
Abstract
We carried out a cross-sectional study to determine the level of knowledge and awareness regarding children's food safety issues among the school-based street food vendors in Dhaka city. A total of 250 school-based street food vendors were interviewed employing a pre-tested structured questionnaire comprising foodborne illness and food hygiene–related questions. We used a scoring system based on the responses obtained from them, and categorized the overall level of knowledge and awareness into “adequate” and “inadequate.” Multivariable logistic regression was used to explore the association between selected sociodemographic characteristics and the level of knowledge and awareness. The most common food item vended by school-based street food vendors was chotpoti/fuchka (37.2%). The median number of schoolchildren customers was 120 per vendor per day. All (100%) vendors were male with a mean age of 30.95±8.8 years, and their mean daily income was 131.16±62.54 Bangladeshi Taka (1.97±0.94 USD). Most (40.1%) of the respondents belonged to the age group 25–34 years, and the majority (43.6%) did not have any formal education. More than two-thirds (68%) vendors could not show adequate level of knowledge and awareness of children's food safety issues. The most common source of obtaining food safety information by vendors was electronic media (91.8%). Elderly (≥45 years) vendors were 17.73 times more likely to have adequate level of knowledge and awareness than the vendors belonging to age group 15–24 years (p<0.001; adjusted OR=17.73; 95% CI=4.38–71.73). Individuals who had an education of higher than primary level were 9.87 times more likely to possess adequate level of knowledge and awareness than those who did not have any formal education (p<0.01; adjusted OR=9.87; 95% CI=2.07–46.93). The majority of school-based street food vendors showed an inadequate level of knowledge and awareness of children's food safety issues.
Introduction
M
Consumption of street-vended foods and beverages is a frequent event in metropolitan cities of the developing world (Mensah et al., 2002). The World Health Organization (WHO) has defined “street-vended foods” or its equivalent “street foods” as “foods and beverages prepared and/or sold by vendors in streets and other public places for immediate consumption or consumption at a later time without further processing or preparation” (WHO, 1996). Street-vended foods are considered as a major public health risk, because there is lack of basic infrastructure and services for food preparation and there are difficulties in controlling large numbers of street food vending operations due to their diversity, mobility, and temporary nature (Ghosh et al., 2007). It is recognized that street food vendors are generally uneducated and belong to poor socioeconomic groups (WHO, 1996). Inadequate knowledge of street food vendors about basic food safety measures poses risks of spreading foodborne diseases within the community (Rane et al., 2011).
In Bangladesh, a large number of workers have chosen their occupation as street food vendors, and there are as many as 200,000 street food vendors working in Dhaka city (Faruque et al., 2010). Some of them are vending various food items targeting school-going children around several school-based locations. School-going children have become accustomed to consuming attractive and colorful food items from the school-based street food vendors. A description of some local food items that are typically sold to schoolchildren is illustrated in Table 1. However, it is questionable how knowledgeable the school-based street food vendors are about basic food safety issues, and how aware they are about the health of their customers (i.e., schoolchildren). Considering the above circumstances, we conducted a study to find out the current level of knowledge and awareness about children's food safety issues among the school-based street food vendors in Dhaka city.
Materials and Methods
This descriptive cross-sectional study was initiated by the Epidemiology Unit, Department of Microbiology, Institute of Public Health (IPH), Dhaka, Bangladesh in cooperation with the Department of Public Health Laboratory (PHL). The study was conducted for a period of 3 months. In this study, school-based street food vendors were those who vended different local food items among the schoolchildren during school hours at the school entrance, or at the side of outer school wall, or on the streets around the school within approximately 50 m from the school entrance or outer school wall of any primary or high school within the area of Dhaka City Corporation (DCC).
A total of 19 different school zones of Dhaka city and its outskirts were selected as study places. A total of 80 primary/high schools were included in this study. Representation of schools from all the 19 zones was ensured. A total of 262 school-based street food vendors were selected conveniently from surrounding areas/streets of the pre-selected primary and high schools. Nonprobability convenience sampling technique was employed for selection of schools and study participants due to logistic constraints. School-based street food vendors, who were available at the spot during the period of data collection and gave informed consent, were interviewed.
