
Abstract
Social media (i.e., internet applications and platforms that allow users to create and share content) are a potentially rich data source for foodborne disease surveillance. This commentary qualitatively evaluates social media as a foodborne disease surveillance system component and discusses novel ways that social media may facilitate the detection of intentional and unintentional food contamination.
Introduction
P
Surveillance systems specifically designed to detect foodborne disease include pathogen-specific surveillance, reports of disease clusters by healthcare providers, components of syndromic surveillance systems, and consumer-driven complaint-based systems (CIFOR, 2009; Balter et al., 2005; Buehler et al., 2009; CDC, 2011a). The need for improved foodborne disease surveillance is underscored by recent high-profile foodborne outbreaks and the estimated 48 million foodborne disease occurrences each year (Scallan et al., 2011a,b; CDC, 2006, 2009, 2011b; ECDPC, 2011). Early detection of both unintentionally and intentionally caused foodborne disease outbreaks (i.e., outbreaks associated with food safety issues or food terrorism acts, respectively) offers potentially significant targets for effective public health intervention (Khan et al., 2001). Modeling studies have estimated that early outbreak detection of terrorism events involving food result in reduced morbidity and mortality (Hartnett et al., 2009; Wein and Lui, 2005). Rapid detection of these events can reduce the number of exposed individuals via contaminated product removal from retail and food service outlets, public notification and education, and a more timely dissemination of preventative and therapeutic measures to exposed individuals.
A successful collaboration between local, state, federal, and private entities could facilitate the creation of a surveillance system that mines social media data for signals of foodborne disease activity. Additionally, data gleaned from social media (i.e., web forum postings, microblog updates, and search engine queries) may be useful in disease outbreak tracking and documentation (Wethington and Bartlett, 2004; Brownstein et al., 2009; Chew and Eysenbach, 2010; Corley et al., 2010; Ginsberg et al., 2009; Hulth et al., 2009; Howland and Conover, 2011; Stuart Chester et al., 2011; Signorini et al., 2011). In 2007, a web forum of mountain bikers assisted public health authorities in detecting a Campylobacter outbreak and identifying potential outbreak transmission vehicles (Stuart Chester et al., 2011). In an analysis of Twitter© content created during the recent H1N1 pandemic, 23% of sampled H1N1 microblog updates were related to personal experience with disease (Chew and Eysenbach, 2010). The same study also found that microblog updates sharing personal experience about H1N1 correlated with reported H1N1 incidence rates (Chew and Eysenbach, 2010). These studies document the willingness of social media users to publicize personal health conditions, therefore providing a potential opportunity for public health surveillance and response. Given the potential for significant morbidity of an outbreak associated with a widely distributed food, coupled with the concern related to the ease of intentional food contamination, efforts to augment foodborne disease surveillance systems are warranted (Hennessy et al., 1996; Khan et al., 2001; Sobel et al., 2002).
The objective of this commentary is to examine the potential capability of social media to augment and improve current food safety and food terrorism surveillance systems.
