
Abstract
Objective:
This was a systematic review and meta-analysis to determine the proportion of Escherichia coli O157 cases that develop chronic sequelae.
Data Sources:
We conducted a systematic review of articles published prior to July 2011 in Pubmed, Agricola, CabDirect, or Food Safety and Technology Abstracts.
Study Selection:
Studies were selected that reported the number of E. coli O157 cases that developed reactive arthritis (ReA), hemolytic uremic syndrome (HUS), irritable bowel syndrome, inflammatory bowel disease, or Guillain Barré syndrome.
Methods:
Three levels of screening and data extraction of articles were conducted using predefined data fields. Meta-analysis was performed on unique outcome measures using a random-effects model, and heterogeneity was assessed using the I2 value. Meta-regression was used to explore the influence of nine study-level variables on heterogeneity.
Results:
A total of 82 studies were identified reporting 141 different outcome measures; 81 reported on HUS and one reported on ReA. Depending on the number of cases of E. coli O157, the estimate for the proportion of E. coli O157 cases that develop HUS ranged from 17.2% in extra-small studies (<50 cases) to 4.2% in extra-large studies (>1000 cases). Heterogeneity was significantly associated with group size (p<0.0001); however, the majority of the heterogeneity was unexplained.
Conclusions:
High unexplained heterogeneity indicated that the study-level factors examined had a minimal influence on the variation of estimates reported.
Introduction
E
The World Health Organization introduced the Global Burden of Disease effort to expand disease burden estimates beyond mortality rates. Diarrheal disease is estimated to be the fifth leading cause of morbidity worldwide, causing an estimated 2.2 million deaths per year (World Health Organization, 2008). As diarrheal disease can be caused by many pathogens, the exact number of cases attributed to E. coli O157 is uncertain. An increased understanding of disease progression and the sequelae associated with E. coli O157 infection could assist efforts to develop more accurate burden of disease (BOD) estimates for E. coli O157.
Understanding the true BOD is an important aspect of evidence-informed decision making and can help guide policy related to foodborne disease prevention, interventions, and cost estimates. However, the accuracy of current BOD estimates is limited by minimal knowledge of the long-term health effects. Development of measures such as Disability Adjusted Life Years (World Health Organization, 2008) and Health Adjusted Life Years (Public Health Agency of Canada, 2005) have attempted to incorporate the long-term health effects of an illness into disease burden estimates. Although the association between E. coli O157 infection and HUS is accepted (Karmali et al., 1985; Palermo et al., 2009; Zoja et al., 2010; Melton-Chelsa et al., 2012), the frequency of cases that go on to develop HUS and other potential chronic sequelae is less well known.
Systematic review is an established way to identify and summarize the body of literature associated with a subject area in a transparent, reproducible manner (Liberati et al., 2009; Higgins and Green, 2011). Meta-analysis (the formal statistical pooling of results from multiple studies) allows for the development of summary estimates, which can be used to inform BOD estimates. Meta-regression can be used to explore variables that may influence the range in reported outcomes (Higgins and Green, 2011). This review was conducted as part of a broader literature search, which also investigated the proportion of cases of Salmonella and Campylobacter that develop chronic sequelae. The purpose of this systematic review and meta-analysis was to estimate the proportion of cases of E. coli O157 that develop HUS, IBS, IBD, ReA, or GBS and to explore which variables contribute to differences between studies.
Materials and Methods
Literature search
A keyword search was performed between July 19 and July 25, 2011 using Pubmed, Agricola, CabDirect, and Food Safety and Technology Abstracts to identify information on E. coli O157, Salmonella, and Campylobacter. The search terms were constructed iteratively by exploring the addition of new search terms. No limitations on date, country of publication, or language were used. Studies specific to E. coli O157 were identified at the final stages of data extraction and are included in this review. The search strategy included any combination of the terms (‘Escherichia coli O157,’ or, ‘O157,’ ‘VTEC,’ ‘STEC,’ ‘O157:H7’ or Salmonella or Campylobacter) and (‘sequel*,’ ‘long-term,’ ‘long term,’ ‘chronic,’ ‘Guillain*,’ ‘HUS,’ ‘hemolytic uremic syndrome,’ ‘haemolytic uraemic syndrome,’ ‘hemorrhagic uremic syndrome,’ ‘haemorrhagic uraemic syndrome,’ ‘Reiter*,’ ‘complication*,’ ‘arthritis,' ‘irritable bowel syndrome,’ ‘IBS,’ ‘post infectious irritable bowel syndrome,’ or ‘inflammatory bowel disease’). Additional references were located through a search of the reference lists of all studies that met the inclusion criteria. All references were imported into RefWorks Reference Management Software (ProQuest LLP, 2012), where duplication removal occurred using the exact and close match functions.