Face-to-face interviews were conducted by four well-trained field data collectors employing a pre-tested questionnaire. The time to complete each interview was approximately 30 min. Pre-testing of the questionnaire was performed among 20 school-based street food vendors by the researchers themselves. After necessary amendment, we finalized a three-page structured questionnaire consisting of 24 closed and open-ended questions for data collection. The questionnaire was composed of three parts. First part of the questionnaire included general characteristics of school-based street food vending like location of food vending, type of food item vended, number of child customer per day, and source and purification system of drinking water for child customers, while the second part of the questionnaire was related to sociodemographic profile of the school-based street food vendors comprising age, sex, educational status, and daily income. Moreover, several knowledge and awareness related variables such as name of common food-/waterborne illnesses, causes of spreading food-/waterborne diseases, causes of contamination of food/water in food shops, artificial color and chemicals in food, and methods of food-/waterborne disease prevention were included in the third part of the questionnaire. Knowledge and awareness part of the questionnaire was a combination of eight-item questions, structured in yes/no or yes/no/don't know, or in a defined set of possible multiple answers with an additional open-ended option of “others (please specify).”
A scoring system was developed to assess the level of knowledge and awareness of each participant. A score of 1 point was assigned for each correct answer, while a score of 0 point was given for each incorrect answer or each “don't know” response. We found a total of 31 correct responses by summing up all single and multiple correct responses obtained from the knowledge and awareness related questions asked to the respondents (Table 2). According to 31 correct responses, we set the total score for measuring level of knowledge and awareness as 31.
Multiple responses.
Method of measuring knowledge and awareness level has been illustrated in the Materials and Methods section of the article.
A cutoff point of 40% score was determined to categorize the level of knowledge and awareness into two grades by applying a criterion-referenced grading system known as The Angoff Mehod (Angoff, 1971, 1984; Carlson et al., 2009; Ricker, 2006). For this purpose, a five-member panel of food safety experts (including the researchers) was formed. The panel members individually reviewed each item of the knowledge and awareness related questions and possible answers, and estimated what percentage of minimally competent school-based street food vendors would answer each item correctly. The estimated ratings for each item were averaged, and those averages were used to determine the overall cut score. We preferred The Angoff Method, because it is a well-established, reliable, and credible approach for setting a standard cutoff score to separate minimally competent persons from non-minimally competent persons (Carlson et al., 2009; Ricker, 2006). Study-participants who scored 13–31 (>40% of total score) were considered to have adequate knowledge and awareness, while they were regarded as having inadequate knowledge and awareness if they scored 0–12 (≤40% of total score). To define the adequacy of the knowledge levels, we conducted a sensitivity analysis by using a cutoff point of the median score as an approach of norm-referenced grading system.
Statistical analysis
After completion of data collection, our study team reviewed all data for validity and consistency. Data were entered into Microsoft Access 2003 (Microsoft, Redmond, WA) and were analyzed by using SPSS 12 for Windows (SPSS, Chicago, IL). We used multivariable logistic regression model to determine the association between selected sociodemographic characteristics of school-based street food vendors and their level of knowledge and awareness (adequate=1; vs. inadequate=0). We entered all the selected independent variables (age, education, and income) in the model as an exploratory evaluation of all selected variables. Classification tables, omnibus tests of model coefficients and Nagelkerke's R2 were used to test the model fit for the logistic regression model. Statistical comparisons of different variables were shown by determining the crude and adjusted odds ratios (OR) along with 95% confidence interval (CI). We performed two-sided significant tests, where a p-value of<0.05 was accepted as the level of statistical significance.
Results
Of the 262 school-based street food vendors approached, 250 food vendors provided consent and took part in the interviews indicating a response rate of 95.42% for this study. Our study revealed that the school-based street food vendors used to vend a variety of local food items for their child customers around the schools (Table 1). Of total 250 food vendors interviewed, more than one third (37.2%) vended chotpoti and fuchka, 20.8% vendors kept achar for sell, another 20.8% sold fruit slices, 14.8% had jhalmuri and vajavuji items, and 17.2% had ice cream, 10% had biscuits and tea, 7.2% sold fast food and soft drinks, and 4.4% shops had other food items such as chanachur, sharbat, banana, and bread.
