
Abstract
Over 1,100 foodborne disease outbreaks cause over 23,000 illnesses in the United States annually, but the rates of outbreaks reported and successful investigation vary dramatically among states. We used data from the Centers for Disease Control and Prevention's outbreak reporting database, Association of Public Health Laboratories' PulseNet laboratory subtyping network survey and Salmonella laboratory survey, national public health surveillance data, and national surveys to examine potential causes of this variability. The mean rate of reporting of Salmonella outbreaks was higher in states requiring submission of all isolates to the state public health laboratory, compared to those that do not (5.9 vs. 4.1 per 10 million population, p=0.0062). Rates of overall outbreak reporting or successful identification of an etiology or food vehicle did not correlate at the state level with population, rates of sporadic disease reporting, health department organizational structure, or self-reported laboratory or epidemiologic capacity. Foodborne disease outbreak surveillance systems are complex, and improving them will require a multi-faceted approach to identifying and overcoming barriers.
Introduction
While multistate outbreaks tend to be large and diffuse, and garner a disproportionate amount of attention, the huge majority of reported FBDOs occur in small, well-defined populations (such as patrons of a restaurant or within a single county). Most outbreak investigations are completed at the local level and do not involve federal agencies (Murphree et al., 2012). The detection of these events and the intensity with which they are investigated depend substantially on local and state resources, staff expertise, and interest. While the popular media and various reports have drawn attention to dramatic differences among states in outbreak reporting (Harris, 2009; Hargrove, 2006; CSPI, 2010), few data are available regarding reasons for that variability. A greater than 20-fold difference in rates of reported outbreaks among states, for example (CSPI, 2010), indicates that there is substantial opportunity to improve outbreak response and, as a consequence, improve our ability to understand and ultimately prevent unnecessary disease burden nationally.
In order to identify ways to improve FBDO investigations, it is important to understand barriers to their success. We examined national data on outbreak reporting rates, investigation outcomes, and laboratory and epidemiologic capacity in states to determine reasons for variability in success rates and identify specific areas to which improvement efforts may be targeted.
Materials and Methods
Data on foodborne disease outbreaks reported to the CDC are collected from all U.S. states through the Electronic Foodborne Disease Outbreak Reporting System (eFORS; recently renamed the National Outbreak Reporting System) (CDC, 2010a). We analyzed national data from eFORS during 2000–2009. CDC criteria were used to define a FBDO as the occurrence of ≥2 cases of a similar illness resulting from the ingestion of a common food (CDC, 2009). An outbreak was classified as having an implicated food vehicle if one was identified in the eFORS report. CDC criteria were used to define a confirmed etiology, which in most cases requires the pathogen or toxin to be identified in clinical specimens from two or more outbreak-related patients, or the implicated food vehicle (CDC, 2010b). For comparisons among states, FBDOs classified as “multistate” (due to food exposures in more than one state) were excluded from the analysis, because the roles of particular agencies cannot be determined from data available in those cases.
We compared rates of sporadic cases and outbreaks due to Salmonella, as it is the most common bacterial pathogen associated with both. Salmonella isolates are routinely submitted to PulseNet, the national molecular subtyping network for foodborne disease pathogens, for molecular subtyping. Data on incidence of individual Salmonella infections were obtained from CDC surveillance reports (CDC, 2012c). We compared ratios of rates of individual cases and outbreaks during 2000–2009, to assess whether underlying disease rates could explain state-to-state variability in outbreak rates.
Data on state-specific epidemiologic capacity for foodborne disease control were collected through a Council of State and Territorial Epidemiologists (CSTE) survey of state foodborne disease epidemiologists in 2010. A variety of questions regarding self-assessment of their state's capacity to respond to FBDOs were asked (e.g., ability to pay overtime, laboratory capacity, statistical support, competing priorities, difficulties working with other state or federal agencies, travel restrictions, delays in notification of reportable diseases), with categorical classification of results (CSTE, 2011). State-specific data regarding rates of collection, serotyping, and molecular subtyping of Salmonella isolates were collected through a national PulseNet survey by the Association of Public Health Laboratories (APHL) in 2008 and a Salmonella laboratory capacity and capabilities survey in 2010. Responses were compared to rates of outbreaks reported, and proportions of outbreaks in which the etiology, food vehicle, either, or both were identified. The proportions of outbreaks in which the etiology, a food vehicle, or both were identified were among measures used to assess successful outcomes of investigations. The CSTE and APHL surveys were performed with a guarantee of anonymity to respondents, and data were required to be de-identified after linking.
