
Abstract
Epidemiologists have used case-control studies to investigate enteric disease outbreaks for many decades. Increasingly, case-control studies are also used to investigate risk factors for sporadic (not outbreak-associated) disease. While the same basic approach is used, there are important differences between outbreak and sporadic disease settings that need to be considered in the design and implementation of the case-control study for sporadic disease. Through the International Collaboration on Enteric Disease “Burden of Illness” Studies (the International Collaboration), we reviewed 79 case-control studies of sporadic enteric infections caused by nine pathogens that were conducted in 22 countries and published from 1990 through to 2009. We highlight important methodological and study design issues (including case definition, control selection, and exposure assessment) and discuss how approaches to the study of sporadic enteric disease have changed over the last 20 years (e.g., making use of more sensitive case definitions, databases of controls, and computer-assisted interviewing). As our understanding of sporadic enteric infections grows, methods and topics for case-control studies are expected to continue to evolve; for example, advances in understanding of the role of immunity can be used to improve control selection, the apparent protective effects of certain foods can be further explored, and case-control studies can be used to provide population-based measures of the burden of disease.
Introduction
Case-control studies are an important epidemiologic approach for attributing enteric illnesses to specific risk factors or exposures, by comparing recent exposures in populations of people with the disease of interest to those in controls who do not have the disease (Breslow et al., 1996; Batz et al., 2005; Scallan and Angulo, 2007b; Pires et al., 2009). Case-control studies are often used during enteric disease outbreak investigations, but have been increasingly used to identify risk factors for sporadic illness (Dwyer et al., 1994). While the same approach is used to investigate both outbreak and sporadic disease, there are important differences in these epidemiologic settings that need to be considered in the design of the case-control study for sporadic disease.
The aim of case-control studies of sporadic disease is to inform public health and regulatory action by identifying risk factors at a population level. Thus, they differ in scope from case-control studies in an outbreak setting, where the goal is to prevent additional illnesses, through identifying the specific common contaminated food source or other exposure. Because sporadic cases do not necessarily share a single specific common contaminated source, the epidemiologic signal from any single source is diluted, making true risk differences more difficult to detect. Even if a food type—for example eggs, spinach, or beef—is an important source of sporadic infections, most servings of that food type are not contaminated, so the odds of a patient having consumed that food type may be only modestly higher than those of a control. Case-control studies of sporadic disease often quantify the magnitude of an exposure risk through the estimation of population measures such as the population attributable fraction (PAF); the PAF is a measure of the fraction of total disease in the population under study that would not have occurred if the effect associated with the risk factor of interest were absent. Because the magnitude of risk is assessed across multiple exposures, biases in the design or conduct of the study, such as selection bias or recall bias, can greatly impact the interpretation of study findings.
The International Collaboration on Enteric Disease ”Burden of Illness” Studies (hereafter, the International Collaboration) was started in 2004 by the U.S. Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO) to foster communication among groups conducting burden of foodborne disease studies and to provide a forum for technical assistance on developing such studies (Flint et al., 2005). In 2005, a working group was established within the International Collaboration to explore the methods used to conduct case-control studies of sporadic enteric disease; the working group had representatives from nine countries (Australia, Canada, Denmark, England, France, Germany, Malta, the Netherlands, and the United States). The group reviewed sporadic case-control studies conducted in various countries from 1990 through to 2009 and discussed key methodological issues influencing their validity. We summarize the review and working group discussions here and highlight how methods have changed over time.
Literature Review and Data Extraction
Eligible studies began on or after January 1, 1990, were published in English on or before December 31, 2009, and were identified by searching PubMed and by hand-searching the reference lists of retrieved articles. For the PubMed search, we used the following search terms: ”case-control foodborne NOT outbreak” and ”case-control enteric NOT outbreak” in the Title/Abstract. The titles/abstracts of all identified studies were read to exclude those that were not relevant, typically because they did not use a case-control study design or were an outbreak investigation or animal or laboratory study. Reference lists of relevant articles were also searched to identify additional candidate studies. The full texts of relevant articles were read to determine if they met the study inclusion criteria. When multiple reports from one study were found, only the initial report was included.
