
Abstract
Background:
Shiga toxin–producing Escherichia coli (STEC) are an important cause of diarrhea and the major cause of postdiarrheal hemolytic uremic syndrome. Non-O157 STEC infections are being recognized with greater frequency because of changing laboratory practices.
Methods:
Foodborne Diseases Active Surveillance Network (FoodNet) site staff conducted active, population-based surveillance for laboratory-confirmed STEC infections. We assessed frequency and incidence of STEC infections by serogroup and examined and compared demographic factors, clinical characteristics, and frequency of international travel among patients.
Results:
During 2000–2010, FoodNet sites reported 2006 cases of non-O157 STEC infection and 5688 cases of O157 STEC infections. The number of reported non-O157 STEC infections increased from an incidence of 0.12 per 100,000 population in 2000 to 0.95 per 100,000 in 2010; while the rate of O157 STEC infections decreased from 2.17 to 0.95 per 100,000. Among non-O157 STEC, six serogroups were most commonly reported: O26 (26%), O103 (22%), O111 (19%), O121 (6%), O45 (5%), and O145 (4%). Non-O157 STEC infections were more common among Hispanics, and infections were less severe than those caused by O157 STEC, but this varied by serogroup. Fewer non-O157 STEC infections were associated with outbreaks (7% versus 20% for O157), while more were associated with international travel (14% versus 3% for O157).
Conclusions:
Improved understanding of the epidemiologic features of non-O157 STEC infections can inform food safety and other prevention efforts. To detect both O157 and non-O157 STEC infections, clinical laboratories should routinely and simultaneously test all stool specimens submitted for diagnosis of acute community-acquired diarrhea for O157 STEC and for Shiga toxin and ensure that isolates are sent to a public health laboratory for serotyping and subtyping.
Introduction
I
While O157 STEC is readily identified in the clinical laboratory by culture on a differential and selective medium such as sorbitol-MacConkey agar, there is no selective agar for isolation of non-O157 STEC strains (Gould et al., 2009). Culture-independent tests such as the enzyme immunoassay (EIA) detect the presence of the Shiga toxins and have facilitated the diagnosis of both O157 and non-O157 STEC infections. The number of non-O157 STEC infections detected has increased with an increasing number of laboratories using these culture-independent tests (Hoefer et al., 2010; Stigi et al., 2012).
Epidemiologic studies of non-O157 STEC infections in the United States have relied largely on convenience samples of isolates submitted to the Centers for Disease Control and Prevention's Enteric Diseases Laboratory for testing (Brooks et al., 2005), have focused on a limited number of laboratories, or describe only a single state or small geographic area (Bokete et al., 1993; Park et al., 1996; Fey et al., 2000; Jelacic et al., 2003; Klein et al., 2002; Lockary et al., 2007; Manning et al., 2007; Hedican et al., 2009; Lathrop et al., 2009; Hadler et al., 2011; Denno et al., 2012; Stigi et al., 2012).
Non-O157 STEC infection became a nationally notifiable disease in 2000. Since then, the Foodborne Diseases Active Surveillance Network (FoodNet) has conducted active, population-based surveillance for these infections. We present data from surveillance for non-O157 STEC from 2000 to 2010, provide estimates of the incidence of culture-confirmed non-O157 STEC infections, compare this with the incidence of culture-confirmed O157 STEC infections, and describe demographic characteristics and frequency of international travel by STEC serogroup.
Materials and Methods
FoodNet is a collaborative project of the Centers for Disease Control and Prevention, 10 state health departments, the United States Department of Agriculture's Food Safety and Inspection Service, and the United States Food and Drug Administration. Staff in FoodNet sites conducted active, population-based surveillance for laboratory-confirmed STEC infections in Connecticut, Georgia, Maryland, Minnesota, New Mexico, Oregon, and Tennessee, and selected counties in California, Colorado, and New York (Scallan, 2007). The percentage of the U.S. population included in FoodNet surveillance increased from 11% during 2000 to 15% during 2010. FoodNet personnel routinely contacted all clinical laboratories (≈650) serving the FoodNet sites to ascertain all culture-confirmed cases of STEC infection among residents.
