
Abstract
Listeria monocytogenes is an important foodborne pathogen of public health concern. A total of 902 retail food samples, including 342 ready-to-eat (RTE) foods, 366 infant foods, and 194 raw chickens were collected randomly in supermarkets and farmers' markets in 12 geographic areas in Shaanxi Province, China and screened for L. monocytogenes. All L. monocytogenes isolates were characterized by antimicrobial susceptibility testing, serotyping, and pulsed-field gel electrophoresis (PFGE). Twenty-seven (3.0%) samples were positive for L. monocytogenes, and 39 L. monocytogenes isolates were recovered from positive samples. Of these L. monocytogenes isolates, 21 isolates (53.8%) showed resistance to at least one antimicrobial. The isolates displayed resistance most frequently to oxacillin (18 isolates, 46.2%), followed by tetracycline (five isolates, 12.8%), erythromycin (four isolates, 10.3%), trimethoprim/sulfamethoxazole (three isolates, 7.7%), chloramphenicol (two isolates, 5.1%), and vancomycin (one isolate, 2.6%). All isolates were sensitive or displayed intermediate resistance to gentamicin, ampicillin, ciprofloxacin, and amikacin. Four serotypes including serotype 1/2b, 4b, 4e, and 1/2a were identified in those foodborne isolates. PFGE analysis demonstrated that some isolates with the same PFGE patterns came from different food sources, and isolates from the same food source tend to cluster closely. Presence of L. monocytogenes of clinically important serotypes in retail foods and their antimicrobial resistance constitute a potential risk for the public. Appropriate measures should be taken by government, industry, and consumers to reduce the risk posed by this ubiquitous pathogen.
Introduction
L
Because of its facultatively intracellular nature, it is difficult to treat listeriosis. Currently, the standard therapy for listeriosis is on the basis of conjoint use of ampicillin and gentamicin, while trimethoprim–sulfamethoxazole is the common antibiotic used for treatment of bacteremia and listeriosis (Hof, 2004). In addition, rifampin, erythromycin, vancomycin, linezolid, and carbapenems have been recommended to treat listeriosis (Hof, 2004; Janakiraman, 2008). Although L. monocytogenes, unlike other foodborne pathogens, rarely develops acquired resistance to antibiotics, multidrug-resistant L. monocytogenes isolates have been reported from food, animals, and humans (Zhang et al., 2007; Morvan et al., 2010; Bundrant et al., 2011). The resistance levels of L. monocytogenes could be affected by the antimicrobials used in humans and animals, and showed geographical and seasonal (Chen et al., 2009) differences. Moreover, resistance genes located on plasmid can be horizontally transmitted to Listeria spp from enterococci through conjugation (de Niederhausern et al., 2004).
Currently, at least 13 serotypes have been identified in L. monocytogenes. Considering their association with epidemic listeriosis, L. monocytogenes could be grouped into four evolutionary genetic lineages (I, II, III, and IV). Lineage I, including serotypes 1/2b, 3b, 4b, 4d, 4e and 7, is found to be overrepresented among human clinical isolates and epidemic outbreaks in most studies, while lineage II including serotypes 1/2a, 1/2c, 3a, and 3c, is typically sporadically isolated from both humans and animals. Lineage III and IV, including serotypes 4a and 4c, are rare and predominantly identified in animals (Liu et al., 2006; Bundrant et al., 2011). Of these 13 serotypes, more than 90% of human listeriosis cases are caused by strains belonging to serotypes 1/2a, 1/2b, and 4b, and most strains associated with listeriosis outbreaks belong to serotype 4b (Roberts et al., 2009).
Although L. monocytogenes exists at a generally low incidence in foods in many countries, it has a relatively high mortality rate and this property make it a notorious foodborne pathogen that is under routine surveillance. In China, due to insufficient attention paid to Listeria contamination and lack of ability of isolation and identification in local laboratories, there is still limited information available on L. monocytogenes in food. The aims of this study were to (1) evaluate the occurrence of L. monocytogenes in retail foods in China; (2) investigate the antimicrobial susceptibility of L. monocytogenes isolates to 10 antimicrobials commonly used in the treatment of listeriosis; and (3) determine the genetical relatedness of L. monocytogenes isolates from different food sources.