A data abstraction form summarizing the study design, study population, method of exposure assessment, and analysis methods was completed for each article by one reviewer (K.E.F.) (see Supplementary Material; available online at
Study Characteristics
The initial PubMed search identified 686 possibly eligible studies. We retrieved 106 articles for full assessment, of which 79 met the eligibility criteria (Fig. 1). Studies were conducted in 22 countries: the United States (22, 28%), the United Kingdom (12, 15%), and Australia (9, 12%) (Table 1). Most studies were started between 1996 and 2002 (55, 70%), coinciding with the launch of formal surveillance networks such as FoodNet (started 1996) and OzFoodNet (started 2001), which provided platforms within which to conduct these studies; most studies (59, 75%) were published from 2001 to 2009. The median study period (defined by the number of months of case ascertainment) was 12 months (range, 1–132 months); two studies did not report study length. Nine pathogens were studied (Table 2). Four of the case-control studies were nested within larger cohort studies (Ghosh et al., 1997; Rodrigues et al., 2001; de Wit et al., 2003; Do et al., 2007).
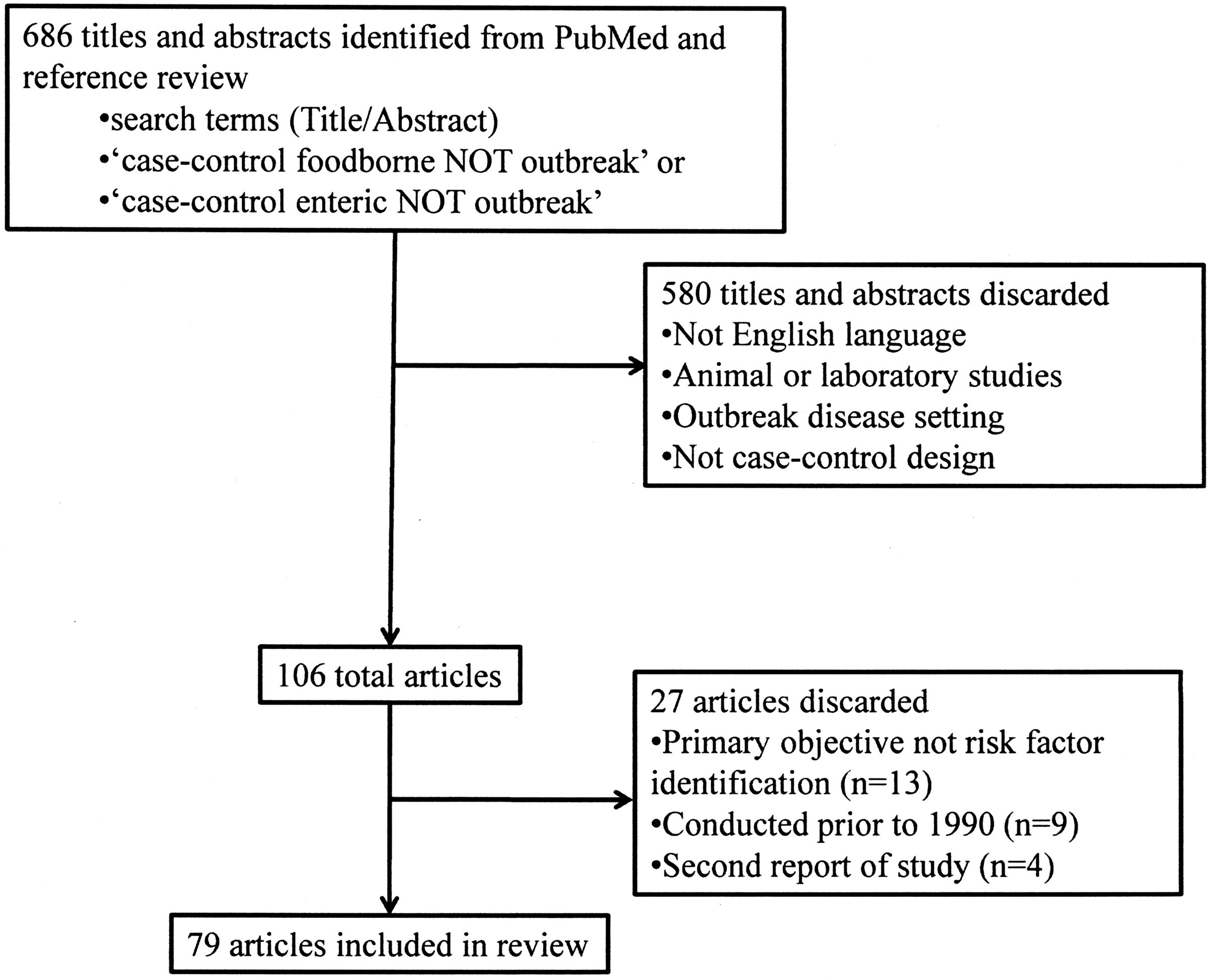
Flow chart of literature search for case-control studies of sporadic enteric infections.