A case of non-O157 STEC infection was defined as the isolation from a resident in the FoodNet surveillance catchment of STEC that expressed an O antigen other than 157 or for which the O antigen was not typable but was known to not express the O157 antigen, not be O-rough, and not have DNA encoding the O157 antigen. A case of O157 STEC infection was defined as the isolation from a resident of a FoodNet site of E. coli O157 that had the H7 antigen, produced Shiga toxin, or had a gene that codes for Shiga toxin production.
Demographic information, including age, gender, race and ethnicity, hospitalization, and death within 7 days of specimen collection, was submitted for each patient. Starting in 2004, site personnel systematically collected information on whether a case was associated with an outbreak, and whether the patient had traveled internationally during the 7 days before illness began (“internationally acquired” infection). To collect additional information on clinical signs and symptoms, site personnel completed a supplemental case report form for all confirmed cases of STEC infection reported during 2008–2009. Supplemental case report form data were extracted from each site's routine patient interview form. For some variables, data were not available for all sites.
Data on laboratory testing practices were obtained from a survey of 664 laboratories conducted in 2007 (Hoefer et al., 2010) and a subsequent survey of 448 laboratories conducted in 2010. Incidence per 100,000 persons was calculated for each gender and age group, based on annual population estimates from the U.S. Census Bureau (U.S. Census Bureau 2011). We compared the incidence of infection with non-O157 STEC with the incidence of O157 STEC infection by site during 2000–2010. STEC cases were further analyzed for proportion and incidence by age group, gender, and FoodNet site. The season of isolation was assigned based on the specimen collection date: winter (December, January, February), spring (March, April, May), summer (June, July, August), and fall (September, October, November).
The Wilcoxon rank-sum test was used to assess differences in age and length of hospital stay; differences in categorical variables were examined using chi-square tests. Spearman's correlation coefficient was calculated to examine the relationship between number of labs testing for Shiga toxin and number of STEC isolates reported each year. All statistical analyses were performed with SAS, Version 9.2 (SAS Institute, Cary, NC).
Results
Incidence and serotypes causing STEC infections
During 2000–2010, 2006 cases of non-O157 STEC infection and 5688 cases of O157 STEC infection were reported from the 10 FoodNet sites. An additional 29 isolates with the O antigen reported as “rough” were not included in further analyses. The incidence of non-O157 STEC infections increased from 0.12 per 100,000 population in 2000 to 0.95 per 100,000 in 2010. This increase correlated with an increase in the number of clinical laboratories performing culture-independent (EIA) testing for Shiga toxin (correlation coefficient=0.94, p<0.001; Fig. 1). The incidence of O157 STEC infections decreased from 2.17 per 100,000 in 2000 to 0.95 per 100,000 in 2010; O157 STEC infections did not correlate with the number of laboratories performing EIA testing for Shiga toxin (correlation coefficient=−0.38, p=0.25).