Materials and Methods
Sample collection and isolation of L. monocytogenes isolates
From July to December 2010, a total of 902 retail food samples were collected randomly from supermarkets and farmers' markets in 12 geographic areas in Shaanxi Province, China including 342 RTE foods including salad, frozen dumpling, salt peanuts, dried tofu, and fried chicken and fish, 366 infant foods including powdered infant formula and infant rice cereal, and 194 raw whole chicken. Isolation of L. monocytogenes was performed as described in GB 4789.30-2010 (National Standard of the People's Republic of China, 2010). Briefly, 25 g of each food sample was mixed and homogenized with 225 mL buffered peptone water (Beijing Land Bridge Technology Ltd., Beijing, China). For whole chicken, the carcass rinse was obtained. The mixture or rinse was incubated at 37°C with shaking at 150 rpm for 18–24 h. After pre-enrichment, a 3-mL aliquot was transferred to 30 mL Listeria enrichment broth LB1 (Beijing Land Bridge Technology Ltd., tryptone 0.5%, multivalent peptone 0.5%, yeast extract paste 0.5%, sodium chloride 2%, potassium dihydrogen phosphate 0.14%, dibasic sodium phosphate 1.2%, esculin 0.1%, nalidixic acid 0.0022%, acridine yellow 0.0013%) and then incubated at 30°C with shaking 150 rpm for 18–24 h. Then a 0.1-mL culture was transferred to 10 mL Listeria enrichment broth LB2 (Beijing Land Bridge Technology Ltd., nalidixic acid 0.002%, acridine yellow 0.0025%, other components were same as LB1). After incubation at 30°C for 18–24 h, a loopful of the culture was streaked onto CHROMagar plates (Beijing Land Bridge Technology Ltd.). Following incubation at 37°C for 24–48 h, one or two presumptive colonies (blue center, surrounding by white haloing) per sample were transferred to trypticase soy agar (Beijing Land Bridge Technology Ltd.) with 0.6% yeast extract and incubated at 37°C for 24 h, and were confirmed by polymerase chain reaction (PCR) detection of hly and iap genes (Kim et al., 2007; Park et al., 2006). L. monocytogenes CMCC54004 from National Center for Medical Culture Collections in China was included as a positive control strain for PCR. The confirmed isolates were stored at −80°C in trypticase soy broth plus 25% (vol/vol) glycerol until further analysis.
Serotyping and antimicrobial susceptibility testing
All of the confirmed isolates were serotyped with a commercial serotyping kit (Denka Seiken Co., Tokyo, Japan) according to the manufacturer's instructions. Antimicrobial susceptibility test was performed by the agar dilution method on Mueller-Hinton agar (Beijing Land Bridge Technology Ltd.) plate containing 5% lysed horse blood (CLSI, 2010). The antibiotic agents tested included oxacillin, vancomycin, tetracycline, gentamicin, trimethoprim/sulfamethoxazole, ampicillin, chloramphenicol, ciprofloxacin, amikacin, and erythromycin. Escherichia coli ATCC 25922 and Enterococcus faecalis ATCC 29212 were used as quality control strains in each run. For all antibiotics except ampicillin, the breakpoints used for staphylococcus (CLSI, 2010) were adopted in this study for L. monocytogenes. For ampicillin, the breakpoint was taken from another study (Li et al., 2007).
Pulsed-field gel electrophoresis (PFGE)
PFGE using ApaI was performed to determine genomic DNA fingerprinting patterns of all L. monocytogenes isolates as previously described (Graves and Swaminathan, 2001). Briefly, 200 μL of cell suspension and 10 μL of 10 mg/mL lysozyme solution (Sigma) were mixed and incubated at 55°C for 20 min, and then 10 μL of 20 mg/mL proteinase K (Sigma) was added before plug preparation. The plugs were cut and were incubated in cell lysis buffer in a 55°C shaker water bath for 15–19 h with constant and vigorous agitation (150–175 rpm). Agarose-embedded DNA was digested with 25 U of ApaI (Takara, Dalian, China) at 25°C for 10 h. DNA fragments were separated by electrophoresis in 0.5×tris-borate-EDTA buffer at 14°C for 22 h on a CHEF-IIIMapper electrophoresis system using a pulse time of 4–40 s. The gels were stained with ethidium bromide and images were taken under ultraviolet transillumination. PFGE results were analyzed by the BioNumerics software (Applied-Maths, Kortrijk, Belgium), and banding patterns were compared by using Dice coefficients with a 1.5% band position tolerance. Genomic DNA of Salmonella serotype Branderup strain H9812 digested with XbaI was used as a molecular marker.