The number of case-patients was 11–2,381 (median, 132 patients); the number of controls was 22–7,618 (median, 228).* Among the 59 (75%) studies reporting a case-patient response rate, the median was 68% (range, 22–100%). Among the 24 (31%) studies reporting a control response rate the median was 69% (range, 22–92%). Less than a quarter of the studies reported power calculations and calculated sample size (16% of studies) (Table 3).
Population summary measures (primarily population attributable fractions derived from the odds ratios) were reported in just over half of the studies (51%) (Table 3); most studies reporting a population attributable fraction were conducted after 1996.
Key Methodological Issues
The International Collaboration working group identified three key methodological issues considered to have the greatest influence on the validity of case-control studies of sporadic enteric disease: (1) accurate identification of cases (case definition), (2) the selection of an appropriate control group (control selection), and (3) accurate definition and measurement of the exposures of interest (exposure assessment).
Case Definition
The case definition used in case-control studies can be considered from two perspectives: the conceptual definition of a case of illness (or case-patient with that illness), which defines which case-patients are eligible for the study through the application of inclusion and exclusion criteria, and the operational task of identifying a participating case-patient, where only a subset of eligible case-patients are enrolled on account of practical, or operational, considerations. Both aspects (conceptual and operational) need to be considered when designing a study. Exclusion criteria may include things such as where the case-patient lives (to ensure that cases arose from the target population), outbreak status (to ensure that cases are not associated with an outbreak or are not secondary cases), age of the case-patient, international travel history (if the focus is on domestically acquired cases), and the presence of symptoms (case-patients who are unable to recall when their symptoms began or who do not report symptoms are typically not eligible). Once eligible case-patients are identified, operational, or practical, considerations may govern which are actually enrolled. For example, case-patients may not be enrolled because they cannot be reached (i.e., there is no phone in the home, or they do not respond to multiple call attempts); if reached, case-patients may not be enrolled because they refuse to participate or because they do not speak the language of the interviewer or questionnaire, or they may be otherwise unable to answer the questions.
Nearly all of the studies in this review (73 studies, 92%) used a laboratory-based definition of a case, requiring some level of microbiological confirmation or subtyping information; all of these studies identified cases through laboratory-based surveillance systems. Laboratory-confirmed Salmonella (24 studies, 31%) infections, including infection with specific Salmonella serotypes (17 studies), and Campylobacter infections (23 studies, 29%) were the most common infections studied (Table 2). Six studies used a symptom-based definition for diarrhea or gastroenteritis and identified cases through hospitals, clinics, or general practitioners. Unlike an outbreak where additional cases are typically identified through active case finding, there was no additional case finding in these studies beyond those cases of infection identified through surveillance systems and hospital or clinic registries. These studies are therefore subject to a differential selection bias because case-patients generally represent more severe disease than that experienced by undiagnosed and unreported case-patients (Sethi et al., 1999; Tam et al., 2003; Scallan et al., 2006). It is not known if the risk factors differ between reported and unreported case-patients.
Most studies (92%) reported the criteria used to exclude case-patients. It was common to exclude patients with secondary cases (individuals with illnesses that were associated with household clusters of illness and were not the first illness in the household); of the 42 studies that reported excluding some illnesses associated with household clusters, 37 (88%) included only the case-patient with the earliest onset of illness, sometimes referred to as the index case. It was also common to exclude cases associated with outbreaks. An alternative to excluding all outbreak-associated cases is to include only the first case in the outbreak and exclude subsequent cases, so that the exposures associated with illness in the outbreak are present in the final analysis. Of the 51 studies that explicitly excluded outbreak-associated cases, seven (14%) included the first case of the outbreak. International travel before illness was another common exclusion criterion, used in 25 studies (31%). Because international travel can itself be an important risk factor for enteric disease, the risk associated with travel can be examined by including patients reporting international travel before illness (Eberhart-Phillips et al., 1997; Kassenborg et al., 2004b; Stafford et al., 2006). Specific age groups were studied in 11 studies (14%); four studies focused on infants (Tenkate and Stafford, 2002; Rowe et al., 2004; Jones et al., 2006b; Fullerton et al., 2007).