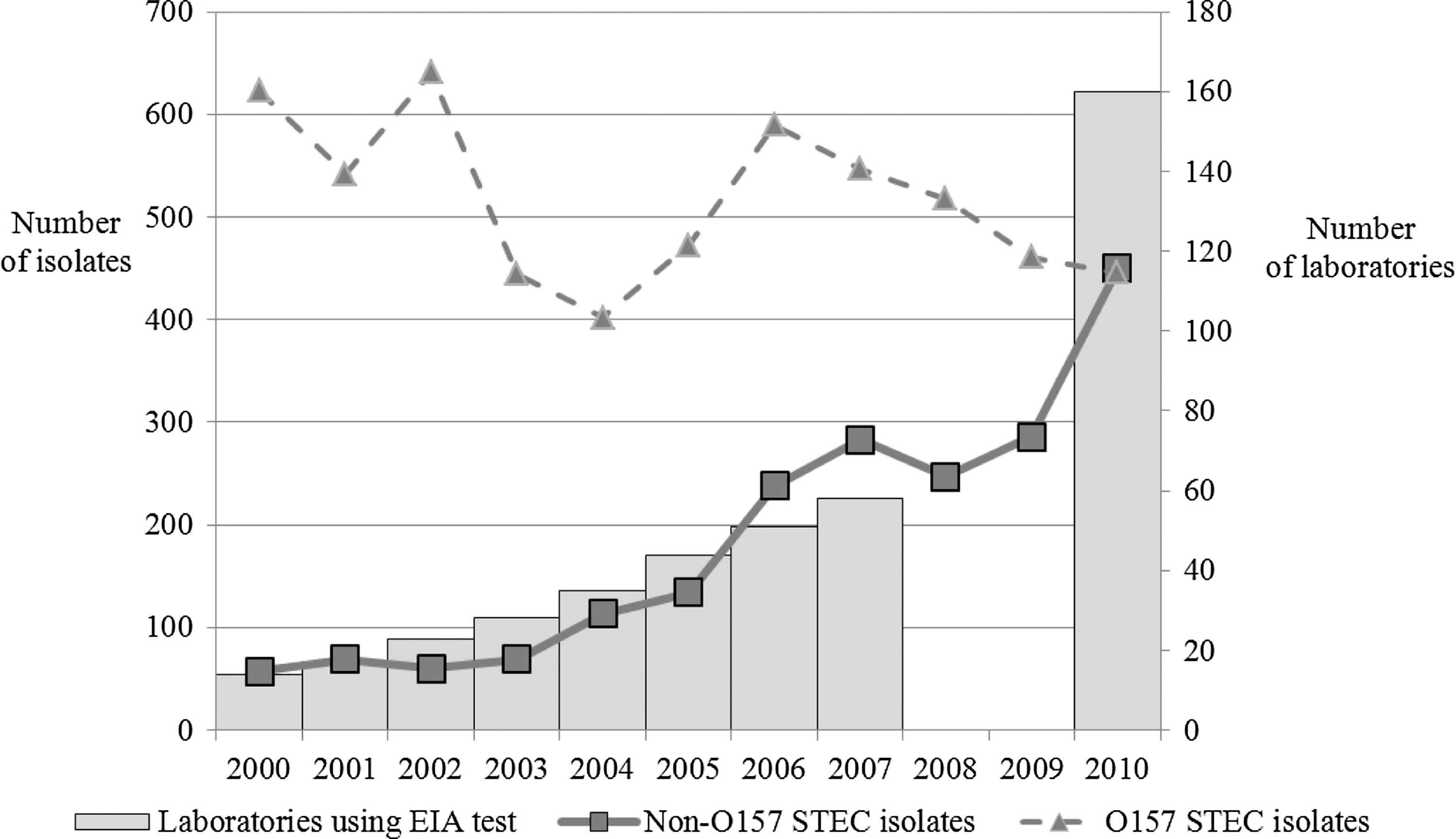
Number of non–O157 and O157 Shiga toxin–producing Escherichia coli (STEC) isolates reported to FoodNet sites and number of laboratories using culture-independent (enzyme immunoassay) tests for Shiga toxin (see Note), 2000–2010. EIA, enzyme immunoassay. Note: Data on laboratories are from 2007 FoodNet laboratory survey (Hoefer et al., 2010) and 2010 FoodNet laboratory survey (CDC, unpublished data). Data were not collected for 2008 and 2009.
The number and incidence of non-O157 STEC infections varied by FoodNet site, with the highest average incidence in New Mexico (1.14 infections per 100,000 persons) and the lowest in California (0.11 per 100,000) (Fig. 2). In New Mexico, non-O157 serogroups caused 66% of STEC infections, compared with only 9% in California and 8% in Oregon.
