
Abstract
Fresh salsa and guacamole often contain diced raw produce, are often made in large batches, and are often poorly refrigerated, which may make them prone to contamination that can cause foodborne illness. The safety of salsa and guacamole is increasingly important as these foods gain popularity. Since 1973, local, state, and territorial health departments have voluntarily reported foodborne disease outbreaks to the Centers for Disease Control and Prevention's Foodborne Disease Outbreak Surveillance System (FDOSS) using a standard reporting form. FDOSS used paper-based reporting for 1973–1997 and switched to electronic reporting for 1998–2008. We reviewed all reports of outbreaks during 1973–2008 in which salsa or guacamole was reported as a vehicle. We found 136 outbreaks in which salsa or guacamole was reported as a possible vehicle, which resulted in 5,658 illnesses. Of these 136 salsa- or guacamole-associated (SGA) outbreaks additional possible food vehicles were reported for 33 (24%) outbreaks. There were no SGA outbreaks reported before 1984. Among reported outbreaks, most were caused by norovirus (24%), nontyphoidal Salmonella (19%), and Shigella (7%). Eighty-four percent of outbreaks were caused by foods prepared in restaurants or delis; of these, 19% reported ill foodworkers, and 29% reported improper storage as possible contributing factors. Among all foodborne disease outbreaks with a reported food vehicle during 1984–1997, 26 (0.9%) of 2,966 outbreaks were SGA, and during 1998–2008, 110 (1.4%) of 7,738 outbreaks were SGA. The number of reported foodborne disease outbreaks attributable to salsa or guacamole increased in the United States from 1984 to 2008, especially in later years, and especially in restaurants. Fresh salsa and guacamole require careful preparation and storage. Focused prevention strategies should reduce the risk of illness and ensure that these foods are enjoyed safely.
Introduction
A
Salsa and guacamole are often identified with Mexican-style cuisine. Among outbreaks associated with ethnic cuisine during 1990–2006, salsa and guacamole were responsible for 13% of outbreaks associated with Mexican-style cuisine (Franco et al., 2009). However, studies limited to outbreaks caused by ethnic or Mexican-style cuisine do not give a complete picture of the contribution of salsa and guacamole to the total burden of foodborne disease outbreaks in United States.
Describing foodborne infections attributable to salsa and guacamole can help determine the risks associated with such foods and encourage measures to keep these foods safe (Campbell et al., 2001; Wheeler et al., 2005). We analyzed reports of all foodborne disease outbreaks reported to the U.S. Centers for Disease Control and Prevention (CDC) during 1973–2008 to describe salsa- or guacamole-associated (SGA) outbreaks and to assess the proportion of outbreaks attributable to contaminated salsa or guacamole.
Materials and Methods
Data source
Since 1973, local, state, and territorial health departments have voluntarily reported foodborne disease outbreaks to CDC's Foodborne Disease Outbreak Surveillance System (FDOSS) (Lynch et al., 2006). States began reporting outbreaks electronically in 1998. Concurrently, outbreak detection and reporting was enhanced by soliciting outbreak reports actively, revising the FDOSS outbreak reporting form, and introducing PulseNet, the national molecular subtyping network for foodborne pathogens (Olsen et al., 2000). Outbreak data are captured using a standard reporting form completed by health department personnel. Information captured in the reporting form includes implicated food vehicles (as a free text field); confirmed or suspected pathogenic etiology; number of illnesses, hospitalizations, and deaths; aggregate symptom profiles; aggregate demographic data; investigation methods; outbreak setting; and factors possibly contributing to the outbreaks.
Definitions
We queried the FDOSS database for all outbreaks with a food vehicle reported. We considered an outbreak to be “salsa- or guacamole-associated” if at least one reported food vehicle was salsa, guacamole, pico de gallo, or a spelling variation of these three foods. Pico de gallo is a variety of Mexican-style salsa often made with raw diced tomatoes, onions, jalapeño peppers, and cilantro. We classified pico de gallo as a salsa.