Results
Prevalence of L. monocytogenes
Among 902 samples, 27 (3%) were positive for L. monocytogenes, including 9 (2.6%) of the 342 RTE food samples, 7 (1.9%) of the 366 infant food samples, and 11 (5.7%) of the 194 raw whole chicken samples. A total of 39 L. monocytogenes isolates were recovered from the 27 L. monocytogenes positive samples (one to two isolates per sample) including 11 isolates from RTE food, 12 isolates from infant foods, and 16 isolates from raw whole chicken (Table 1).
One to two Listeria monocytogenes isolates were collected from each positive sample.
RTE, ready-to-eat.
Serotyping
Four different serotypes were identified among 39 L. monocytogenes isolates (Table 2). The majority of the isolates belonged to 1/2b (23 isolates, 59.0%), followed by 4b (8 isolates, 20.5%), 4e (7 isolates, 17.9%), and 1/2a (1 isolate, 2.6%). Serotype 1/2b was most frequently detected in RTE foods (9 isolates, 81.8%) and raw whole chicken (14 isolates, 87.5%). Serotypes 4e and 4b each were detected in 50% of isolates from infant foods. With regard to genetic lineage, lineage I-related isolates (1/2b, 4e, and 4b) were dominant (38 isolates, 97.4%). The remaining one isolate (1/2a) in raw whole chicken belonged to lineage II. None of the isolates fell into lineage III and lineage IV.
RTE, ready-to-eat.
Antimicrobial susceptibility testing
The 39 L. monocytogenes isolates displayed resistance most frequently to oxacillin (18 isolates, 46.2%), followed by tetracycline (5 isolates, 12.8%), erythromycin (4 isolates, 10.3%), trimethoprim/ sulfamethoxazole (3 isolates, 7.7%), chloramphenicol (2 isolates, 5.1%), and vancomycin (1 isolate, 2.6%) (Table 3). All isolates were sensitive to gentamicin, ampicillin, ciprofloxacin, and amikacin. Of all L. monocytogenes isolates, 21 isolates (53.8%) exhibited resistance to at least one antimicrobial (Fig. 1). Twelve isolates were resistant to one antimicrobial, eight to two antimicrobials, and one isolate was resistant to seven antimicrobial agents (Fig. 1).
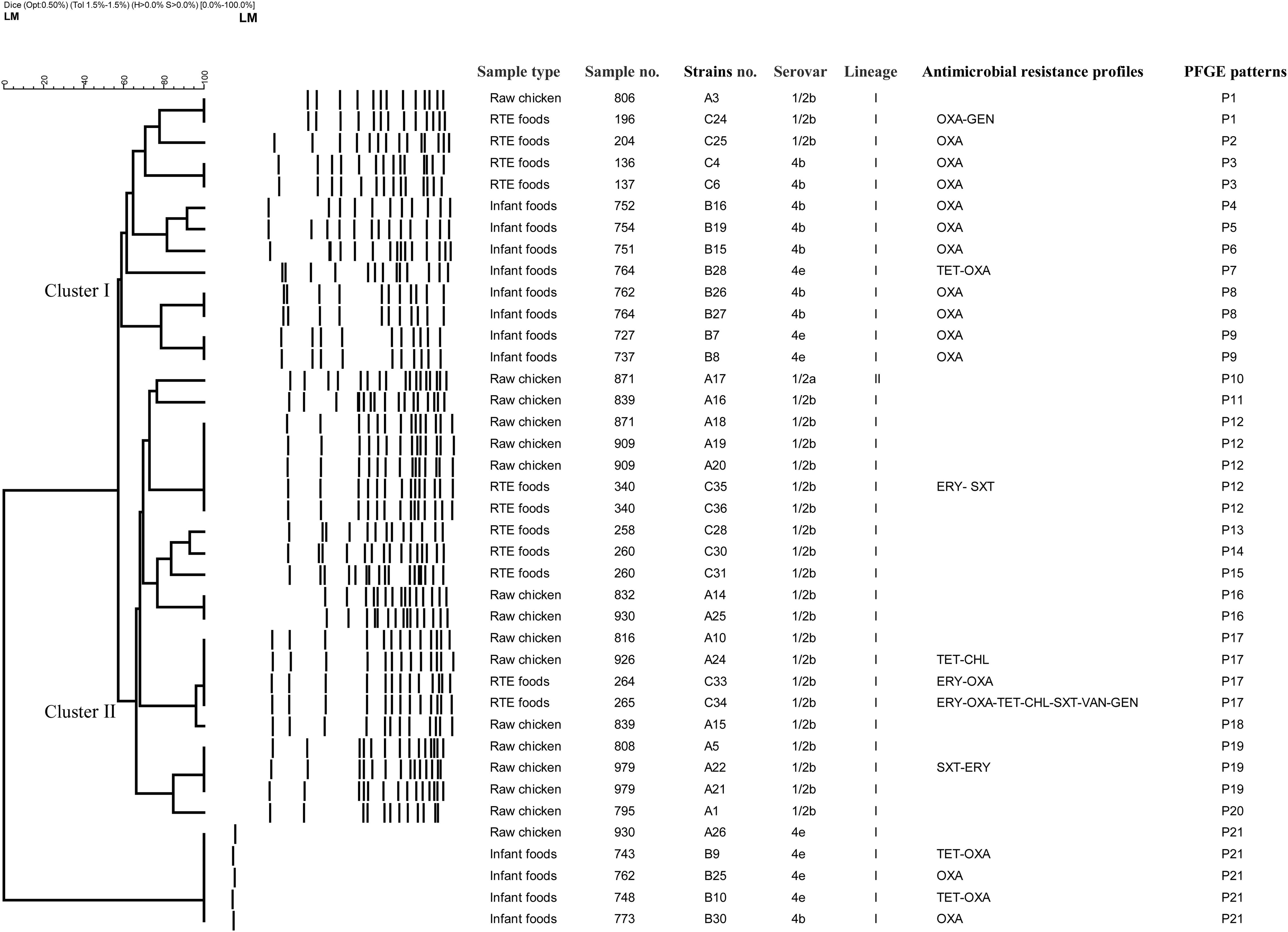
Dendrogram of pulsed-field gel electrophoresis (PFGE) patterns showing the genetic relatedness of 39 Listeria monocytogenes strains. The source, strain name, serogroup, antibiotic resistance pattern, and PFGE pattern of the strains are shown in the right side. OXA, oxacillin; GEN, gentamicin; TET, tetracycline; ERY, erythromycin; SXT, trimethoprim–sulfamethoxazole; CHL, chloramphenicol; VAN, vancomycin. RTE, ready-to-eat.