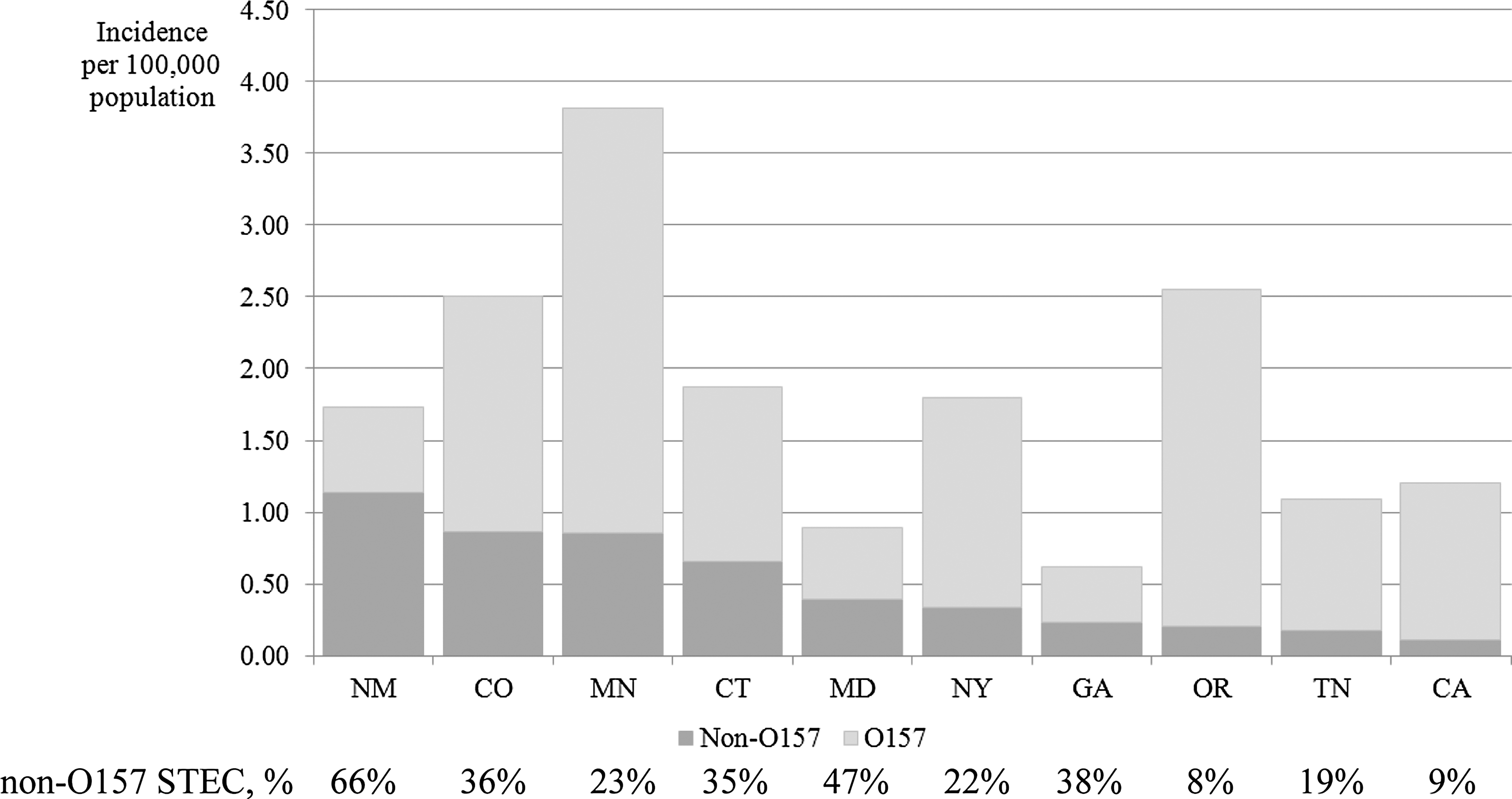
Average incidence per 100,000 population and the percent of Shiga toxin–producing Escherichia coli (STEC) infections caused by non-O157 STEC serogroups, by FoodNet site, 2000–2010.
The O antigen was reported for 1708 (85%) non-O157 STEC isolates. Seventy-one O antigens were reported, most commonly O26 (447 isolates, 26%), O103 (381, 22%), O111 (326, 19%), O121 (106, 6%), O45 (92, 5%), and O145 (64, 4%). Together, these six serogroups accounted for 83% of all non-O157 STEC isolates in which an O antigen was reported. The H antigen was reported for 1078 isolates. Of these isolates, the most common serotypes were O26:H11 (26%), O103:H2 (24%), and O111:NM (21%) (Table 1).
