
Abstract
We describe prevalence and antimicrobial susceptibility results for thermophilic Campylobacter isolates collected from humans, food, and food-animals in an integrated food chain surveillance network in Mexico. From 2003 to 2006, stool samples were collected from children with diarrhea at state sentinel hospitals. Concurrently, fecal samples from asymptomatic children in kindergartens, as well as raw chicken, pork and beef from retail outlets, and food-animal intestines from slaughterhouses were all collected in 65 cities from four different states. C. jejuni was identified with a standardized hippurate test. Hippurate negative, indoxyl acetate positive isolates were classified as Campylobacter spp. Susceptibility testing was performed by agar dilution according to Clinical and Laboratory Standards Institute guidelines. A total of 1,259 C. jejuni and 1,797 Campylobacter spp. isolates were recovered from 11,811 samples. Chicken was significantly more contaminated for both intestinal samples (93.6%) and meat products (58.3%), compared with swine (71.4%)/pork (14.6%) samples, and cattle (25.1%)/beef (5.3%) samples (p<0.001). Campylobacter was recovered from 5.1% of children with diarrhea and from 3.2% of asymptomatic children. Chicken was significantly more likely to harbor ciprofloxacin-resistant C. jejuni (85.8%) than swine (62.5%, OR=3.6), cattle (39.8%, OR=9.3), or humans (58.2%, OR=4.4). No significant differences were found for ciprofloxacin-resistant Campylobacter spp. among food-animals, but the rate in food-animals was significantly higher than in humans (84% vs. 56.7%, OR=4.0). Swine was significantly more likely to harbor erythromycin-resistant C. jejuni (14.8%) than chicken (3.5%, OR=4.9), cattle (1.8%, OR=9.3), or humans (3.0%, OR=5.7), and was associated with higher rates of erythromycin-resistant Campylobacter spp. (41.9%) than chicken (10.5%, OR=6.1) and humans (11.9%, OR=5.3). The high resistance rates to ciprofloxacin preclude the use of fluoroquinolones for treatment of campylobacteriosis in Mexico. Our results emphasize the need for ongoing and integrated surveillance of antimicrobial usage and antimicrobial susceptibility in humans and animals.
Introduction
C
During the last two decades, Campylobacter isolates have become increasingly resistant to antimicrobial agents. The public health community has voiced concern about the increasing resistance to fluoroquinolone and macrolide antibiotics, as these are the drugs of choice for severe infections caused by this pathogen (Luangtongkum et al., 2009). Due to the growing globalization of food trade and travel, international organizations have recommended that surveillance for isolation and antimicrobial resistance of foodborne pathogens should be conducted along the entire food chain (WHO, 1997, 2002; FAO, 2003).
Comprehensive surveillance studies on the prevalence and antimicrobial resistance of Campylobacter are rare in low and middle income countries due to the cost of the selective media, the microaerophilic atmosphere, and the technical skills required. In 2002, we established an active and integrated food chain surveillance system for Salmonella, Campylobacter, and Escherichia coli in four states in Mexico. The study methodology was designed to create a sustainable surveillance program in a developing country such as Mexico. We have previously reported the surveillance results for Salmonella, in which we observed high frequencies of antimicrobial resistance in humans, food, and animals. High resistance rates to extended-spectrum cephalosporins were identified as a major public health risk (Zaidi et al., 2008).
In this report, we describe prevalence and antimicrobial susceptibility results obtained by the network for Campylobacter isolates collected from 65 different cities during 2003–2006.
Methods
Sample collection
The network included states from four different geographical regions of Mexico: Sonora in the northwest, San Luis Potosi in the center, Michoacan in the southwest, and Yucatan in the southeast. Food-animal production is a major economic activity in these states; most of the retail meat is locally produced. The sampling methods and design were fully described in a previous publication (Zaidi et al., 2008). Briefly, active surveillance was conducted in one city per month. In each city, at least 40 fecal samples from kindergarten children; 10 each of retail chicken, pork, and beef from municipal markets and butcheries; and 10 each of chicken, swine, and cattle intestines (cecum) from municipal slaughterhouses were collected. Large cities were sampled more than once at different retail outlets and kindergartens. Active surveillance was also conducted on ill children admitted to state public hospitals. Stool samples collected from ill children with diarrhea and asymptomatic children from kindergartens were transported in Cary-Blair medium. Raw retail meat and food-animal intestines were transported in sterile plastic bags, placed in chilled ice boxes, and processed within 24 h.