Multiple vehicles could be reported for an outbreak. If any reported vehicle in a given outbreak was salsa or guacamole, we classified the outbreak as SGA. If a specific ingredient in salsa or guacamole was the only reported food vehicle, then that outbreak was not captured in our query. Outbreaks where exposure to the implicated food occurred in more than one state were considered multistate outbreaks.
Etiologies were “confirmed” if there was laboratory evidence of the pathogen responsible for the outbreak in clinical samples from ≥2 patients or in the implicated food (CDC, 2006). Confirmation does not require the pathogen to be detected in all outbreak-associated cases, if an epidemiologic link to a confirmed case exists. Multiple etiologies could be reported.
“Restaurant-associated outbreaks” were defined as outbreaks in which at least one of the settings of food preparation was reported as a restaurant or deli. In restaurant-associated outbreaks, ill foodworkers were deemed a possible contributing factor if “Was a foodworker implicated as the source of contamination?” was answered “yes.” Food held at an inappropriate time or temperature was deemed a possible contributing factor if “food allowed to remain at room temperature,” “food prepared before serving and held,” or “inadequate cold-holding temperatures” was marked “yes.”
Statistical analysis
We determined the distribution of all SGA outbreaks and associated illnesses by year, state, and etiology. We also determined the distribution of illnesses by age and sex. For each etiology, we summarized outbreaks by magnitude (the number of illnesses, hospitalizations, and deaths), seasonality, outbreak setting, and contributing factors. We used Pearson's chi square test when comparing groups.
Results
Number and magnitude of outbreaks
From 1973–2008, we identified 136 outbreaks possibly attributable to salsa (n=96), guacamole (n=35), or both (n=5), among 11,455 foodborne disease outbreaks with at least one food vehicle reported to CDC (Table 1). The first reported SGA outbreak occurred in 1984 (Fig. 1). From 1984–1997, a median of two SGA outbreaks was reported per year, with a median of 41 illnesses per outbreak. From 1998–2008, the median number of outbreaks reported per year increased to 11, and the median number of illnesses per outbreak reported decreased to nine. SGA outbreaks were reported in 31 states, with no clear geographic pattern. Only one multistate SGA outbreak was reported.

Number of salsa- or guacamole-associated outbreaks and median number of illnesses per outbreak by year, Foodborne Disease Outbreak Surveillance System, United States, 1973–2008. PulseNet is the national molecular subtyping network for foodborne pathogens. Outbreak surveillance was enhanced in 1998 by the introduction of electronic outbreak reporting, active solicitation of outbreak reports, and revisions to the outbreak reporting form.
Of the six outbreaks with multiple pathogens implicated, all were salsa-associated outbreaks, one had two confirmed pathogens reported (B. cereus and C. perfringens), and the remaining five had two suspected pathogens reported (B. cereus, C. perfringens, Campylobacter, nontyphoidal Salmonella, and Staphylococcus).
The 136 SGA outbreaks were responsible for 5,658 illnesses, 140 hospitalizations, and three deaths from 1984–2008. Age was available for 1,487 outbreak patients, of which 1,032 (70%) were aged 20–49 years. Fifty-one percent of patients were female. Patient demographic characteristics did not differ significantly by etiology or by food vehicle.
Etiologies
Of all 136 SGA outbreaks, most were caused by norovirus (24%), nontyphoidal Salmonella (19%), and Shigella (7%); 10 other pathogens accounted for 18% of outbreaks, multiple etiologies accounted for 4%, and 28% had no etiology reported (Table 1). Of the 98 (72%) outbreaks with a pathogen reported, 63 (64%) were confirmed and 35 (36%) were suspected.