RTE, ready-to-eat; R, resistant isolates; ERY, erythromycin; OXA, oxacillin; TET, tetracycline; CHL, chloramphenicol; SXT, trimethoprim–sulfamethoxazole; AMP, ampicillin; GEN, gentamicin; CIP, ciprofloxacin; AMI, amikacin; VAN, vancomycin.
PFGE
All of the L. monocytogenes isolates were analyzed for genetic relatedness using PFGE with ApaI. Except for five isolates that were not typeable using the enzyme chosen, the remaining 34 isolates were categorized into two clusters based on 57% similarity and 20 PFGE patterns (Fig. 1). Cluster I included all isolates of serotypes 4b and 4e recovered from RTE food and infant food, and three isolates of serotype 1/2b. In cluster II, all except one isolate belonged to serotype 1/2b. The most frequent PFGE patterns (P) was P12 (14.7%, 5/34), followed by P17 (11.8%, 4/34) and P19 (8.8%, 3/34). Five other PFGE patterns containing isolates sharing 100% homology were P1, P3, P8, P9, and P16 (each containing two isolates). Some isolates with identical PFGE patterns came from different sources (Fig. 1). All the isolates with identical PFGE patterns belonged to the same serotype, but some of them showed different antimicrobial resistance profiles (Fig. 1).
Discussion
In this study, the prevalence of L. monocytogenes in different food items sold in Shaanxi Province in China was determined and the isolates were characterized for serotype, antimicrobial resistance, and genetic relatedness. The overall prevalence of L. monocytogenes in RTE food samples is 2.6%, which was similar to previous reports in other countries (Little et al., 2007; Sant'Ana et al., 2012). It is suggested that the RTE food should be heated for a while before consuming to reduce the chance of getting infected by L. monocytogenes. The positive rate for infant food samples was 1.9%, which was higher than other reports in China (Chen et al., 2003; Huang et al., 2005). As L. monocytogenes could lead to severe infections in infants, the existence of the pathogen in infant food products constitutes a potential risk for infants' health. The prevalence of L. monocytogenes in raw whole chicken samples was 5.7%, which was much lower than another report (37.0%) for chicken in Japan (Inoue et al., 2000). Varied contamination rate in different retail foods and in different geographic locations may be due to the differences in livestock management, processing, sampling strategy, isolation methods, and so on (Hansen et al., 2006).