Statistical analysis
Data were analyzed using SAS 9.2 (SAS Institute, Inc., Cary, NC). Univariate linear regression was performed for most analyses, using coefficient of determination R 2. Poisson regression with Wald 95% confidence limits was used for comparison of means.
Results
During 2000–2009, 11,256 FBDOs involving 236,042 ill persons were reported to CDC. Of these, 124 (1.1%) were categorized as “multistate” outbreaks and were excluded from further analyses. The number of outbreaks reported by individual states over the 10-year period ranged from nine to 1,581. The mean annual rate of reported outbreaks was 38 per 10 million population (among states, range of 2.6–209 per 10 million). Overall, 4,628 (41%) FBDOs had a confirmed etiology. The proportion of outbreaks with a confirmed etiology varied by state from 10% to 90% (Fig. 1). Rates of outbreak reporting did not correlate with state population (Fig. 2a).
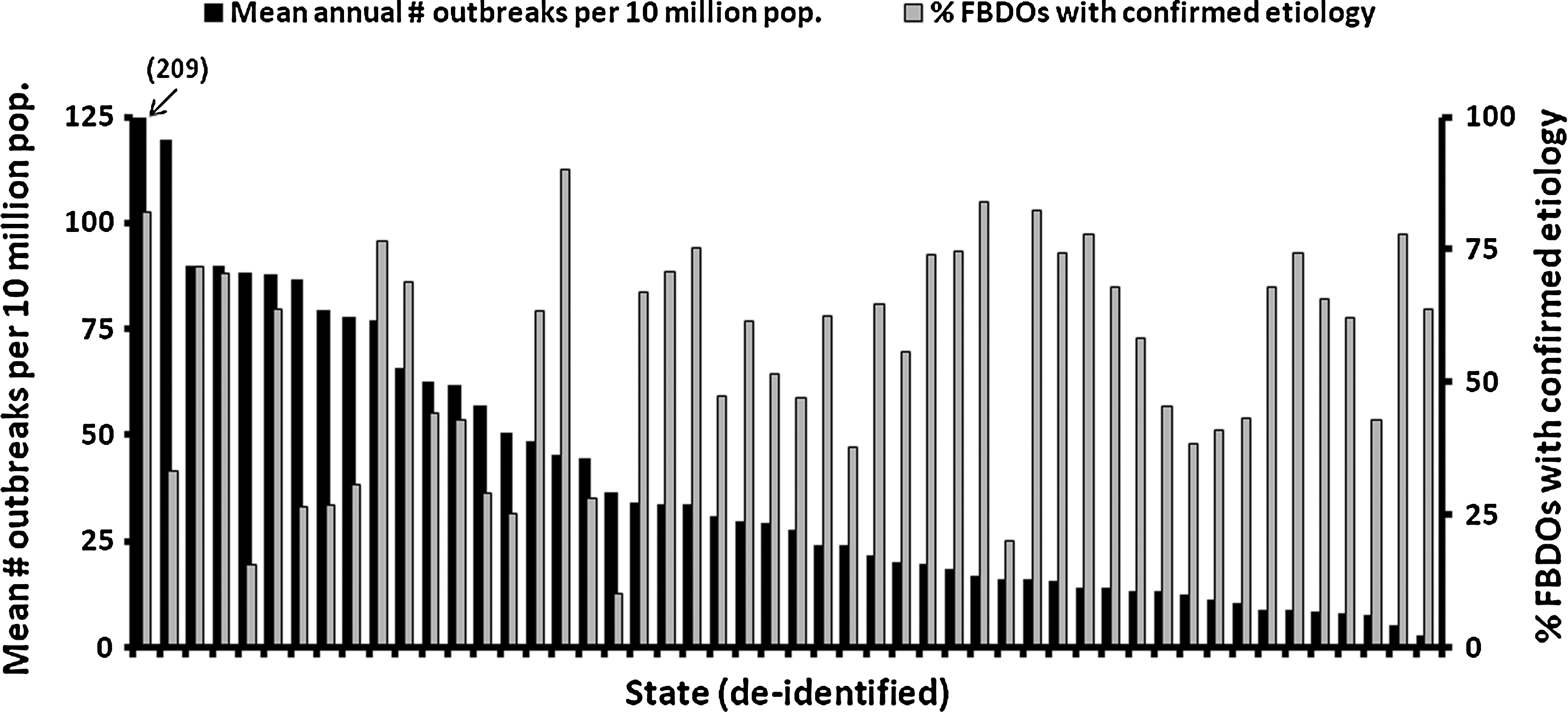
Annual rates of foodborne disease outbreaks reported to the Centers for Disease Control and Prevention per 10 million population, and proportion of reported foodborne disease outbreaks (FBDOs) with a laboratory-confirmed etiology, by state (de-identified), 2000–2009.