Regarding the sociodemographic profile of 250 school-based street food vendors, all (100%) were male with a mean age of 30.95±8.8 years, ranging from 15 to 52 years. The highest number (40.1%) of the vendors belonged to the age group 25–34 years. While comparing their education level categories, majority (43.6%) did not have any formal education, 23.2% attended primary education but did not complete, another 23.2% completed primary education, and only 10% had an education higher than primary level. The mean daily income of the food vendors was found to be 131.16±62.54 Taka (1.97±0.94 USD) within a range between 50 Taka (0.75 USD) and 300 Taka (4.51 USD).
Knowledge and awareness level of the school-based street food vendors on children's food safety is illustrated in Table 2. Of 250 respondents, the majority (92.8%) heard of food-/waterborne diseases, though a notable portion (7.2%) never heard of it. When calculating overall level of knowledge and awareness of the school-based street food vendors by The Angoff Method (Angoff, 1971, 1984; Carlson et al., 2009; Ricker, 2006), it was revealed that majority (68%) of them did not have adequate knowledge and awareness on children's food safety, while about one-third (32%) respondents showed adequate level of knowledge and awareness in this regard (Table 2). The sensitivity analysis by using a cutoff point of the median knowledge score (10) also revealed a similar result pertaining to overall knowledge and awareness level of the respondents. Sources of the food-/waterborne disease–related information received by the school-based street food vendors are shown in Figure 1. Most (91.8%) of the food vendors knew food-/waterborne disease–related information from electronic media (radio, TV, and satellite).
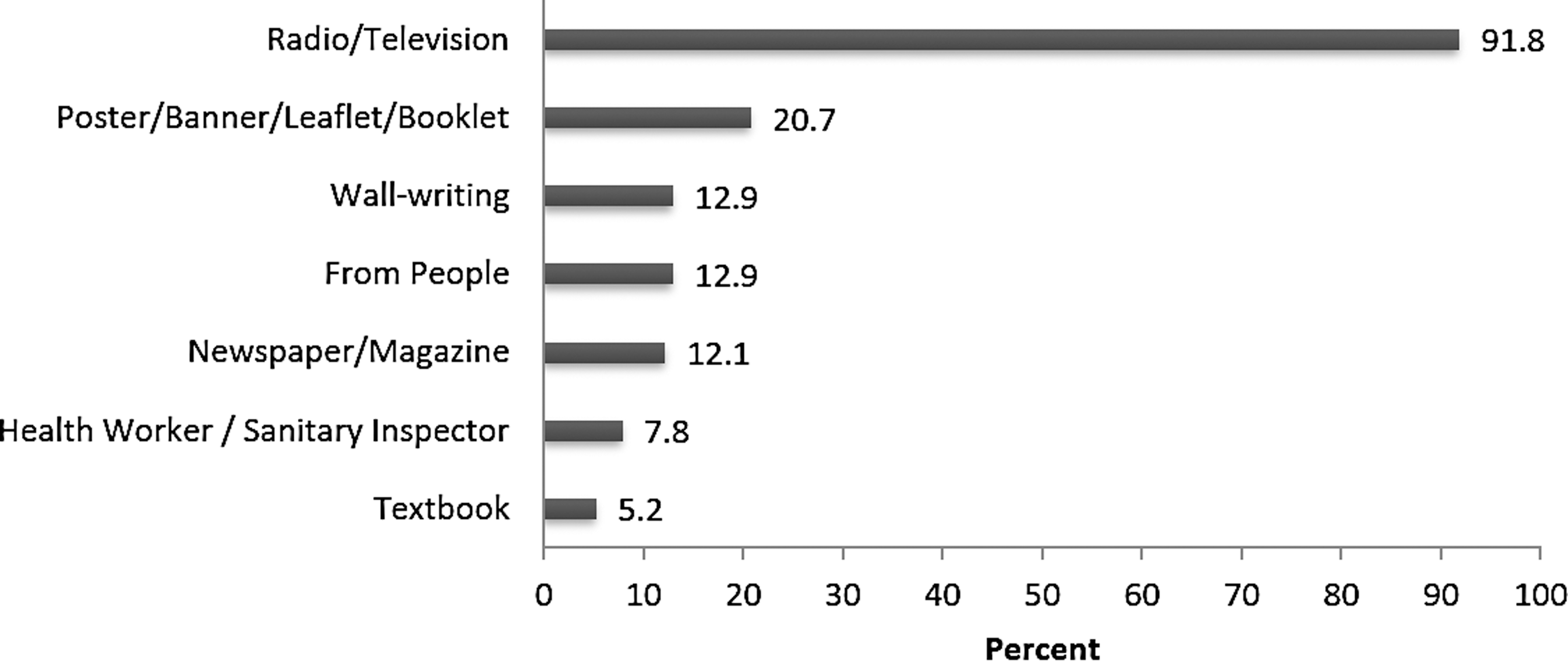
Sources (multiple responses) of food-/waterborne disease-related information received by school-based street food vendors (n=232), Dhaka, Bangladesh, 2006.
Crude and adjusted odds ratios for level of knowledge and awareness of school-based street food vendors related to selected sociodemographic characteristics are shown in Table 3. Logistic regression analysis showed that the school-based street food vendors aged 45 years or above were 17.73 times more likely to have adequate level of knowledge and awareness than the vendors belonged to age group 15–24 years (p<0.001; adjusted OR=17.73; 95% CI=4.38–71.73). School-based street food vendors who at least completed primary education (p<0.01; adjusted OR=6.58; 95% CI=2.2–19.65), and the vendors who had an education of higher than primary level (p<0.01; adjusted OR=9.87; 95% CI=2.07–46.93) were more likely to have adequate knowledge and awareness than those who did not have any formal education (Table 3). However, the logistic regression model showed a modest fit of the data to the model.