Evaluating the Potential of Social Media as a Component of Foodborne Disease Surveillance
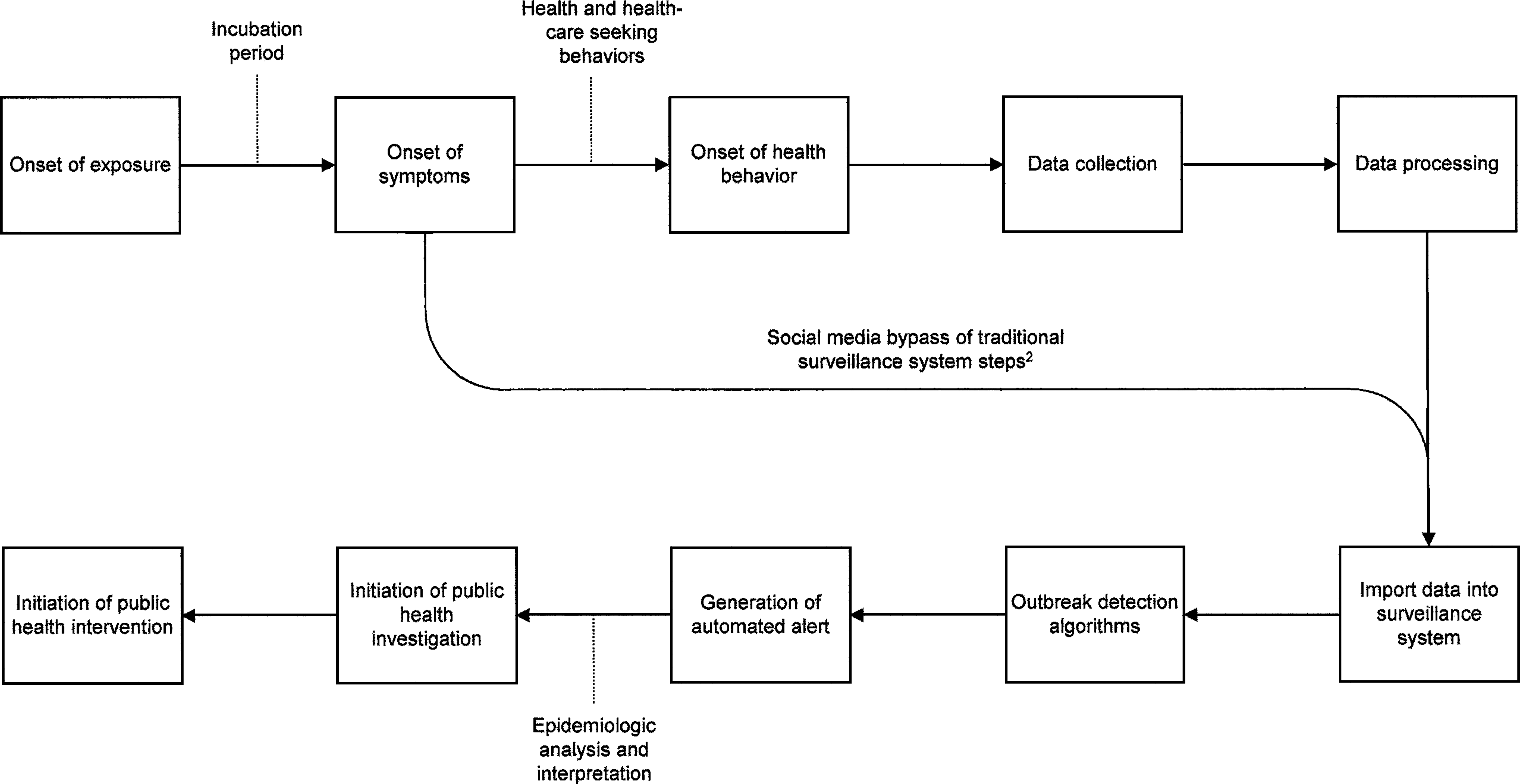
Table 1 provides a qualitative analysis of the capacity of social media to be used as a component in a foodborne outbreak surveillance system by juxtaposing social media data characteristics and the Centers for Disease Control and Prevention (CDC) Working Group framework for evaluating public heath surveillance systems for early outbreak detection (Buehler et al., 2004). As described in Table 1, a major advantage of including social media as a surveillance system component is timeliness. Traditional foodborne disease surveillance modalities rely on health seeking behavior, sample collection, laboratory testing, and reporting. Social media data can potentially be collected and analyzed in real time, and can potentially bypass important delays inherent in other foodborne disease surveillance activities (Fig. 1). In 2011, the Illinois Department of Health reported that foodborne outbreak questionnaires distributed via Facebook©, a large social media network, were completed significantly faster than questionnaires distributed via email (8.7 vs. 42.3 h, respectively; p-value<0.05) (Howland and Conover, 2011). When assessing timeliness for enteric disease surveillance, Hedberg et al reported a median delay of 6.5 days between case report from clinicians to the health departments (Hedberg et al., 2008). For outbreaks with known etiology, the median number of days from symptom onset to outbreak detection was 1–16 days, with bacterial toxins and Salmonella representing the extremes of that range (Hedberg et al., 2008). Given that the majority of health departments report delayed notification as a barrier to investigating foodborne disease, reducing the delay between symptom onset to outbreak detection is critical for health department response (Hoffman et al., 2005).
Foodborne surveillance systems may also benefit from the inclusion of social media data due to the potential representativeness of its user-base and/or access to potential cases. The potential representativeness of many foodborne disease surveillance systems is poor given the multiple barriers for foodborne disease data collection and reporting. This is often represented by the “iceberg” effect, in that very few cases are identified and reported to public health authorities. In an important finding, Li et al. (2010) reported that 81% of complainants who utilized a complaint-based system to report expected foodborne disease did not seek medical attention, which potentially precludes complainants from entering into the more traditional components of a foodborne disease surveillance system. However, this study also suggested that individuals are willing to seek alternative routes for foodborne disease reporting. Given documentation of outbreak cases preferring internet-based surveys compared to telephone surveys, the ease of sharing social media data may contribute to a surveillance system representativeness that has not been observed to date (Ghosh et al., 2008). Furthermore, social media users can allow for potential follow-up and case characterization by providing usernames or email addresses. The size of the social media population is another important aspect that contributes to the potential representativeness for surveillance systems. For example, Facebook© reports 750 million active users, with 50% logging on to the website every day (Facebook Press Room, 2011). Such figures dwarf the reach of other foodborne disease surveillance systems; therefore, the potential representativeness of social media data is significant.