Of all 5,658 illnesses that occurred in SGA outbreaks, most were caused by nontyphoidal Salmonella (33%), norovirus (17%), and Shigella (14%); 10 other pathogens accounted for 11% of illnesses, multiple etiologies accounted for 1%, and 23% had no etiology reported (Table 1). Excluding a single, large outbreak of enteroinvasive E. coli infections (370 cases), Campylobacter outbreaks had the greatest median number of illnesses per outbreak (27), followed by Shigella (25), nontyphoidal Salmonella (24), and Salmonella enterica serotype Typhi (21). The three reported deaths were attributed to Shigella (1) and Clostridium botulinum (2). Both botulism deaths occurred in the same outbreak, from salsa prepared in a private home.
Forty-seven percent of outbreaks of norovirus infection occurred in December–February, and 65% of outbreaks of nontyphoidal Salmonella infection occurred in June–August. A seasonal pattern was not found for outbreaks caused by other pathogens or outbreaks caused by unknown or multiple etiologies.
Outbreak settings and vehicle types
Most SGA outbreaks (114, 84%), occurred in a restaurant or deli (Table 1), compared with 55% of all foodborne disease outbreaks with identified vehicles during the same time period (p<0.001). Other settings of preparation for SGA outbreaks included homes (six outbreaks), caterers (four outbreaks), schools (two outbreaks), groceries (two outbreaks), and other or unknown settings (eight outbreaks). Of SGA outbreaks with contributing factor information available, ill foodworkers were reported as a possible contributing factor for 19 (19%) of 100 outbreaks for which foodworker information was available. Inappropriate food holding times or temperatures were reported as a possible contributing factor for 19 (29%) of 66 outbreaks that occurred in restaurants.
The SGA outbreaks we identified were almost exclusively caused by freshly prepared salsa or guacamole (132, 97%), not commercially produced products, which are typically heat- or pressure-treated. Commercially processed foods were reported as vehicles in only four outbreaks; three outbreaks occurred in restaurants with chips and salsa as the reported vehicle, and guacamole was the other reported vehicle. Pathogens were reported for only two of these outbreaks: nontyphoidal Salmonella and norovirus. Multiple possible food vehicles were reported for 33 (24%) of 136 SGA outbreaks, which included 19 (58%) reports of chips and salsa or guacamole. The other 14 outbreaks with multiple possible food vehicles in addition to salsa or guacamole included reports of Mexican-style foods (seven outbreaks) and other foods (seven outbreaks). Although non-tomato salsas, such as mango or pineapple salsa, were not reported as vehicles, we cannot be certain that all reported salsa vehicles were tomato-based.
Emergence of salsa and guacamole as vehicles of illness
Among 751 foodborne disease outbreaks with identified food vehicles reported to CDC from 1973–1983, no SGA outbreaks were reported. Among all foodborne disease outbreaks with an identified food vehicle from 1984–1997, 26 (0.9%) of 2,966 outbreaks were SGA, and from 1998–2008, 110 (1.4%) of 7,738 outbreaks were SGA (Fig. 2). Among restaurant-associated outbreaks with identified food vehicles, from 1984–1997, 15 (1.3%) of 1,198 outbreaks were SGA, and from 1998–2008, 101 (2.1%) of 4,844 outbreaks were SGA (Fig. 3).