Isolation, identification, and antimicrobial susceptibility testing
All participating laboratories used the same standardized methods for isolation of Campylobacter. Stool samples and animal intestines were placed in buffered peptone water for 30 min and plated on Cefex agar (Brucella agar with 5% lysed horse blood, 10 μg/mL rifampin, 50 μg/mL nystatin, and 33 μg/mL cefoperazone). Raw retail meat was incubated in Bolton broth with Bolton Broth Selective Supplement (Oxoid, Cambridge, UK) for 24 h at 37°C and subcultured on Cefex agar. Cefex plates were incubated for 48 h at 42°C in microaerophilic atmosphere (85% N2, 10% CO2, 5% O2). Campylobacter isolates were sent to the coordinating center in Yucatan, where they were verified by phase-contrast microscopy and positive oxidase and catalase tests. Isolates were speciated by a single, experienced microbiologist using hippurate and indoxyl acetate tests. For the hippurate test, a dense suspension (McFarland ∼5) was incubated in a 37°C water bath for 2 h after which ninhydrin solution was added to the tube. Only a dark purple color was considered a positive result (Nachamkin, 2003). A positive control was run with every test batch. Hippurate-negative, indoxyl acetate–positive isolates were classified as Campylobacter spp. Susceptibility testing to erythromycin, ciprofloxacin, gentamicin, and tetracycline by agar dilution on Mueller-Hinton agar with 5% sheep blood was performed according to Clinical and Laboratory Standard Institute recommendations (CLSI, 2009). C. jejuni ATCC 33560 was used as a control strain. Susceptibility results were analyzed using WHONET software version 5.6.
Ethical considerations
The protocol was reviewed and approved by the Ethics Committee at each participating institution. Informed consent for processing the children's stool samples and using the data for research purposes was obtained from all legal guardians.
Statistical analysis
Statistical analysis was performed with the chi-square test with Yates' correction and the estimation of the odds ratio with 95% confidence intervals for comparing isolation and resistance rates among sources.
Results
Recovery from human, retail meat, and animal samples
A total of 3118 Campylobacter isolates were recovered from 11,811 samples, of which 1,259 were classified as C. jejuni and 1,797 as Campylobacter spp. Sixty-two isolates that were both hippurate-negative and indoxyl acetate–negative were excluded from analysis. In comparing intestinal samples from animals, chicken intestine was significantly more contaminated with Campylobacter (93.6%) than swine (71.4%; p<0.001, OR=3.7, 95% CI 2.8–5.0) or cattle (25.1%; p<0.001, OR=43.3, 95% CI 31.8–59.2). Likewise, chicken meat was significantly more contaminated (58.3%) when compared to pork (14.6%; p<0.001, OR=9.5, 95% CI 7.8–11.6) and beef (5.3%; p<0.001, OR=28.8, 95% CI 21.2–39.4) (Fig. 1). Campylobacter was isolated from 5.1% of children with diarrhea and 3.2% of asymptomatic children.