Social Media as a Catalyst for Groups to Self-Identify Foodborne Outbreaks
The key issue for foodborne outbreak detection is to identify unusual clusters of disease and then to link them to specific exposures. Members of a group can recognize a common illness and then identify the common source (Stuart Chester et al., 2011; Li et al., 2010). When a group framework is absent, complaints typically refer to the last meal eaten. Social media could increase the efficiency of groups to self-identify illnesses and common exposures. This efficiency can be via one of two mechanisms. The first relates to how individuals are positioned within a social media network. Measures of network centrality, including degrees of connectedness and positioning within the network, can be proxy measures for how information related to foodborne illnesses and exposures moves between people in networks. The second form relates to the perspective of the individual who shares foodborne illness and exposure information. For disease surveillance purposes, firsthand information related to illness or exposure is more informative than secondhand information (Corley et al., 2010). Text mining and classification algorithms could identify and weight firsthand information more than secondhand or opinion information. Highly connected individuals sharing or receiving firsthand information may facilitate the detection of potential foodborne outbreaks or intentional contamination events. Figure 2 provides an illustrative example of a small social media network, wherein Individual 1 is the most connected in terms of indegree and outdegree relationships. Foodborne illness and/or exposure information in this network is most likely to flow through Individual 1. This concentration of information may facilitate recognition of common illness and/or common exposure.

A simple social media network consisting of 11 individuals and their relationships.
Additionally, the ability of social media to organize groups by exposure could allow for the detection of intentionally or unintentionally caused outbreaks by identifying common illnesses among persons with the common exposure. This would be a novel way to expand the ability of complaint systems to identify outbreaks. For example, a social media group is formed around a preference for Food A. In situations where Food A is contaminated, group members may begin to post firsthand experience of foodborne disease. Other group members read the initial postings, have consumed Food A, notice similar signs of illness, propose an exposure-illness connection, and notify public health authorities. In this manner, groups may self-identify intentionally or unintentionally caused foodborne outbreaks based on their being organized around a common exposure.
Finally, social media could enhance pathogen-specific surveillance and subsequent data analysis, by creating opportunities to link people with the same pathogen-specific illness in ways that allow them to search for common exposures. Public health agencies could host secure online surveys or web forums where individuals with confirmed pathogen-specific illness would be invited to anonymously provide information related to foodborne disease exposures. Given limited public health funding and the reduction in cost for internet-based versus telephone-based outbreak investigations, this mechanism could facilitate outbreak recognition and response for pathogen-specific illnesses (Ghosh et al., 2008).
Conclusion
The incorporation of social media data into foodborne disease surveillance systems does have value, yet surmountable challenges exist. Methods for analyzing and interpreting social media data for indicators of intentional or unintentional foodborne disease outbreaks are not fully developed. However, components of social media–based surveillance systems could be designed to search for key words that may signal intentionally or unintentionally caused outbreaks. “Diarrhea,” “vomiting,” “fever,” and commonly used, equivalent terms may provide important early warning clues for foodborne disease outbreaks. Detection algorithms could also be calibrated to search for specific syndromes or symptoms, such as “drooping eyes” or “paralysis” for foodborne botulism. Li et al. (2010) found that complainants who mentioned two ill people (versus only mentioning oneself) and three ill people (versus only mentioning oneself) is a statistically significant predictor of a complaint leading to an outbreak detection (Li et al., 2010). Therefore, surveillance systems could be designed to not only search for key terms, but also weight terms in relevance of importance. Another important disadvantage of including social media as a surveillance system component would be low specificity and positive predictive value. The generation of false alarms, due to low specificity, can misdirect resources and reduce stakeholder use. However, a system-of-systems composition may mitigate this disadvantage if multiple surveillance components detect trends. In an effort to increase specificity and reach younger, tech savvy demographic groups, researchers have suggested that public health surveillance systems could also be designed to generate links to secured, electronic public health surveys and foodborne disease questionnaires (Chew and Eysenbach, 2010). Additionally, concerns related to privacy, potential transmission of personal health information, and associated legal issues need to be addressed. While the creation of a legal framework to address these issues is beyond the scope of this commentary, social-media end user agreements, government-industry data sharing agreements, and “opt-in/opt-out” user agreement clauses may address some concerns.
Social media cannot replace traditional public health surveillance system components. However, the incorporation of existing social media into a public health surveillance system-of-systems may enhance early foodborne disease outbreak detection. Social media may also facilitate the ability for groups to self-identify foodborne outbreaks, which would provide a novel outbreak recognition mechanism and reduce detection time. Public health surveillance efforts can potentially exploit the ability of social media to link illnesses and exposures in ways that could increase the sensitivity or timeliness of existing methods. The advantages that social media contribute to surveillance systems, namely timeliness, representativeness, and facilitation for self-identification of outbreaks, outweigh the disadvantages related to specificity and analytical methodologies. Augmenting existing surveillance systems with social media data may potentially translate into the reduction of morbidity and mortality related to food safety and intentional contamination events.
Footnotes
Disclosure Statement
No competing financial interests exist.