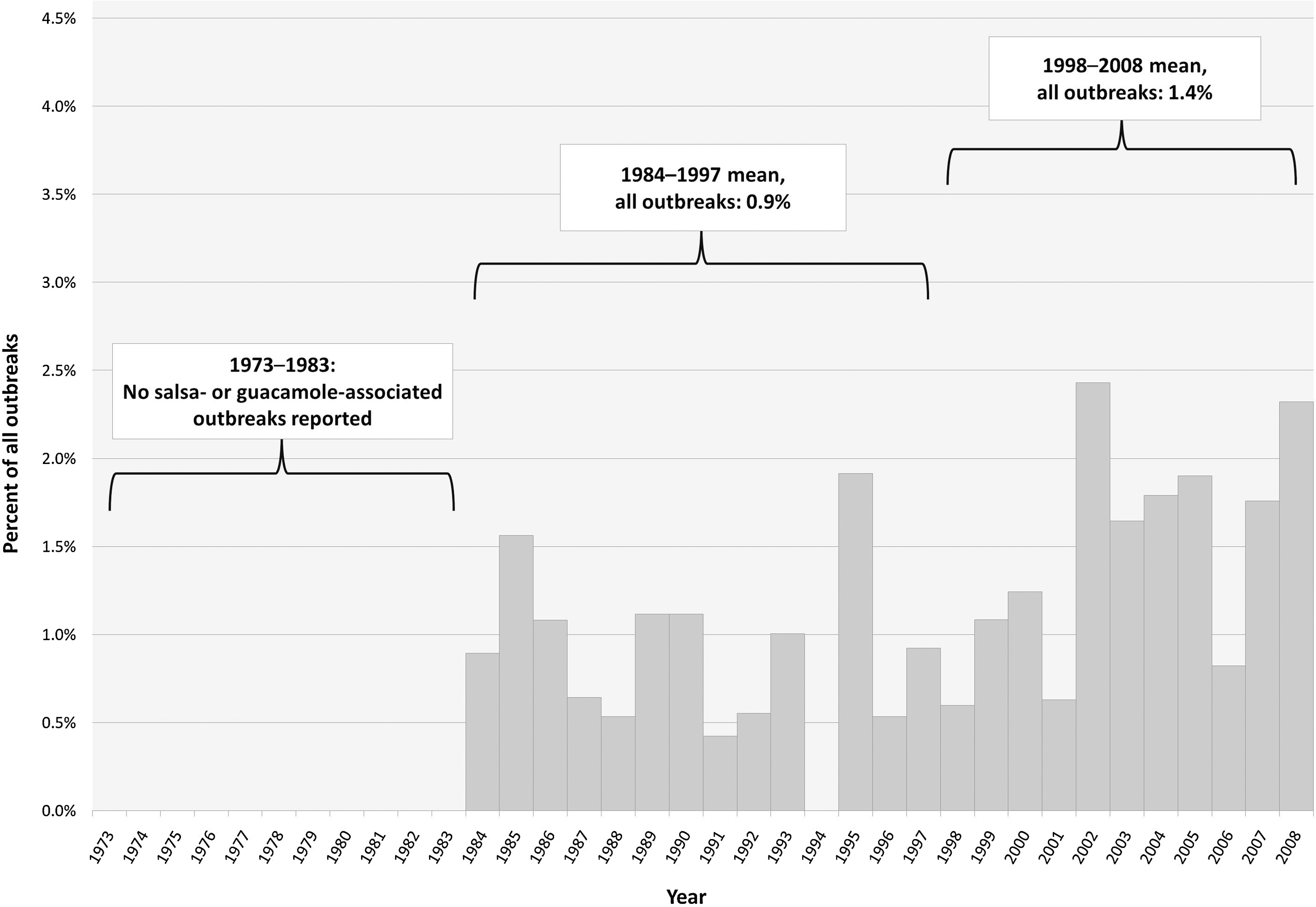
Salsa- or guacamole-associated outbreaks as a percentage of all foodborne disease outbreaks with an identified food vehicle, Foodborne Disease Outbreak Surveillance System, United States, 1973–2008.