Tracking excluded case-patients and controls, and the reason for their exclusion or loss allows for calculation of participation and response rates and determination of the adherence to predetermined criteria for participation (Fig. 2). While 92% of studies reported the criteria used to exclude case-patients, only 78% reported the criteria used to exclude controls; all of these studies used the same exclusion criteria as was used for case-patients. Over half of the studies reported the number of eligible case-patients excluded (54%), while less than 15% of studies reported the number of potential controls excluded. Flow diagrams were used to illustrate the study population in some of the studies (Varma et al., 2006, 2007; Jones et al., 2006b; Voetsch et al., 2007; Denno 2009), and their value has been recognized in the reporting of randomized controlled trials (Egger et al., 2001).

Example of flowchart that can be used to track cases enrolled in a case-control study of sporadic enteric disease, using a case-control study of Salmonella serotype Enteritidis as an example.
Control Selection
For study validity, it is important that selected controls would have had the same opportunity to be recognized as case-patients if they had been exposed and developed disease, thus they must come from the same source population and geographic area (i.e., catchment area) as the cases. The catchment area of the surveillance system from which the cases are identified should define the catchment area for the controls. In practice, this can be hard to assure, particularly where the laboratory-based surveillance systems or registries used to identify cases are not population-based (i.e., do not cover a defined catchment area.)
Controls are frequently selected from the general population. However, even when controls are selected from the same catchment area as case-patients, there is no guarantee that, had a control become ill, he or she would have sought medical care and been reported as were the case-patients. Controls may differ from case-patients who are ascertained in a laboratory-based surveillance system by factors that affect the identification process that occurred for cases to be ascertained in the surveillance system. The selection of controls from persons with another laboratory-confirmed infection ensures that case-patients and controls are similar with regard to these factors affecting identification, though it may decrease the generalizability of the study findings to the general population (McCarthy and Giesecke, 1999 and Giesecke; Wilson et al., 2008; Voetsch et al., 2009).
Almost half of the studies reviewed (36 studies, 46%) used population-based controls; the most common methods of identifying population-based controls were random or sequential digit dialing from telephone directories or registries (21 studies), and population registries (13 studies). Continued reliance on telephone-based methods of selection of controls is becoming increasingly problematic, as mobile telephones become more widely used. Most telephone directories or registries used to identify and recruit controls do not include mobile telephone numbers, and mobile telephone numbers are often not linked to the neighborhood or city in which the control lives.
The next most common source of controls was either a hospital or a clinic (17 studies, 22%). Other control sources included national- or state-based control banks (4 studies, 5%) or convenience samples (e.g., case nominated neighbors or friends; 5 studies, 6%). Ten studies (13%) used a combination of sources.
Matching
Matching was used in 69 studies (87%) in this review. Of these, 14 (20%) used frequency matching; the other 55 (80%) used individual matching. All of the studies that used matched designs reported the matching criteria used. Among the 43 studies that reported the number of matched controls per case, the average was two (range, 1–15 per case).
Matching of case-patients and controls is common and has historically been done to control confounding by the criteria on which matching is performed. It is primarily employed for study efficiency and practical considerations (Kleinbaum et al., 1982; Rothman et al., 2008). For example, matching can be used to ensure that controls come from the same source population as the cases; a common example is using sequential digit-dialing based on a case-patient's phone number for geographical matching. The advantages and disadvantages of matching should be carefully considered before a matched design is selected, as matching may decrease the investigators' ability to examine all exposures of interest. Matching can be done at either the individual or group level. When individual matching is employed and controls are questioned about the exposure window during which the case occurred, it is important to recruit and interview controls in a timely manner to reduce recall bias. With group, or frequency, matching, there is more operational flexibility, as the goal is to enroll controls so that the control group matches certain characteristics of the case-patient group. With individual matching, case-patients without matched controls are not included in the analysis, potentially reducing the power of the study; frequency matching allows all cases to be included in the analysis. If matching is employed, analyses appropriate to the matched design must be conducted (Kleinbaum et al., 1982; Hennekens et al., 1987; Rothman et al., 2008).