Demographic characteristics and exposures
Most demographic characteristics of persons infected with O157 and most non-O157 STEC serogroups were similar (Table 2). Similar proportions of persons with non-O157 and O157 STEC infections were female, and the median age of patients was similar. However, the median age of persons with an O45 infection (22 years) and O121 infection (29 years) was older than those infected with other serogroups and more persons with O121 infection were male; the demographic characteristics of O121 cases were likely affected by a large outbreak in an institutionalized population. For non-O157 STEC infections, the incidence was highest among children aged <5 years (1.89 per 100,000 persons), with a marked peak among children aged 1 year (3.93 per 100,000 persons) (Fig. 3). Incidence was lowest among adults aged 18–59 years (0.23 cases per 100,000) and ≥60 years (0.22). There was a higher proportion of persons of Hispanic ethnicity among those with non-O157 STEC infection (16% compared with 6% for O157 STEC, p<0.001) (Table 1). STEC infections, both non-O157 and O157, occurred most frequently during the summer months.
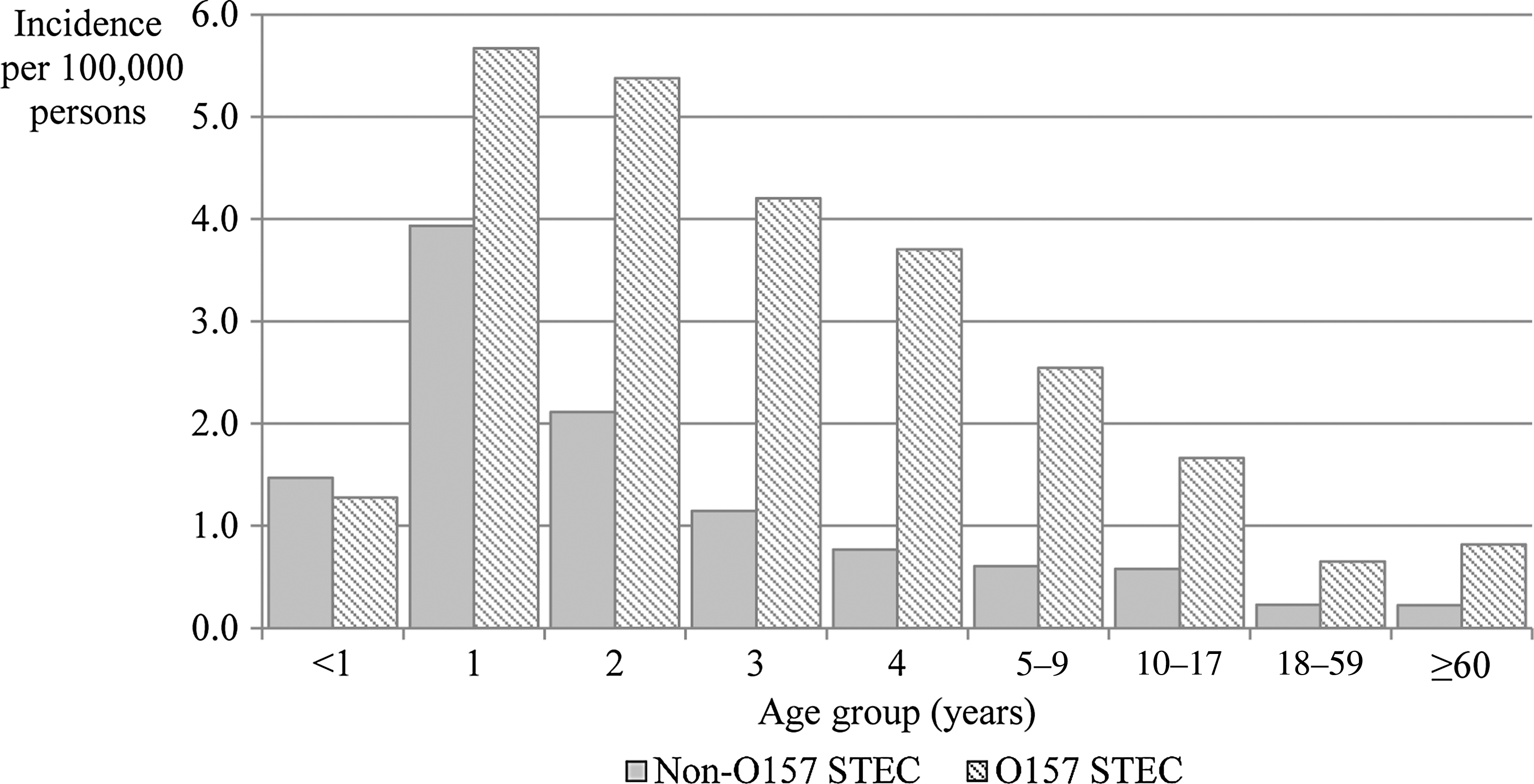
Incidence of non-O157 and O157 Shiga toxin–producing Escherichia coli (STEC) infections reported by the 10 FoodNet sites, by age group, 2000–2010.