In terms of susceptibility to 10 antibiotics, 53.8% of the isolates exhibited resistance to at least one antibiotic, which was much higher than other reports (Miranda et al., 2008; Morvan et al., 2010; Korsak et al., 2012; Wieczorek et al., 2012). For example, 0.42% of L. monocytogenes from food and food-related sources in Poland were resistant, and 1.27% of isolates from human listeriosis cases in France showed phenotypic resistance. In addition, nine isolates (23.1%) showed multidrug resistance (two or more kinds of antibiotics). The high prevalence of oxacillin resistance among L. monocytogenes isolates (46.2%) in this study was consistent with previous studies (Troxler et al., 2000; Li et al., 2007), which has been related to the absence of specific penicillin-binding proteins in the Listeria cytoplasmic membrane (Heger et al., 1997). In addition to oxacillin, the resistance to tetracycline (12.8%), erythromycin (10.3%), and trimethoprim/sulfamethoxazole (7.7%) was much higher than other antibiotics. There was strong evidence that the imprudent use of antibiotics in agriculture and stock farming may lead to the antibiotic resistance transfer from food commensals to human residential bacteria via horizontal gene transfer (Wang et al., 2006). An important finding necessitating attention was that one isolate from RTE food demonstrated resistance to vancomycin. Resistance to vancomycin has been rarely reported among L. monocytogenes isolates from various foods (Yang et al., 2008; Conter et al., 2009; Ruiz-Bolivar et al., 2011; Korsak et al., 2012). Since vancomycin has represented the cornerstone of treatment of infections caused by Gram-positive bacteria, and many listerial infections are caused by consumption of contaminated foods, the presence of vancomycin-resistant L. monocytogenes in RET foods is of great concern. The vancomycin-resistance determinants of Listeria may be transferred from other bacteria such as enterococci, and conjugation studies indicated that transposons and plasmids are responsible for the emergence of resistance to antimicrobials such as vancomycin in Listeria (Conter et al., 2009). All isolates in this study were sensitive to gentamicin, ampicillin, ciprofloxacin, and amikacin, which was in agreement with other reports (Heger et al., 1997; Korsak et al., 2012). These data on antimicrobial resistance profile are of importance for clinicians to choose effective agents to treat problematic and sometimes fatal listerial infections.
In this study, all L. monocytogenes belonged to lineages I and II, which was in agreement with previous studies in the United States, Japan, Poland, China, and many European countries (Kathariou, 2002; Parihar et al., 2008; Yang et al., 2008). L. monocytogenes isolates belonging to 1/2b (59.0%) were most frequently detected. This was consistent with another study in the United States (Chen et al., 2010). In contrast, several studies (Chen et al., 2009; Yan et al., 2010) in other parts of China reported that serotype 1/2a was predominant in food products. The high prevalence of isolates of serotypes 1/2b and 4b may pose a public health threat since these serotypes were associated with human listeriosis cases, and isolates of serotype 4b were commonly implicated in outbreaks (Roberts et al., 2009).
Some isolates with identical PFGE patterns were recovered from different food samples, which indicates that cross contamination may occur among the retail foods during production, transportation, or in the market. Isolates with the same PFGE pattern may exhibit the same antimicrobial resistance profiles (such as isolates in P3) or different antimicrobial resistance profiles (such as isolates in P17). Our findings indicate that PFGE patterns did not correlate with antimicrobial resistance profiles, which was in agreement with Zhang et al. (2007). All isolates with the same PFGE patterns exhibited the same serotypes, which contrasts with Yan et al. (2010), who reported that isolates with the same PFGE patterns exhibited the same or different serotypes.
In summary, L. monocytogenes existed at a relatively low rate in retail foods in Shaanxi Province in China, but the risk it posed for human health could not be underestimated, especially when they are present in RTE foods and infant foods. Moreover, most of the isolates belonged to the serotypes (1/2a, 1/2b, and 4b) frequently associated with disease, and some demonstrated resistance to commonly used antibiotics in treating listeriosis. PFGE indicates that L. monocytogenes from different sources are genetically diverse and cross-contamination may occur. Appropriate measures should be taken by industry, retailers, and consumers to reduce the risk of L. monocytogenes infection. For example, hazard analysis and critical control point programs should be implemented in plants to lower contamination during processing. Preventing cross-contamination, keeping good personal hygiene, and storing RTE food in a refrigerator are effective measures to reduce the risk of listeriosis taken by retailers and consumers.
Footnotes
Acknowledgment
This research was supported in part by the Fundamental Research Funds for the Central Universities (No. QN2011139) and National Natural Science Foundation of China (No. 31101347).
Disclosure Statement
No competing financial interests exist.