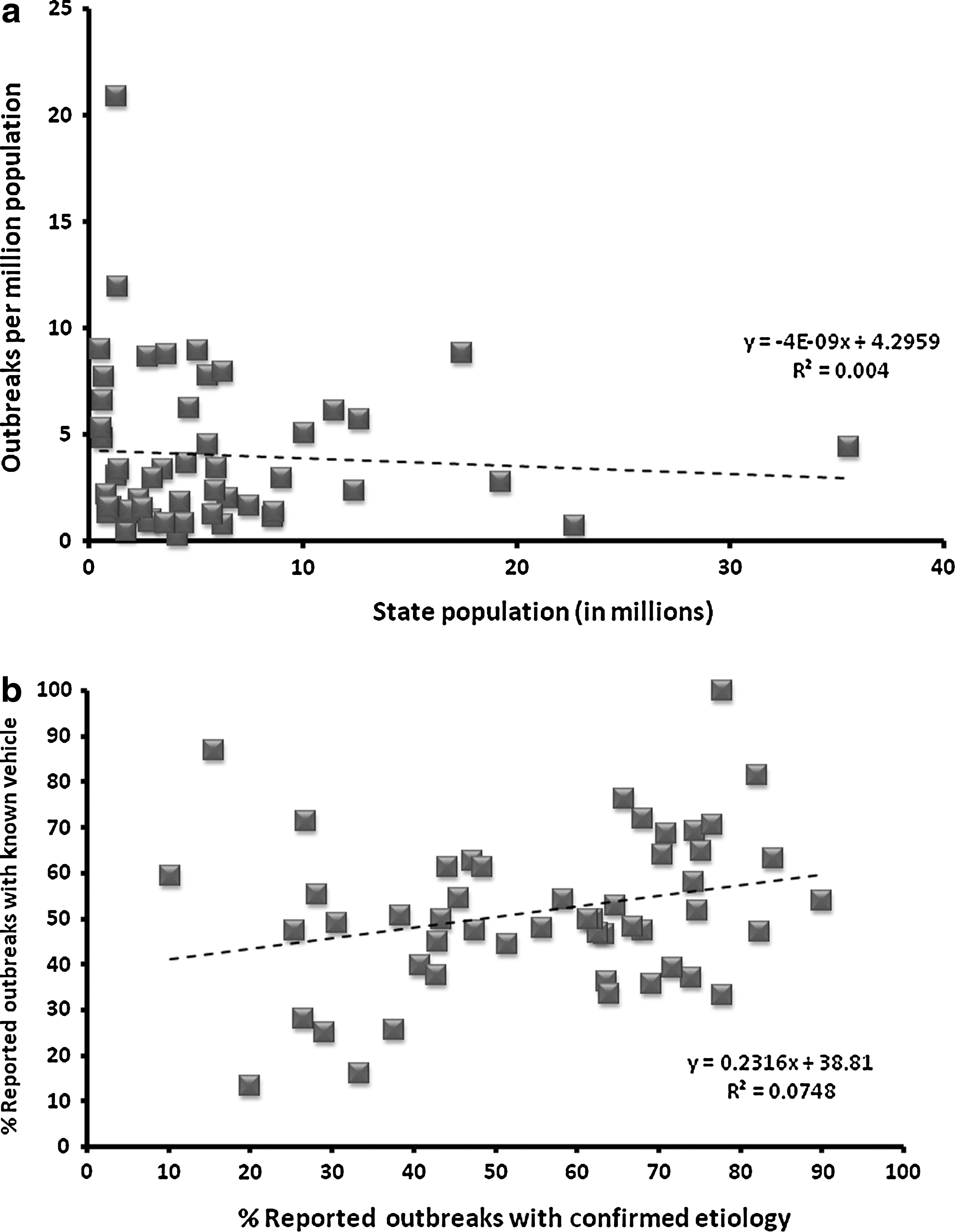
Examples of scatter plots showing (a) lack of correlation between a state's population and its rate of reported foodborne outbreaks and (b) correlation between a state's success in identifying an etiologic agent and identifying a food vehicle, during a foodborne disease outbreak investigation.
A food vehicle was identified in 6,228 (55%) outbreaks (among states, range of 13–100%), and both the etiology and food vehicle were identified in 2,731 (24%, range of 0–78%). There was no correlation between rates of identification of the food vehicle, etiology, or both, and a state's overall rate of reported outbreaks or state population. Success in identifying an etiologic agent did correlate with success in identifying a food vehicle (Fig. 2b).
During the study period, 1,256 Salmonella outbreaks were reported (overall U.S. rate of 4.3 outbreaks per 10 million population, range among states of 0.2–66). Of 442,497 individual cases of Salmonella reported during this period, 3,029 (6.8%) were associated with recognized FBDOs. The ratio of overall rates of Salmonella infections (per 100,000 population) to rates of Salmonella outbreaks (per 10 million population) to reported by states varied dramatically (overall U.S. ratio of 35.2, range among states of 1.27–1202.8).
All states require reporting of Salmonella cases to the health department. In 2010, 30 (60%) states required submission of isolates to their state laboratories. Forty-nine state laboratories reported performing Salmonella serotyping; 48 serotype all isolates received, and one does so selectively. All 50 states perform pulsed-field gel electrophoresis (PFGE) molecular subtyping of Salmonella isolates. Overall, approximately 94% of isolates received are subtyped; 43 states routinely subtype all isolates received (including 11 which do not require submission). The mean rate of reporting Salmonella outbreaks was higher in states requiring submission of all isolates to the state public health laboratory, compared to those that do not (5.9 vs. 4.1 per 10 million population, p=0.0062), but not in states that routinely