Control misclassification
Case-control studies of sporadic enteric disease frequently include only controls who report no recent diarrheal illness (i.e., well or healthy controls). This practice is primarily motivated by a desire to avoid misclassification. The assumption is that controls reporting a recent diarrheal illness may actually have had mild undiagnosed cases of the illness under study, while controls with no recent history of diarrhea are less likely to have had an undiagnosed case of illness. In practice, however, rates of specific enteric infections are often quite low in a population; unless the infection being studied is hyper-endemic, it is unlikely that a control had diarrhea caused by the infection under study. In this review, 68% of studies that reported control exclusion criteria excluded controls with symptoms of illness.
The selection of controls from persons with another laboratory-confirmed infection can also minimize misclassification bias. Five studies in this review used controls with a laboratory-confirmed infection other than the one under study: studies of Campylobacter (Gillespie et al., 2002 [used C. coli and C. jejuni cases as controls for C. jejuni and C. coli cases, respectively], and Wingstrand et al., 2006 [used non-campylobacteriosis bacterial gastroenteritis patients, mainly Salmonella spp., as controls]), Cryptosporidium (Pintar et al., 2009 [used non-cryptosporidiosis laboratory-confirmed enteric disease cases as controls]), Listeria (Schlech et al., 2005 [used 1 case each of laboratory-confirmed Salmonella and Campylobacter as controls]), and Salmonella (Voetsch et al., 2009 [used other Salmonella serotypes as controls for Salmonella serotype Enteritidis cases]).
Misclassification of controls may also occur if there is protective immunity to the infection. Asymptomatic infections will remain undiagnosed, because medical care is not sought. Asymptomatically infected persons may be included in the control group, which could lead to underestimation of the risk of infection associated with vehicles of exposure. Recent studies in Denmark and the Netherlands on the burden of salmonellosis based on a national sero-survey have shown evidence that previous exposure is widespread (Mangen et al., 2004; Simonsen et al., 2008). Despite this, none of the case-control studies under study incorporated any validation of susceptibility to infection among controls.
Exposure Assessment
Case-control studies rely on a person's recall of a past exposure. Poor recall can result in a biased study with respect to exposure assessment; to minimize the differential effect of this bias, the use of standard questionnaires and trained interviewers can ensure that interviews are conducted as similarly as possible for each case-patient and control (Correa et al., 1994; Rothman et al., 2008). All the studies in this review used a standard questionnaire to assess exposures of case-patients and controls. Half of the studies administered questionnaires over the phone (39 studies, 49%); 14 studies (18%) used postal questionnaires (self-administered by the study participant), and nine studies (10%) conducted face-to-face interviews. Six studies used more than one method.
Because enteric diseases are commonly transmitted through food, most exposures assessed are related to the consumption of particular food items, and, in some instances, where and how that food item was prepared or consumed. The set of possible risk factors, or exposures, included in the questionnaire is determined by hypotheses derived from previous studies of the pathogen and outbreak investigations. The aim of case-control studies of sporadic enteric infection is to evaluate the general risk attributable to specific exposures at the population level, not for an outbreak, so the most meaningful questions may be relatively general (i.e., ”consumption of any chicken,” as opposed to “consumption of Brand X chicken prepared at home”). However, more detailed exposure information can help to inform certain specific intervention efforts and regulatory actions, so investigators must decide the appropriate level of detail in assessing exposures based on the intended use of the results.
The time period about which study participants are asked to remember their exposures is referred to as the exposure window. The end of the exposure window is the point in time before the case-patient or control interview from when the case-patient or control is asked to recall their exposures. For case-patients, the end of the exposure window is usually illness onset, although, especially for infections with long incubation periods, not always; for controls, the end of the exposure window can vary. We define two exposure windows based on different endpoints: (1) the “case-patient onset-based window,” the timing of which is determined by the onset of the case-patient's illness; this can apply to both case-patients and controls, and (2) the “control interview-based window,” which ends at the control interview and is an alternative exposure window for controls. Using the control interview-based window can be especially helpful to reduce recall bias in controls; this approach can be used even if case-patients and controls are matched. The length of the exposure window usually depends on the length and range of the incubation period of the infection being studied; the goal is to capture exposures that occurred just before the incubation period and, therefore, could have been the source of infection. It is important to consider the exposure window in the design phase of a case-control study; identical exposure windows will often, but not always, be used for both case-patients and controls.