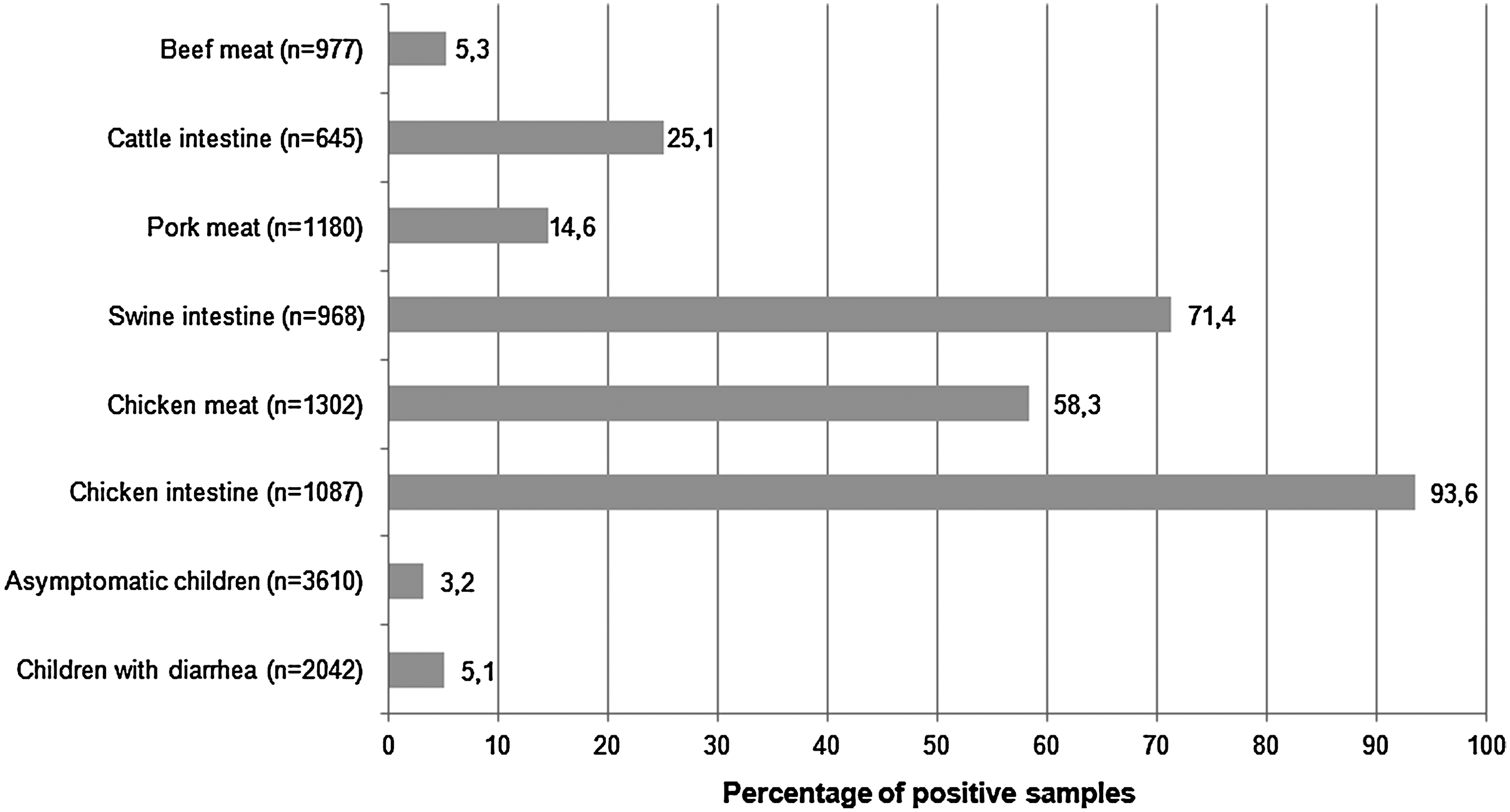
Prevalence of Campylobacter in human, retail meat, and food-animal samples in Mexico, 2003–2006.
Antimicrobial susceptibility patterns
The proportions of resistant Campylobacter isolates and the minimum inhibitory concentration (MIC) distributions for all sources are shown in Table 1. Tables 2 and 3, respectively, show the MIC distributions for C. jejuni and Campylobacter spp. by animal source. Comparison of the resistance rates among sources, including the odds ratio, is shown in Table 4.
Includes resistant and intermediate.
Vertical lines indicate breakpoints for susceptibility; MIC values may not add up exactly to 100% due to rounding off.
Includes resistant and intermediate.
Chicken, swine, and cattle isolates collected from food-animal intestines at slaughter and their corresponding raw retail meat have been combined because resistance patterns were very similar.
Vertical lines indicate breakpoints for susceptibility; MIC values may not add up exactly to 100% due to rounding off.
Refers to thermophilic hippurate-negative, indoxyl-positive Campylobacter.