subtype all isolates received versus those who did not (5.4 vs. 4.7 per 10 million population, p=0.7770). Isolate submission requirement and routine PFGE policies did not correlate with improved rates of identifying a food vehicle in Salmonella outbreaks, or the proportion of all FBDOs with an identified etiology or food vehicle.
Univariate regression analyses were performed to identify correlations between subjective evaluations of epidemiological limitations within state health departments (from the CSTE survey) and objective investigation outcomes (rates of outbreak reporting, and identification of an etiology and/or food vehicle). The only positive correlation was an association between reported increased difficulty working with other state and federal agencies and lower overall statewide rates of outbreak reporting (correlation coefficient=2.8; p=0.002).
Discussion
There are dramatic differences across the United States in capacities to report and investigate foodborne disease outbreaks, with rates of reported Salmonella outbreaks varying 30-fold among states (CSTE, 2011). We found that the mean rate of reporting such outbreaks was higher in states that require submission of all Salmonella isolates to their state laboratories, and in states that routinely perform molecular subtyping of all isolates, compared to those that do not. States that more frequently identified an etiologic agent also tended to have more success identifying a food vehicle during outbreak investigations. States with higher overall rates of outbreak reporting noted less difficulty working with other state and federal partners compared with those with lower rates. The latter may reflect increased comfort with interagency communication as experience with outbreak investigations grows and such interactions become more routine. The numerous steps required in outbreak investigations depend on coordination of a variety of agencies and activities, and no single intervention will resolve all problems with the system. Overcoming barriers to successful investigations will require solutions that are tailored to individual states and counties.