In this review, most studies used the case-patient onset-based window (68 studies, 86%) for case-patients. Other points used as the end of the exposure window for case-patients included the case-patient interview (4 studies) and specimen collection date (3 studies), while four studies did not state the end of the exposure window. For controls, just over half of the studies used the control interview-based window (42 studies, 54%), and 27 (39%) used the case-patient onset-based window.
The length of the exposure window for case-patients and controls varied depending on the pathogen being studied; the most common length was 7 days (24 studies, 31%), followed by 5 days (13 studies, 17%). Only five studies (6%) did not report the length of the exposure windows for case-patients and controls. Three studies used multiple exposure windows of different lengths (i.e., 7 days, 3 days, and 1 day), all ending at case-patient illness onset, for assessing exposures to commonly consumed foods (Mølbak et al., 2002; Doorduyn et al., 2005; Marcus et al., 2006). The use of this method was pioneered in a 2002 Danish study of sporadic Salmonella serotype Enteritidis infections, in which the magnitude of association between consuming eggs and infection increased with decreasing exposure windows, 7 days to 3 days to 1 day (Mølbak et al., 2002).
Insights Gained from 20 Years of Investigations of Sporadic Infections
Approaches to the study of sporadic enteric disease have evolved and matured. Before the 1990s, epidemiologic studies of enteric diseases focused largely on outbreak-associated disease. As information needs for policy-making increased, more data about the overall burden of and risk factors for enteric disease was needed. Consequently, more attention has focused on understanding sporadic disease, which comprises a large majority of enteric illnesses. Formal surveillance networks were established with the aim of demonstrating the burden of enteric diseases in the developed world, focusing on sporadic disease (Scallan and Angulo, 2007a, b; Kirk et al., 2008; PHAC, 2008; Majowicz et al., 2010). These surveillance networks facilitated landmark research studies into sporadic enteric disease (Wheeler et al., 1999; Tam et al., 2003, de Wit 2001, Voetsch et al., 2004; Jones et al., 2006a). Many of these surveillance systems have provided population-based platforms for case-control studies.
Specific lessons learned in the past 20 years include the need for careful consideration of the size of the study and the need to pay close attention to the set of exposures being assessed. Case-control studies of enteric infections, particularly those conducted over multiple years, are complex and resource-intensive undertakings, potentially involving multiple surveillance systems, local and regional health authorities, multiple laboratories. These studies need an adequate budget and suitably qualified personnel to coordinate and organize. A study should obviously be large enough to have adequate power to show an effect in the desired analyses. Investigators accustomed to outbreak investigations, which often need only small samples to demonstrate the very strong association that typically exists for the outbreak vehicle, should keep in mind that many of the effects associated with sporadic disease may be weak, even though population attributable fractions may be large, particularly for common exposures. Additionally, if the contaminated sources of sporadic infections are very diverse, and only a small fraction of cases is caused by a certain exposure, there may be insufficient power to show an association, even if the effect is strong. In a recently completed case-control study of Campylobacter infection in England, for example, a sample size of 1,500 cases and 1,500 controls was needed for 80% power to detect a minimum odds ratio of 1.39 at the 0.05 significance level. The sample size was based on chicken consumption as the main exposure of interest and assumed a prevalence of 87% in the control population of eating any chicken in the 10 days before interview (Tam et al., 2009). This example illustrates the general fact that, when exposure frequency in the control population is very high, large studies are needed to demonstrate effects, a situation analogous to that found in many epidemiologic studies of chronic disease.
The selection of exposures about which cases and controls are queried is a key component of the design of these studies, in turn relying on the articulation of clear research questions with plausible hypotheses before the study. A successful case-control study is one that accurately and precisely identifies valid risk factors for infection or disease that can be used to guide practical interventions to prevent illness. Case-control studies of enteric disease are conducted for many reasons, including the following three: (1) as exploratory research into potential risk factors, (2) to confirm existing hypotheses, or (3) to inform policy. Usually, a study will aim to address all three. The plausible hypotheses should take into account country-specific information such as food consumption patterns and food distribution. Case-control studies can identify novel risk factors for enteric disease; follow-up research can confirm, refute, or further explore these exposures, as their association with illness may not be causal. Some recently identified novel risk factors, for some of which further research has been conducted, include contact with sandboxes, associated with Salmonella serotype Typhimurium infections in the Netherlands (Doorduyn et al., 2005), consuming hummus or melons prepared in commercial establishments, associated with Listeria infections in the United States (Varma et al., 2006), and, for infants, riding in shopping carts next to meat or poultry, associated with Salmonella and Campylobacter infections in the United States (Jones et al., 2006b; Fullerton et al., 2007).
