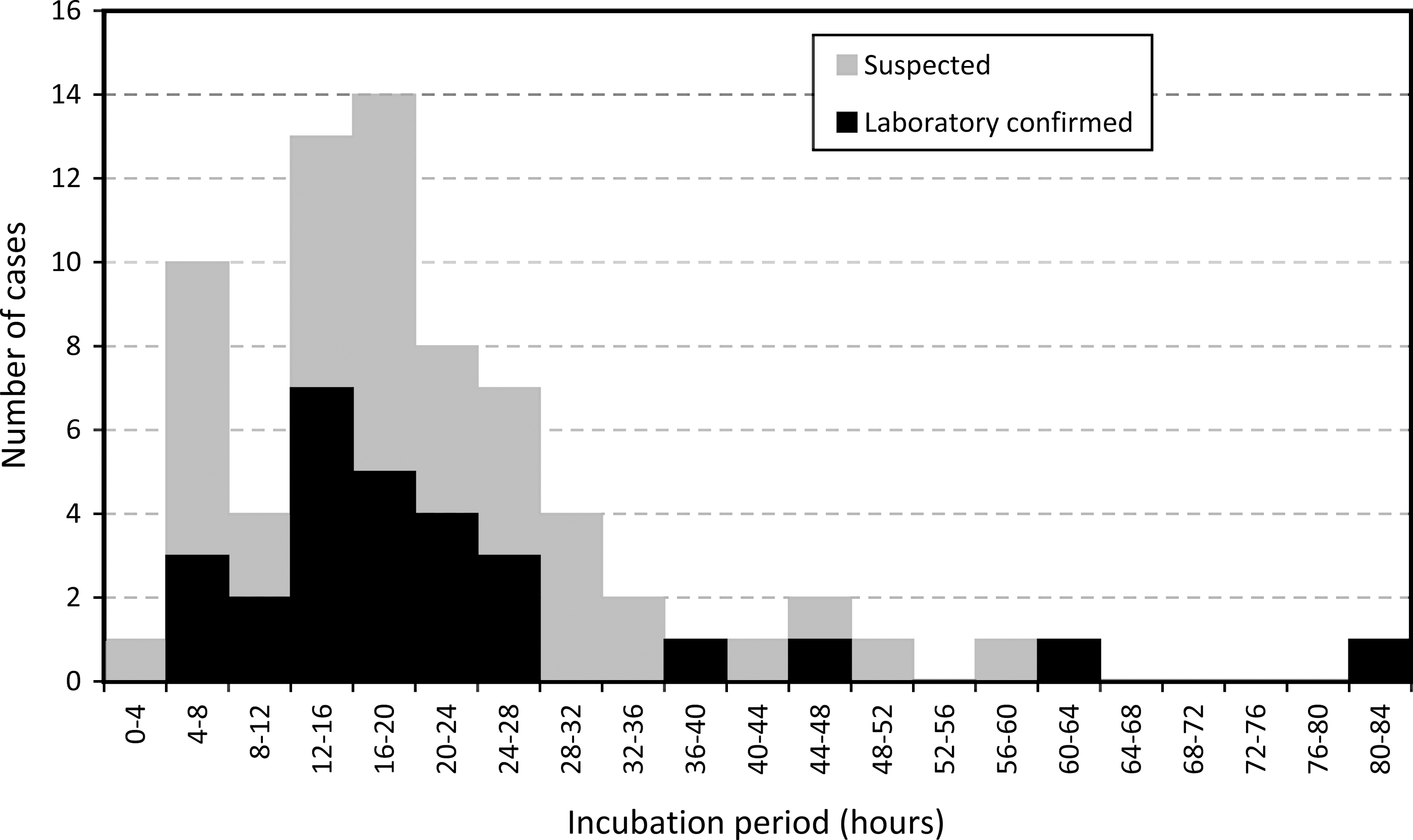
Cases of gastroenteritis (n=71), by incubation period, among attendees of a barbeque at a sports club, Sydney, January 30, 2009.
A total of 54 people (76%) sought medical attention at either a GP or a hospital, and 13 (18%) were admitted to hospital. At initial interview (1–13 days after onset of illness), 54 cases (76%) remained unwell; therefore, duration of illness could only be collected from 17 people, for whom the median duration of illness was 86 hours (range 19–230 hours). Consistent with the case definition, all interviewed suspected or confirmed cases had diarrhea, with all but one reporting that it was profuse and watery and five reporting blood in the stool. Other symptoms reported included abdominal pain (87% of cases), fever (86%), headache (80%), nausea (79%), vomiting (75%), joint pain (66%), tingling (11%), and sore throat (8%).