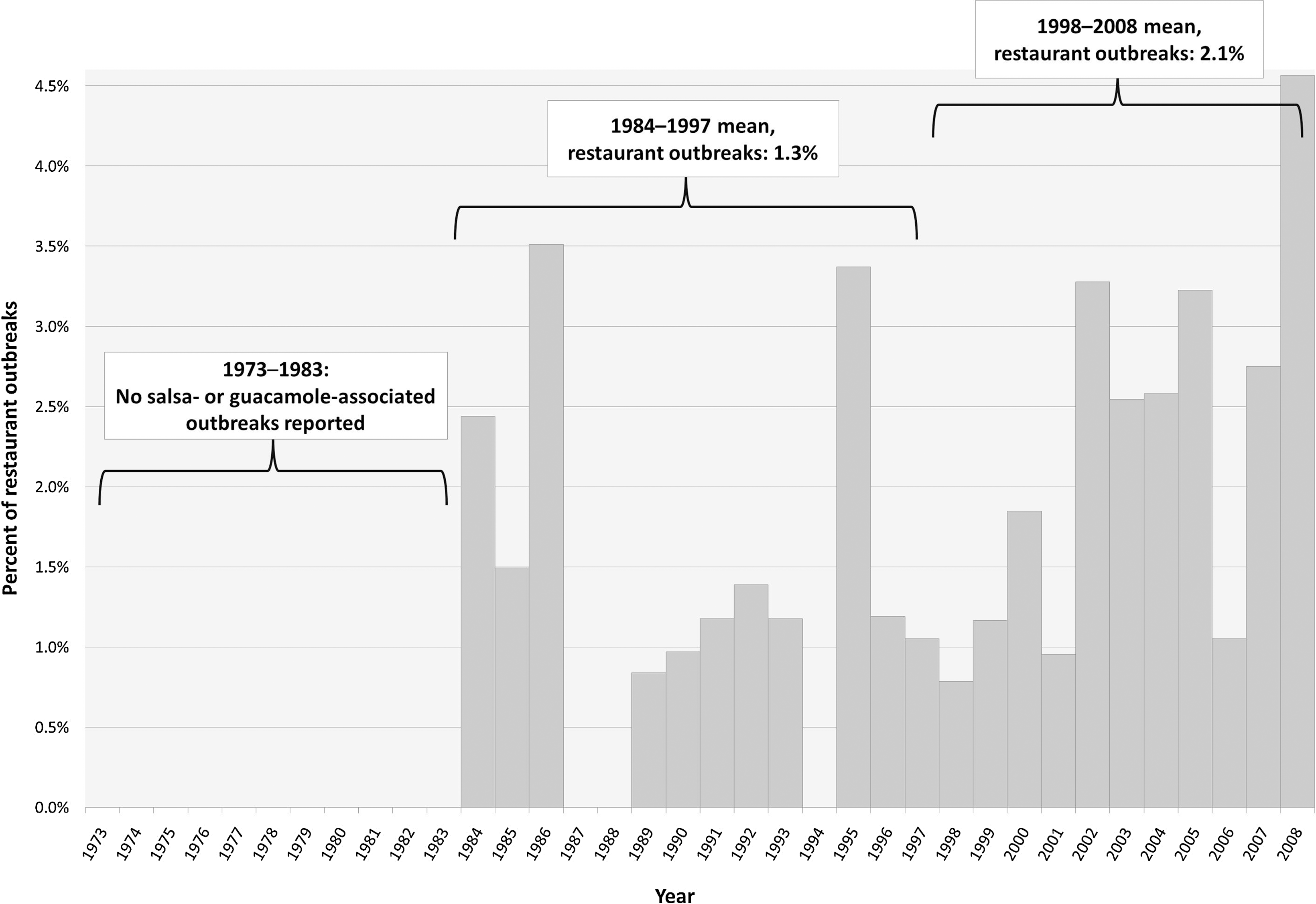
Restaurant-associated salsa- or guacamole-associated outbreaks as a percentage of all restaurant-associated foodborne disease outbreaks with an identified food vehicle, Foodborne Disease Outbreak Surveillance System, United States, 1973–2008.
When looking at a period with stable surveillance methodology, 1998–2008, the percentage of outbreaks that was SGA was generally greater in later years (from 2002–2008) than early years (from 1998–2001; Fig. 2). A similar but more pronounced increase was observed in SGA outbreaks that occurred in restaurant settings (Fig. 3).
Discussion
Salsa and guacamole are important sources of foodborne illnesses in the United States, and were possibly the vehicles for 136 reported outbreaks with 5,658 illnesses from 1984–2008. These outbreaks were caused by a variety of pathogens, including pathogens with human reservoirs and pathogens with animal reservoirs, which suggests several routes of contamination are responsible. Over the study period, the percentage of all foodborne disease outbreaks that were SGA increased, especially in restaurant settings. From 1998–2008, the percentage of foodborne disease outbreaks that were SGA increased substantially in later years, as did the percentage of restaurant-associated outbreaks that were SGA.