Data specifically regarding funding of foodborne disease programs in states are not readily available. Because two of the significant factors associated with successful investigations were associated with the laboratory, attention should be given to ensuring that states have resources to support submission and routine subtyping of all Salmonella isolates. While increased resources may be necessary to improve states' capacities to respond to foodborne outbreaks, increased funding alone is unlikely to solve all barriers to successful investigations. Data-driven targeting of available resources is important. Substantial flexibility is necessary for individual state or local jurisdictions to focus on different steps in the investigation process depending on evaluation of an individual program's needs. Currently, there are few data to compare performance of state programs at specific steps in the process of foodborne disease response (such as time from disease onset to reporting to the health department, time from culture to serotyping or PFGE, proportion of case interviews completed) (Hedberg et al., 2008). Suggested performance metrics for laboratories, epidemiology, and environmental health programs have recently been published by the Council to Improve Foodborne Outbreak Response (CIFOR, 2010), and others are under development by the CDC (CDC, 2012a). In addition, capacity to respond to foodborne disease outbreaks is being incorporated into assessments of states' public health emergency preparedness programs (Potter et al., 2007). As data are collected and available for comparison among states, individual programs will increasingly be able to identify specific areas in need of improvement and assess changes over time.
This study evaluated variability in performance at the state level. With over 3000 county health departments in the United States, it is likely that similar dramatic differences exist at local levels, which may in part explain our inability to identify more factors that consistently correlated with success among states. The distribution of responsibilities for public health functions varies widely. In some states, most reports of foodborne disease are collected and investigated by a single centralized state agency, while in others individual counties or cities are very independent and rely minimally on state programs for support. Performance indicators have been developed for local and county food safety programs (CIFOR, 2010), and it is important that individual states evaluate these data as they determine how to focus efforts at improvement.
This study had a number of limitations. Reporting of foodborne disease outbreaks to the CDC is passive and voluntary, and there are no data available to assess the completeness or consistency of reporting across states. It is also possible that there are biases toward reporting outbreaks in which an etiology or food vehicle is successfully identified. Many of the results of the national survey of foodborne disease epidemiologists involved subjective assessments of programmatic barriers, which are likely highly interdependent and potentially confounding. The timeframes of the programmatic surveys and available surveillance data did not correlate exactly, and it is possible that changes over time in staffing and laboratory practices could affect our results. Because there is no standard, quantifiable measure of the “success” of outbreak investigations, we used the best surrogates available from existing data. It would be useful to examine the effect of public health funding, laws, regulations and policies on the performance of food safety programs. We found that the wide variability in reported rates of Salmonella outbreaks among states is not due solely to underlying differences in disease rates. It is important, therefore, that assessments of outbreak investigations be used as only one of a variety of indicators of a state's public health capacity.
A variety of programs are being developed to help improve the level of FBDO response in the United States. Current efforts include standardization of foodborne disease questionnaires among states, increased participation in PulseNet, FoodNet, Rapid Response Teams, FoodCore, the Environmental Health Specialist Network, the multi-agency CIFOR, implementation of the Food Safety Modernization Act, and a host of training projects (CDC, 2012b). The impact of uniform national training to improve the competence and consistency of the public health workforce should also be explored. These programs all have different focuses, and as successes are identified they should be widely shared and applied. As specific barriers can be targeted for improvement, eliminating performance disparities among states will lead to improved food safety for the entire country.
Footnotes
Acknowledgments
This publication was supported in part by Cooperative Agreement U60HM000803 from the Centers for Disease Control and Prevention (CDC) to the Association of Public Health Laboratories. Its contents are solely the responsibility of the authors and do not necessarily represent the official views of CDC.
Disclosure Statement
No competing financial interests exist.