Food items served at the event included beef ribs, chicken, chorizo (spicy sausage) and bread, a lettuce and tomato salad, a Russian salad (potatoes, peas, and carrots in a home-made mayonnaise containing lemon, mustard, olive oil, and raw whole eggs), and small fruit and caramel-filled pastries. In the univariate analysis, illness was significantly associated with consumption of the Russian salad (RR=1.61, 95% confidence interval 1.11–2.35), and with having Russian salad (RR=2.60 [1.29–5.27]) or any salad item (RR=3.02 [1.17–7.81]) on the plate, regardless of whether it was eaten or not. A marginally increased risk of illness was also associated with consumption of iceberg lettuce (RR=1.30 [0.97–1.76]) and tomato (RR=1.24 [0.99–1.56]; Table 1).
RR, risks ratio; CI, confidence interval; exp, exposed; nonexp, nonexposed; BBQ, barbeque.
The independent effect of each item was assessed by including all food items implicated in the univariate analysis into a multiple logistic regression model (Table 2). Consuming Russian salad remained significantly associated with being a case after adjusting for lettuce and tomato consumption (odds ratio=10.3 [1.79–59.5]). Lettuce was significant in the unadjusted analysis but not in the adjusted analysis, suggesting it was not an independent risk factor.
Laboratory investigation
Of the 33 samples collected from ill attendees, Salmonella Typhimurium was detected by culture in 30 (91%). All 30 isolates had the same MLVA pattern of 3–9-8–12-523 and were all phage typed as Salmonella Typhimurium 108/170. One confirmed case was co-infected with Aeromonas species. Of the three attendees from whom Salmonella was not isolated, Blastocystis hominis (which is of uncertain pathogenicity) was identified in one case, whereas the other two samples had no pathogens detected. All three attendees from whom Salmonella was not detected remained suspected cases due to their clinical symptoms and epidemiological link to the barbeque, and were, therefore, included in the analysis.
Environmental investigation
The raw egg mayonnaise and cooked sliced potato used in the Russian salad, sliced tomato tops, whole lettuce, and the cloth used to cover the cooked barbeque meats were found to be contaminated with Salmonella Typhimurium 108/170. The raw chicken pieces were contaminated with Salmonella Sofia.
Of all of the food samples obtained at the caterer's residence that were confirmed positive for Salmonella Typhimurium 108/170, the raw egg mayonnaise was the only food that was stored in a sealed container at the time of sampling and not apparently opened after it had been made before the barbeque. However, Salmonella Typhimurium 108/170 was not detected in the eggs obtained from the caterer's residence, grocery store, or from the trace-back investigation.
The NSWFA issued an official Prohibition Order to the principal caterer prohibiting the handling of food for sale at both the family residence and at the club until issued with clearance that there was no longer a risk to public health. The NSWFA also obtained cooperation from management of the club and the local council to ensure that the club facilities were not used by the caterer or any other business until they complied with the Food Safety Standards. The NSWFA successfully prosecuted the catering business for selling food that was unsafe, failing to maintain appropriate temperature control of the food, and failing to notify the NSWFA that a food business was being carried out.
Discussion
This article describes a large outbreak of Salmonella gastroenteritis among attendees at a privately catered barbeque held at a Sydney sports club. Seventy-one cases were identified out of 85 persons interviewed; however, since a list of attendees was unavailable, the full extent of the outbreak and overall attack rate remain unknown. The median incubation period of 17 hours was within the general range for Salmonella infections of between 6 and 72 hours, most commonly 12–36 hours (Behravesh et al., 2008). The calculated median duration of illness of 86 hours is likely an underestimate of the actual duration of illness, as 21 cases were still experiencing gastrointestinal symptoms when interviewed. The burden of illness was high with 76% of those ill seeking medical attention, and 18% requiring hospitalization.