Changes in surveillance methods nationally since 1973, and variation in outbreak investigation and reporting by states, make it difficult to assess trends. Even from 1998–2008, a period with stable surveillance methodology, there was likely ongoing improvement in outbreak detection because of an increasing number of infections reported to PulseNet and improved diagnostic testing for norovirus at public health laboratories (Hall et al., 2012). By reporting SGA outbreaks as a proportion of all outbreaks with reported food vehicles, we attempted to control for changes in overall outbreak detection.
The specificity of reported food vehicles varies by each individual outbreak and by state. This poses a challenge in determining the exact number of outbreaks and illnesses attributable to salsa and guacamole. Our classification of outbreaks with multiple possible vehicles as SGA may lead to an overestimation of SGA outbreaks. Conversely, our definition of SGA outbreaks did not capture outbreaks in which the vehicle reported was a specific ingredient in salsa or guacamole (Barton Behravesh et al., 2011; Campbell et al., 2001; Mody et al., 2011; Wheeler et al., 2005).
The safety of salsa and guacamole is increasingly important as these foods gain popularity; since 1991, salsa has outsold ketchup in the United States (Weise, 2010). The number of Mexican-style restaurants in the United States grew more than 30% from 1998–2009 and 15% from 2004–2009 (NPD Group, 2009). Salsa is not unique to Mexican-style cuisine; it is part of numerous Latin-American cuisines, Tex-Mex, and contemporary American cuisine, among others.
Ingredient quality may affect salsa and guacamole safety. Salsa and guacamole contain ingredients often implicated in produce-associated outbreaks. In 2008, a United States Department of Agriculture food safety program screened 3,437 samples of cilantro, hot peppers, tomatoes, and onions and found that nearly 1% of samples yielded Salmonella (MDP, 2009). Research shows that tomatoes with bruises, cut skin, or chill injury carry an increased opportunity for pathogens to infiltrate the fruit and multiply (Wade et al., 2003a,b,c; Wells, 1997). Tomatoes are graded according to quality; less than 5% of Grade 1 tomatoes, but up to 10% of Grade 2 tomatoes can be seriously damaged by bruises (USDA, 1997). Chefs may choose to use lower grade tomatoes for foods like salsa, reserving higher quality tomatoes for foods in which more of the tomato is visible to the consumer. We speculate that using lower quality tomatoes could increase the risk of contamination. Since salsa and guacamole are generally not cooked, there is no opportunity to kill pathogens that may have penetrated a tomato or other ingredients. Chefs may want to avoid the use of bruised tomatoes in these foods. Additionally, certain combinations of ingredients may make some salsas safer than others. Research shows that recipes containing lime juice and fresh garlic inhibit the growth of bacterial pathogens in contaminated salsa, regardless of storage temperature, whereas bacteria grew rapidly in contaminated salsa without these ingredients (Ma et al., 2010).
Several characteristics of fresh salsa and guacamole increase the risk of bacterial growth, if contaminated. Dicing or pureeing produce, typical for preparation of salsa and guacamole, creates a large cut surface area that can spread contamination and increases availability of nutrients that support the growth of pathogens like Salmonella (Asplund et al., 1991; Weissinger et al., 2000). Additionally, salsa and guacamole are frequently prepared and stored in large batches, allowing contamination of just a few ingredients, to pervade many servings (MMWR, 2008). Furthermore, salsa and guacamole may be inadequately refrigerated, thereby facilitating the growth of some foodborne pathogens (Campbell et al., 2001; Franco et al., 2010; Schmitt, 2003). Finally, placing fresh salsa on warm foods may increase microbial growth (Franco et al., 2010).