Age group, educational status, and daily income were included in the model.
Eight cases are missing for this variable (n=242).
Reference category.
Ranging from 6 to 11 years of education.
Eighteen cases are missing for this variable (n=232).
OR, odds ratio; CI, confidence interval; BDT, Bangladeshi Taka; 1 US Dollar=66.50 BDT (during study period).
Discussion
The present study revealed that the food items vended by the school-based street food vendors particularly chotpoti-fuchka, achar, jhalmuri, and vajavuji were very popular and attractive street foods among the school-going children (Table 1). Usually these preparations are thoroughly cooked, fried or deep-fried. There is little possibility of contamination with microbes during cooking, although the risk varies from mild to high depending upon the contamination during handling, serving, or preserving. We did not find any female school-based street food vendor in our study places indicating that women are still away from this occupation in Bangladesh. On the other hand, 20–53.6% of the street food vendors were female in a study conducted in Mexico (Estrada-Garcia et al., 2004).
In our study, the mean age of the school-based street food vendors was 31 years, which was similar to the mean age of 28 years found among the ice cream vendors in the streets of Phnom Penh city (Kruy et al., 2001). In our study, the low mean daily income of the school-based street food vendors illustrating a poor socioeconomic condition of this self-employed group of population. In this study, more than two-third of respondents showed inadequate level of knowledge and awareness, which was similar to the result of other relevant studies performed among food vendors in Iran (Askarian et al., 2004), Dakar (Aidara-Kane et al., 2000), Ghana (Mensah et al., 2002), and Indonesia (Vollaard et al., 2004).
Older school-based street food vendors were more likely to have higher level of knowledge and awareness because they might be more experienced in food vending practice than the younger individuals. Similarly, older food service workers had better knowledge and attitude regarding food hygiene in Iran (Askarian et al., 2004). The present study also illustrated that the level of knowledge and awareness of school-based street food vendors were significantly associated with their educational status, while a study done in Malta showed that the level of food safety knowledge and awareness among the food handlers was associated with their previous exposure to salmonellosis (Gauci et al., 2005). The food vendors studied in Jakarta (Vollaard et al., 2004) and Phnom Penh (Kruy et al., 2001) cities showed overall low level of education which was similar to our study result.