Excluding the 35 outbreak-associated O121 cases, the characteristics and exposures differ as follows: 58% female, median age 22 years, 49% summer months, 76% resident of metropolitan county, 7% Hispanic ethnicity, 84% white race, 20% hospitalized, and 4% international travel. Excluding outbreak-associated cases of the other serotypes resulted in little change in demographic characteristics and exposures.
O26, O103, O111, O121, O45, and O145 accounted for 83% of all non-O157 STEC isolates in which an O antigen was reported. The remaining O antigens reported were O118 (2% of total), O91 (1%), O69 (1%), O165 (1%), O76 (1%), and O1, O2, O4, O5, O7, O8, O10, O15, O22, O24, O25, O28, O33, O43, O49, O50, O51, O55, O71, O73, O74, O80, O82, O84, O86, O87, O88, O96, O98, O104, O105, O109, O110, O113, O117, O119,O123, O124, O125, O126, O128, O130, O132, O140, O143, O146, O151, O153, O156, O159, O162, O163, O166, O172, O174, O175, O177, O178, O179, O181 (all <1%).
Indicates statistically significant (p<0.01) difference between non-O157 and O157 STEC.
Analysis includes only cases from 2004 to 2010.
An outbreak of O45 infections was reported in 2005 from a county in New York State not included in the FoodNet catchment area (
Travel destination information collected since 2008. Countries visited by non-O157 STEC case-patients were Mexico (59%), Dominican Republic (6%), Peru (4%), Costa Rica (3%), and Aruba, Bahrain, Bolivia, Brazil, Canada, Colombia, Dominica, El Salvador, France, Guatemala, Honduras, India, Israel, Italy, New Zealand, Nicaragua, Spain, Switzerland, Syria, United Kingdom, Uruguay, and Venezuela (<2% each).
Patients with non-O157 STEC infection were about one third as likely as those with O157 STEC to be associated with an outbreak (7% versus 20%, p<0.001) (Table 1). For each of the six most common non-O157 STEC serogroups, except for O121 STEC, there were no statistically significant differences among serogroups in demographic characteristics between outbreak-associated and sporadic cases (Table 1).
Patients with non-O157 STEC infection were five times more likely than those with O157 STEC infection to have traveled internationally during the 7 days before specimen collection (15% versus 3%, p<0.001) (Table 1). The proportion of cases that were internationally acquired varied by serogroup: 21% of patients with O103 infection, 20% of those with O111 infection, and <10% of patients infected with the other most common non-O157 STEC serogroups. The travel destination was reported only in 2008–2010. Among these 115 non-O157 STEC case-patients, 109 visited a single country, and Mexico was the most common country reported (64 cases, 59%). Among the 32 O157 STEC case-patients for whom the travel destination was known, 41% traveled to Mexico.
Hospitalization and clinical characteristics
Patients with non-O157 STEC infection were less likely to be hospitalized than those with O157 (14% versus 43%, p<0.001). Although the median duration of hospitalization was the same for non-O157 and O157 STEC infections (3 days), patients with O157 STEC infection tended to have longer hospital stays than those with non-O157 STEC infection (p=0.002). Among non-O157 STEC cases, the proportion hospitalized varied by serogroup, from 10% of those with O26 STEC to 28% of those with O145. More patients with O45 and O145 STEC infection were hospitalized than those infected with other non-O157 STEC serogroups (p<0.001). Among O157 STEC cases, 33 deaths (0.6%) were reported, compared with two deaths (0.1%) among those with non-O157 STEC infection (p=0.0042). One was in a person with an O156 infection; in the other, the serogroup was not reported.