Includes resistant and intermediate.
Chicken, swine, and cattle isolates collected from food-animal intestines at slaughter and their corresponding raw retail meat have been combined because resistance patterns were very similar.
Vertical lines indicate breakpoints for susceptibility; MIC values may not add up exactly to 100% due to rounding off.
Refers to thermophilic hippurate-negative, indoxyl-positive Campylobacter.
NS, not statistically significant.
Chicken was significantly more likely to harbor ciprofloxacin-resistant C. jejuni (85.8%) compared to swine (62.5%, OR=3.6), cattle (39.8%, OR=9.3), or humans (58.2%, OR=4.4). There were no differences in ciprofloxacin resistance among Campylobacter spp. isolates in the different food-animals; however, the resistance rates in food-animals were significantly higher than in humans (84% vs. 56.7%, p<0.001, OR=4.0; Tables 3 and 4). Erythromycin-resistant C. jejuni was significantly higher in swine (14.8%) than in chicken (3.5%, OR=4.9), cattle (1.8%, OR=9.3), or humans (3.0%, OR=5.7); swine also more frequently harbored erythromycin-resistant Campylobacter spp. (41.9%) than chicken (10.5%, OR=6.1) and humans (11.9%, OR=5.3). Resistance rates for tetracycline were significantly higher in C. jejuni from cattle (81.6%) and Campylobacter spp. (84.8%) from swine. No differences were observed for gentamicin-resistant C. jejuni among the different sources; gentamicin-resistant Campylobacter spp. (15.4%) was significantly higher in cattle when compared to chicken and humans (Tables 2 –4).
Discussion
This study comprehensively examines Campylobacter isolates throughout the food chain in Mexico. The prevalence data paralleled proportions reported for other national and regional surveys where chicken (carrying mainly C. jejuni) and swine (mainly C. coli) commonly harbor Campylobacter, with chicken meat showing more frequent contamination than pork or beef products (FDA, 2011; Gupta et al., 2004).
Our results showed that there was a high frequency of resistance to ciprofloxacin and tetracycline; lower rates were seen for erythromycin and gentamicin. Resistance rates in humans were very similar to those reported for Argentina during a similar time period (62% resistance to ciprofloxacin and 3% to erythromycin) (PAHO, 2005). High frequencies of ciprofloxacin resistance in human isolates have also been reported in France (25% to 42%) (Gallay et al., 2007) and Germany (46%) (Luber et al., 2003). Ciprofloxacin resistance has reached very high frequencies in Thailand and Taiwan (75% to 92%), where Campylobacter is a major cause of dysentery in children and travelers (Bodhidatta et al., 2002; Isenbarger et al., 2002; Yang et al., 2008). Lower rates have been reported for C. jejuni in the United States with a 17.2% resistance to ciprofloxacin and 0.3% resistance to erythromycin (PAHO, 2005).
Although the antimicrobial resistance rates in this study varied by food-animal and compound, they were significantly higher than in humans for all antimicrobials tested. Our resistance patterns in food-animals are comparable to those in certain regions of Asia where resistance rates in food-animals are high, usually above 55% (Cokal et al., 2009; Padungtod et al., 2006). In China, the problem is particularly acute, as ciprofloxacin resistance has reached almost 100% in broilers (Chen et al., 2010). A large surveillance study conducted in the European Union (EFSA, 2010) reported a trend toward increasing resistance in both C. jejuni and C. coli from 2005 to 2007. Among C. jejuni from live poultry, ciprofloxacin and erythromycin resistance rose from 33% and 1%, respectively, in 2005, to 43% and 4%, respectively, in 2007. Similar trends were observed in C. coli from swine. During this period, ciprofloxacin resistance rose from 35% in 2005 to 46% in 2007, while erythromycin resistance rose from 25% to 39%. Far lower resistance rates have been reported in C. jejuni isolates from chicken meat in Canada (2.1% to 2.5% resistance to ciprofloxacin, and 7.1% to 15.8% resistance to erythromycin) (CIPARS, 2004). In the United States, macrolide resistance in C. jejuni among isolates from retail meats has basically remained below 3%, while C. coli resistance has been consistently higher, ranging over 12%, but with no significant temporal trend in either species. Ciprofloxacin resistance, while also higher in C. coli, has remained largely unchanged over the past 7 years ranging from 20% to 30% (FDA, 2011).