The foods potentially implicated by both the epidemiological analysis and environmental investigation were lettuce and a Russian salad consisting primarily of potato and raw egg mayonnaise. The strongest epidemiological association with illness was observed for the latter food item, and having Russian salad on the plate even if it was not eaten increased the relative risk of illness. The possibility of some other unknown initial source of Salmonella contamination cannot be ruled out, as no positive isolate was obtained from the eggs or the farm environment in the trace back investigation. However, this is not uncommon, as egg or farm environment sampling does not always provide definitive conclusions in outbreaks where raw egg products are implicated, because Salmonella may be transient in the farm environment (Sarna et al., 2002; Stephens et al., 2007; Mannes et al., 2010) and the sensitivity for laboratory testing for detecting specific pathogens in eggs is generally limited (Williams et al., 2009). The most plausible explanation remains that one or more of the egg shells used to make the mayonnaise were contaminated with poultry fecal material containing Salmonella Typhimurium 108/170, which remained in the Russian salad, as there was no cooking or “kill” step to reduce the bacterial burden before consumption.
Eggs have been implicated in multiple previous outbreaks of Salmonella Typhimurium in Australia (Hall, 2002; Sarna et al., 2002; Tribe et al., 2002; McCall et al., 2003; Stephens et al., 2007; Stephens et al., 2008; Williams et al., 2009). In 2006 and 2007 in Australia, 35 separate outbreaks of various phage types of Salmonella Typhimurium were caused by consumption of raw eggs, raw egg-containing products, or cross contamination of other foods by raw eggs (OzFoodNet Working Group, 2007, 2008). In response to this, Food Standards Australia New Zealand (2009) recently developed a draft primary production and process standard and risk assessment for eggs and egg products. The NSW Egg Food Safety Scheme also came into effect in 2010, which places specific food safety requirements on producers of eggs and egg products at the primary industry level (NSWFA, 2010a). Further, the Australian Egg Corporation Limited (2008) has developed a voluntary code of practice for the manufacture of egg products as part of a comprehensive quality assurance program. However, many outbreaks relating to raw egg products continue to occur, and ongoing discussions and investigations at the national level are required.
Although industry-based activities are important, this outbreak shows that attention should also be focused on reducing the potential for outbreaks that result from community events where caterers are not a registered business, have little or no training in food handling, and often store or prepare food in a private residence. Research has shown that food handling practices are generally poor in private residences with 99% of respondents reporting some form of improper food handling in one Australian study, including 41.7% who mishandled raw food (Mitakakis et al., 2004).
The prevalence of catering for large events by private individuals not licensed as a food business is unknown, but it is unlikely that the circumstances that lead to this outbreak are unique and such scenarios are difficult for authorities to identify until an outbreak occurs. To enhance retail standards in NSW, additional legislation was gazetted in 2010 to ensure that every business serving potentially hazardous foods has at least one person qualified as a Food Safety Supervisor (NSWFA, 2010b). This legislation would also apply to all businesses that undertake catering or other food-based activities from home.
The major epidemiological limitation of this study was the fact that a full list of attendees was not available and the proportion of the cohort interviewed was not complete. Recall bias is always a limitation in a retrospective cohort study, particularly as people who become sick may think more carefully about what they ate than those who did not. However, given the small menu and the fact that almost all interviews were conducted within a week of the barbeque, recall bias would have been minimized. Despite these limitations, the epidemiological and supporting microbiological evidence allowed the foodborne nature of the outbreak to be confirmed, and the likely food vehicle identified.
Conclusion
This outbreak implicated raw egg mayonnaise with potential cross contamination of other food items on the plate, further reinforcing the need to continue to implement best practice through the egg production and supply chain. This will help to limit, but not prevent, foodborne illness that results from privately catered events such as the barbeque in this outbreak. Ultimately, it is the responsibility of food handlers and venue owners where food is being served to ensure adequate facilities and training for large-scale food preparation and serving. Mechanisms for supporting and educating community organizations that hold events including the provision of food are needed to minimize the risk to the community. Councils may be able to play a role in monitoring venues used for community events serving food and in ensuring that caterers are registered, can provide evidence of food handling training, and prepare food in satisfactory premises.
Footnotes
Acknowledgments
The authors would like to gratefully acknowledge the assistance of Patricia Morton, Brett Campbell, and other staff from the SSW and SESI PHUs, the NSWFA, and NSW Health, who assisted in the investigation. They would also particularly like to acknowledge Darren Mayne, SESI PHU, who performed the multivariate analysis. This work was completed while AJ was a Master of Applied Epidemiology (MAE) scholar. The MAE Program was funded by the Australian Government Department of Health and Ageing.
Disclosure Statement
No competing financial interests exist.