Data on other clinical characteristics of STEC infections was available for cases reported in 2008 and 2009. Infection with O157 STEC generally caused more severe illness than infection with non-O157 STEC. Nearly all patients with either O157 (99%) or non-O157 STEC infection (99%) had diarrhea, but bloody diarrhea was reported more frequently by those with O157 infection (85 versus 55%, p<0.001) (Table 3). Abdominal pain was also more common in O157 infection (87% versus 80%, p=0.003), as was vomiting (42% versus 25%, p<0.001). Eleven percent of persons with O157 STEC infection developed physician-diagnosed HUS, compared with 1% of those with non-O157 STEC infection (p<0.001). The four cases of HUS among persons with non-O157 STEC infection were associated with serogroups O111 (two cases), O103, and O121.
Information was obtained from a combination of chart review and self-report, depending on the site.
Not all sites asked about each feature. The denominator (N) varied depending on the number of sites asking about a feature.
Indicates statistically significant (p<0.01) difference between non-O157 and O157 STEC.
The Shiga toxin type was reported for 941 of 1266 (74%) non-O157 STEC isolates and 1213 of 1973 (61%) O157 STEC isolates during 2007–2010. Of the non-O157 STEC isolates, 74% had Stx1 only, 17% had Stx2 only, and 9% had Stx1 and Stx2. Of the O157 STEC isolates, 2% had Stx1 only, 47% had Stx2 only, and 51% had Stx1 and Stx2. Patients with isolates that had Stx2 were more likely to be hospitalized than those that had isolates with Stx1 only (38% versus 12%, p<0.001). All cases of HUS occurred among patients with isolates that had Stx2.
Discussion and Conclusions
The number of non-O157 STEC infections reported in FoodNet sites increased substantially during the past decade. By 2010, for the first time, the rate of non-O157 STEC infections equaled that of O157 STEC infections. This increase was strongly correlated with a concomitant increase in the number of laboratories testing for Shiga toxin using the enzyme immunoassay and is thus most likely because of changes in laboratory testing. In 2003, 2% of clinical laboratories reported testing all stool specimens using a test that would detect the Shiga toxins; by 2007, this had increased to 4%, and 11% of laboratories reported using these tests at least some of the time (Hoefer et al., 2010). A similar relationship between laboratory testing and detection of non-O157 STEC infections was reported from Washington State (Stigi et al., 2012). As more laboratories implement culture-independent testing for the Shiga toxins, the number of non-O157 STEC reported will continue to increase (Hoefer et al., 2010).
We found marked variation in the ratio of non-O157 to O157 STEC by FoodNet site that is also explained, at least to some degree, by differences in testing practices. In some sites where most of the large reference laboratories routinely test for Shiga toxin (Hoefer et al., 2010) (e.g., Maryland and New Mexico), more than half of STEC were non-O157 serogroups, whereas in sites where fewer laboratories test for Shiga toxin (e.g., California and Oregon), fewer non-O157 STEC were reported. For example, in Minnesota, most non-O157 STEC were detected at two sites that conducted enhanced surveillance and routinely tested for non-O157 STEC. In these two sites, nearly 50% of the reported STEC were non-O157 serogroups; in the rest of the state, where testing for non-O157 STEC was not routine, only one quarter of STEC were non-O157 (Hedican et al., 2009). As more laboratories implement testing for Shiga toxin, further studies should examine whether geographic differences persist. In smaller studies in individual states or regions, non-O157 STEC have been estimated to account for 30–64% of STEC infections (Fey et al., 2000; Jelacic et al., 2003; CDC, 2007; Lockary et al., 2007; Manning et al., 2007); in the United States as a whole, it is estimated that non-O157 STEC represent 64% of domestically acquired STEC infections (Scallan et al., 2011).