We found that 3% of healthy asymptomatic kindergarten children in Mexico (3–7 years of age) were shedding Campylobacter in their feces. Our findings are consistent with cohort studies conducted in Peru and Mexico where Campylobacter isolation rates decline with age (Calva et al., 1988, Oberhelman et al., 2003). Children younger than 1 year of age have the highest rates of Campylobacter diarrhea; almost no episodes occur in those over 5 years old. These and other recent studies suggest that age-acquired immunity may modify the burden of antimicrobial-resistant Campylobacter in Mexico. Surveillance data collected by our network showed that Campylobacter was less frequently isolated from children with diarrhea (5.1%) than was Salmonella (12.3 %) or Shigella (7.9%) (Zaidi et al., 2008). A recent cohort study in Yucatan also showed that Campylobacter gastroenteritis carried a lower burden of disease compared to Salmonella, Shigella, and diarrheagenic E. coli (Zaidi et al., 2012). In contrast, a recent report from Western Mexico (Larrosa-Haro et al., 2010) found that Campylobacter was the most commonly isolated bacterial pathogen (15.7%) in young children with diarrhea, indicating that there may be significant regional differences within the country.
There were several limitations to our study. The lack of accurate data on the quantity and type of antimicrobials used in food animal production and clinical medicine limits our ability to assess the risks associated with increased resistance in foodborne pathogens. Data on disease severity and treatment in humans was not systematically collected; we were thus unable to establish the relationships between antimicrobial-resistant Campylobacter and negative human health impacts. In Mexico, fluoroquinolones are not licensed for the pediatric population and tetracyclines are prohibited for children under the age of eight; however, both these antibiotics are used in food-animal production, as are macrolides and aminoglycosides (Anonymous, 2004). It is thus reasonable to assume that many of the fluoroquinolone and tetracycline-resistant Campylobacter strains isolated from the children in our study were transmitted through contaminated food or direct contact with animals. The method we used for species differentiation is yet another shortcoming. Polymerase chain reaction is currently the gold standard for distinguishing among different Campylobacter species. In this study, a single, experienced microbiologist used standardized inoculums, and classified isolates as C. jejuni only for unambiguous positive tests. Although standard references continue to recommend the use of hippurate and indoxyl acetate tests for differentiating thermophilic Campylobacter for routine surveillance and processing of clinical specimens (Fitzgerald et al., 2011; OIE, 2011), and the use of a standardized method by skilled personnel reduces the risk of misclassification (Nakari et al., 2008), we chose to classify our hippurate-negative isolates as Campylobacter spp. instead of C. coli to avoid uncertainty. Our Campylobacter spp. isolates share many of the features reported for C. coli in the scientific literature, such as a higher prevalence in swine and cattle, and higher frequencies of resistance to erythromycin and gentamicin (Zhao et al., 2010). While the use of molecular methods would yield greater accuracy, the cost and technical skill needed for identifying large numbers of isolates makes this unfeasible for Mexico and most low to middle income countries. Furthermore, the overall burden of Campylobacter infections in Mexico is lower than other pathogens such as Salmonella and Shigella, and therefore, does not justify the cost involved (Zaidi et al., 2012).
Conclusion
This is the first extensive study of Campylobacter along the food chain in Mexico. The high resistance rates to ciprofloxacin among human isolates preclude the use of this antibiotic class for treatment of campylobacteriosis. More broadly, our antimicrobial susceptibility results point to the need for ongoing periodic surveillance for resistance trends in foodborne pathogens in both the veterinary and medical sectors. Well-designed studies on the human health impact of antimicrobial usage in food-animals as well as consequent risk-based regulations on the use of antimicrobials in food production are warranted.
Footnotes
Acknowledgments
This study was financed by the U.S. Food and Drug Administration (grant FD-U-001934-03-2) and the Fundacion Mexicana para la Salud, Capitulo Peninsular.
Disclosure Statement
No competing financial interests exist.