SGA outbreaks were significantly more likely to be reported as restaurant-associated, compared with all outbreaks with identified vehicles reported to CDC. In restaurants, reports of inappropriate time or temperature holding possibly contributed to 29% of SGA outbreaks with contributing factors reported. Although contributing factor information was not reported for all outbreaks and may not be definitive even when reported, our findings are consistent with another study that identified improper washing, cutting, and storage practices as contributing factors for contamination and proliferation of enteric bacterial pathogens in tomatoes served in restaurants (Kirkland et al., 2009). Foods containing diced tomatoes, such as salsa and guacamole, are considered potentially hazardous by the U.S. Food and Drug Administration's (FDA) Food Code and require storage time, temperature, or acidity controls (FDA, 2009).
The types of pathogens transmitted through salsa and guacamole indicate both human and non-human reservoirs as sources of contamination. Norovirus, Shigella, and Hepatitis A virus are examples of pathogens commonly transmitted by humans, which combined account for 44% of 98 SGA outbreaks with reported etiology. Pathogens with human reservoirs can contaminate foods anywhere from harvest to preparation in the kitchen. Ill foodworkers were reported as a possible contributing factor in about half of reported outbreaks of norovirus, Shigella, and Hepatitis A virus infections; some of the other outbreaks caused by these human-reservoir pathogens could have resulted from ingredients contaminated by humans before arriving in the kitchen. For example, in an outbreak of hepatitis A caused by green onions in salsa, the onions were apparently contaminated on the farm (Wheeler et al., 2005). Nontyphoidal Salmonella, Campylobacter, and E. coli O157:H7, pathogens with non-human reservoirs, accounted for a third of SGA outbreaks with an identified etiology. Ill foodworkers were reported as a possible contributing factor for a lower percentage of these outbreaks, suggesting that many of these outbreaks were caused by ingredients contaminated on the farm, in packing facilities, in transport, or by cross-contamination in kitchens.
Several practices can likely decrease the risk of SGA outbreaks. First, following good hand hygiene and food-handling practices in restaurants and home kitchens should minimize the risk of contamination and amplification of pathogens in these foods. Wash all produce thoroughly under running water before eating, cutting, or cooking; keep fruits and vegetables that will be eaten raw separate from other foods such as raw meat, poultry, or seafood, and from kitchen utensils used for those products; and store perishable fresh fruits and vegetables in a clean refrigerator at a temperature of 40°F or below (FDA, 2012). Second, a healthy workforce is crucial for the safe harvest and preparation of produce. Sick leave policies for field and restaurant workers and all others handling fresh produce that discourage employees from working when ill can reduce the risk of contamination by human-reservoir pathogens (Sumner et al., 2011). FDA's Guidance for Industry recommends policies for improved worker health; sanitation in the field, at packaging, and during transportation; and for other agricultural practices (FDA, 1998). Because methods to decontaminate produce are not highly effective, the key to preventing produce-associated outbreaks is preventing initial contamination by following such recommendations (Lynch et al., 2009). Third, adherence to safe food-handling practices in restaurants and other retail-settings could be enhanced by considering fresh salsas and guacamole prepared with diced produce items as potentially hazardous foods, thereby requiring time and temperature controls, unless their recipe is shown to inhibit pathogen growth. Although foods containing diced raw tomatoes are already considered potentially hazardous, diced produce items other than tomatoes, such as jalapeño peppers, support the growth of pathogens (FDA, 2009; Ma et al., 2010; Mody et al., 2011).
The increase in salsa and guacamole outbreaks reflects the growing popularity of ethnic foods and the expanding palate of the American population. Fresh salsa and guacamole are served at many restaurants and homes across the United States. Focused prevention strategies should reduce the risk of illness and ensure that these foods are enjoyed safely.
Footnotes
Acknowledgments
We thank Suzette Thedford, Olga Henao, Tracy Ayers, and Cathy Young for their valuable contributions to this manuscript, and state and local health departments for voluntarily reporting outbreaks to the Foodborne Disease Outbreak Surveillance System.
Disclosure Statement
No competing financial interests exist.