Many areas for further research exist to improve the validity and usefulness of case-control studies of enteric disease. Some prominent examples include the interpretation of “protective factors” and the role of immunity. One consistent finding across many case-control studies of enteric infections, regardless of pathogen, is the identification of factors negatively associated with infection, or so-called “protective factors.” While some exposures are expected to be protective against enteric infections (e.g., breast feeding in infants, drinking filtered water), the interpretation of findings that suggest that the consumption of certain foods is associated with decreased risk is not straightforward. Several explanations in addition to causal effect (i.e., that the identified factor does indeed confer protection from infection when consumed) have been offered, including bias due to differential recall of exposure between case-patients and controls or due to confounding. Confounding could be at play if protective factors are associated with other unmeasured factors that affect risk, such as lifestyle factors or socioeconomic factors. As further discussed below, it is also possible for “protective” associations to be observed with exposures that are actually risky but that occur frequently and lead to protective immunity (Kapperud et al., 1998, 2003; Swift and Hunter, 2004; Stafford et al., 2006; Voetsch et al., 2007).
The impact of individual immunity on the comparison of case-patients and controls, particularly for Campylobacter infections, is intriguing and warrants further exploration (Adak et al., 1995; Friedman et al., 2004; Havelaar et al., 2009). While the impact of the immune status of controls on the results of case-control studies is unknown, and to the extent that exposure to common sources of infection may be associated with protective immunity, it can be presumed that if controls are immune to the particular infection under study then the measures of association between risk factors and infections may be decreased; true risk factors may appear to be less strongly associated with illness or may even appear to be protective factors. It has been suggested that protective factors may be found where there is longstanding or lifelong protective immunity owing to exposure to the pathogen over many years; however, this may not be the case for some enteric infections (Swift and Hunter, 2004; Havelaar et al., 2009). A history of previous exposure to the pathogen in an individual (leading to individual immunity) could be a confounder of the association of current exposure and infection and could be treated as such through the study design and analysis (Rothman and Mahon, 2004). Consequently, case-control studies of sporadic infections that are unable to include information on the immune status of participants may be better able to identify risk factors where exposure is only occasional, where the pathogen is uncommon, where protective immunity is not long-lasting. Alternatively, collecting information about chronic as well acute exposures could allow for control for confounding by previous immunity in analysis. An important advance in methodology for case-control studies would be the ability to use rapid antibody tests to determine the immune status of controls, allowing inclusion of only non-immune controls.
Attribution of foodborne illness to specific food commodities (Adak et al., 2005; Painter et al., 2009; Pires et al., 2009) has become a high priority for regulatory authorities in many countries. Thus, using consistent methods to define foods and food commodities across countries is becoming increasingly valuable. Additionally, a potential next step in the evolution of the analysis of case-control studies of sporadic enteric disease is to estimate the total number of illnesses caused by a specific exposure. One approach is to combine population attributable fraction proportions with surveillance data and reporting multipliers; in Australia, this type of analysis estimated that 50,500 Campylobacter infections annually occurred because of consumption of contaminated chicken (Stafford et al., 2008).
Conclusion
Previous reviews of case-control studies have considered methods and included studies from a broad range of disease areas (Wingo et al., 1998; Pocock et al., 2004; Knol et al., 2008). We review methods used in case-control studies of sporadic enteric infections.
The case-control design is useful for describing the relative importance of a range of risk factors for sporadic enteric infections, and can identify possible risk factors. As our understanding of sporadic enteric infections grows, methods, topics, and uses for case-control studies are expected to continue to evolve; for example, advances in understanding of the role of immunity can be used to improve control selection, the apparent protective effects of certain foods can be further explored, and the studies can provide population-based measures of the burden of disease.
Footnotes
Disclosure Statement
No competing financial interests exist.
*
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.