The present study revealed that electronic media (radio, television, and cable/satellite television) were the main sources of knowledge and information for most of the school-based street food vendors. Currently, electronic media has been flourished as a strong education media all over the world, including Bangladesh. Therefore, these electronic media can be utilized straightforwardly to increase the level of knowledge and awareness of the school-based street food vendors regarding children's food safety issues.
There are no data available regarding the foodborne outbreak associated with street food vendors in Bangladesh so far. Findings of a recent study (Faruque et al., 2010) conducted in Dhaka city showed that about 58% of the street food vendors did not cover their food while selling, and 88% vendors used stored water for cleansing of utensils. Furthermore, the study (Faruque et al., 2010) revealed that all (100%) of the street food samples had medium to high risk potentiality in terms of total viable microbial load and medium to low risk potentiality in terms of total coli form count. It is likely that bacterial contamination resulted from the use of contaminated water as well as due to the unhygienic condition of the vending itself (Faruque et al., 2010). There is no existing law, policy, or guidelines on street food vending in Bangladesh. As a result, the vendors operate their business informally and haphazardly. Street food vending is under any regulation nor under any organized monitoring system. Faruque et al. (2010) confirmed that 100% street food vendors had no formal training on food safety as well as food serving/handling, and more than 90% vendors were neither supervised nor monitored by any authority.
In the present study, classifying respondents as having adequate or inadequate knowledge and awareness was based on a criterion-referenced grading system The Angoff Method (Angoff, 1971, 1984; Carlson et al., 2009; Ricker, 2006). This system ensures a fair and defensible rationale for determining a cutoff score, because each participant's performance is established independently of the group who participated for assessment by comparing with clearly stated criteria and standards for particular levels of performance, while in norm-referenced method a participant's performance is directly influenced by the performance of other participants in the group (James, 2002; CTL, 2006). In our study, the outcome of using criterion-referenced grading system showed that an adequate level of knowledge and awareness among school-based street food vendors was reflected by an apparently low score representing at least 41% of the correct responses. However, we are convinced of our result based on the sensitivity analysis we conducted, which showed no drastic differences.
Because we conducted the present study exclusively with school-based street food vendors, the study might be considered as a pilot research of its kind in Bangladesh. However, a limitation of the study was the severe time constraint faced by the whole research team to complete the assignment within a strict timeline. A non-probability convenient sampling technique was adopted for selection of schools and the school-based street food vendors during interview due to time and fund constraints, and unavailability of appropriate sampling frame. Therefore, our study participants should not be considered as a representative sample for generalization of the study result, and caution should be used in interpreting the results since it was a convenience sample. Moreover, our logistic regression results should be interpreted with caution because the model showed modest fit, and further studies with bigger sample sizes are recommended to confirm our findings. Since our study is a pilot one, it would provide a first round impression about the school-based street food vendors in Dhaka city to the future investigators in the same discipline.
Conclusion
The present study revealed that more than two-thirds of the school-based street food vendors did not have adequate level of knowledge and awareness of foodborne diseases and food hygiene, posing a warning to the schoolchildren's food safety in Dhaka city. Our study recommends that pertinent health authorities and DCC should initiate appropriate training programs (e.g., using electronic media) for school-based street food vendors of Dhaka city on foodborne illness, food safety, and food hygiene. Simultaneously, incorporation of food safety and food hygiene messages into textbooks and school curriculum would provide opportunities for increasing awareness of children regarding food safety, as recommended by WHO (WHO, 1996).
Footnotes
Acknowledgments
We gratefully acknowledge funding from the Health, Nutrition and Population Sector Program (HNPSP), Directorate of Planning and Research, Directorate General of Health Services, Dhaka, Bangladesh. Moreover, we would like to thank Dr. Md. Rafiqul Islam (Former Director, IPH, Dhaka, Bangladesh) for his continuous support to carry out the research project.
Disclosure Statement
No competing financial interests exist.