Because of the large and geographically diverse area included in this analysis and the large sample size provided by the inclusion of 11 years of surveillance data in all 10 FoodNet sites, we were able to extend previous findings, and provide some new insights regarding epidemiologic features of non-O157 STEC. Our study had sufficient power to provide a more definitive analysis by non-O157 STEC serogroup; other studies did not have enough cases to do so. About 20% of the cases in our analysis were included in smaller, state-specific analyses (Hedican et al., 2009; Lathrop et al., 2009; Hadler et al., 2011).
Persons with non-O157 STEC infection were nearly five times more likely than persons with O157 STEC infection to report recent international travel and three serogroups, O111, O103, and O26 were frequently travel-associated, particularly to Mexico or Central America. Other, smaller, studies have described similar patterns (Hedican et al., 2009; Lathrop et al., 2009; Hadler et al., 2011). Little is known about the prevalence of these serogroups in Central and South America, although all three have been isolated from humans and cattle in Chile and Argentina (Cordovez et al., 1992; Mercado et al., 2004; Rivas et al., 2006), and non-O157 STEC have been isolated from street-vended food in Mexico (Lopez-Saucedo et al., 2010). Our finding that non-O157 STEC were more commonly reported among persons of Hispanic ethnicity may be explained by the large number of reported infections from New Mexico, the FoodNet site with the largest Hispanic population (U.S. Census Bureau, 2011).
During the time period analyzed, testing of patients with diarrhea for non-O157 STEC was much less routine than testing for O157 STEC, and many fewer infections were recognized. It is likely that under-recognition of non-O157 STEC illnesses is a major reason that the ones that are recognized were less likely to be associated with outbreaks than O157 STEC infections.
Because FoodNet surveillance includes areas in only 10 states and the surveillance population included only 15% of the U.S. population, cases captured by this system may not be representative of all cases of non-O157 STEC infection in the United States (Scallan, 2007). Additionally, the laboratories that test for non-O157 STEC in states with FoodNet sites might not be representative of all of the laboratories serving FoodNet sites. Whether a person with STEC infection is actually tested properly could be influenced by demographic characteristics (e.g., children may be more likely to be tested), or the type of health care accessed (e.g., in another analysis, reference laboratories were less likely than others to test all stool specimens routinely for STEC [Hoefer et al., 2010]); data on the types of tests that were performed on each specimen were not collected systematically during this time period. FoodNet does not collect information on the virulence factors or stx-subtypes associated with each infection; this information would be useful to further characterize traits associated with severe infections.
The current FoodNet case definition relies on culture-confirmation of an infection to be reported. Because not all stools that yield Shiga toxin in broth culture are further cultured on selective media for STEC or forwarded to state laboratories for further testing, it is likely that our findings underestimate the true number of non-O157 STEC infections. We could not evaluate the proportion of toxin-positive stools not submitted for culture or not yielding an isolate at the state public health laboratory because FoodNet personnel did not systematically collect this information before 2012.
The non-O157 STEC are a heterogeneous group; different serogroups vary in their association with certain exposures (i.e., travel), with outbreaks, and with severe illness. More information on the most important routes of transmission for non-O157 STEC is needed. The ability to detect non-O157 STEC infections is dependent on clinical laboratories performing Shiga toxin testing and expeditiously sending positive broths to public health laboratories for isolation and characterization of STEC. To diagnose STEC infections, all stools submitted for diagnosis of acute community-acquired diarrhea should be simultaneously cultured for O157 STEC on selective and differential agar and assayed for non-O157 STEC with a test that detects the Shiga toxins (Gould et al., 2009). Clinical laboratories should promptly report positive findings of STEC to the physician and to public health authorities and follow guidance so that strains are appropriately serotyped and subtyped (Gould et al., 2009).
Footnotes
Acknowledgments
We thank the Emerging Infections Program surveillance officers and the participating local and state health departments and laboratories. Mike Hoekstra provided valuable input on the statistical analyses. Funding for this report was provided by the Centers for Disease Control and Prevention, the United States Department of Agriculture, and the United States Food and Drug Administration.
Disclosure Statement
No competing financial interests exist.