Inclusion and exclusion criteria for systematic review
Three levels of screening were performed (for details, see Supplementary Data S1; Supplementary Data are available online at
Data collection process
Relevance screening and data extraction were conducted using a standardized form created in Microsoft Excel (Version 2007) (available from the authors upon request). Training for the first level of screening was performed using 200 test articles that were assigned to each reviewer. Consensus of >95% was achieved between reviewers for the test articles. Due to the high agreement and resource constraints, each article was subsequently reviewed by a single reviewer.
The second level of screening was performed independently by two reviewers per reference. Inclusion/exclusion results for the articles were compared and conflicts were resolved via consensus, with included references moving on to the third level of screening.
The third level of screening was performed by four different reviewers, with two reviewers independently reviewing each article. The screening questions and data extraction tool were refined through a pilot test of 50 articles. Once refined, data were extracted using the data extraction tool described in the following section. Conflicts were resolved via consensus; any remaining disagreements were resolved by a third reviewer.
Data variables
Information on population (dates for data collection, country, age range, and gender distribution of E. coli O157 cases), disease status (related to the sequelae) prior to illness with E. coli O157, season of data collection, outbreak source (where applicable), study directionality (retrospective versus prospective), source of data (surveillance versus outbreak versus hospitalized cases of E. coli O157), categories describing E. coli O157 diagnosis and sequelae diagnosis, the length of time between E. coli O157 infection and sequelae diagnosis (follow-up time) and outcomes (number of participants with E. coli O157, number of participants who developed chronic sequelae) was extracted. Categorization of season, outbreak source, data source, study design, pathogen diagnosis, and sequelae diagnosis was performed after data extraction for inclusion in the meta-regression. In the northern hemisphere, seasons were classified as fall (September–November), winter (December–February), spring (March–May), and summer (June–August). In the southern hemisphere they were classified as fall (March–May), winter (June–August), spring (September–November), and summer (December–February). Outbreak source was classified as food, water, animal contact, day care, nursing home, or other. Data source was classified as surveillance (which included laboratory and notifiable disease registries, sporadic cases, and other population surveillance), associated with an outbreak or as hospitalized cases of E. coli O157. Study directionality was classified as prospective (cases of E. coli O157 were identified and the assessment for sequela occurred in the future), retrospective (both identification as a case of E. coli O157 and sequelae diagnosis had already occurred when data collection for the study was initiated), or other (for hospitalized cases where directionality could not be determined). Pathogen diagnosis was classified as confirmed (through culture, serology, or DNA based tests), probable (based on case definition from study or associated with an outbreak), or other (which included studies where cases of HUS were included in the case definition for E. coli O157). Sequelae diagnosis was categorized as taken from medical records/diagnosed by physician, other (which included self-reported questionnaires, or studies that reported multiple outcomes using a variety of definitions for HUS), or not reported. For studies that identified both full and partial cases (met some but not all criteria used to assess HUS) of HUS, only full cases were included as an outcome measure for the analysis.
As some studies reported multiple methods of diagnosis for both the sequelae (e.g., both medically diagnosed and self-reported cases) and E. coli O157 (e.g., both probable and culture-confirmed cases) as well as multiple data sources (e.g., both outbreak associated and hospitalized cases), each combination of E. coli O157 and sequelae diagnosis was considered a separate outcome measure. As it was possible to create multiple estimates from the same study for the proportion of cases of E. coli O157 that developed sequelae, the term “outcome measure” was used to describe these unique proportion estimates.
Assessment of reporting of factors related to internal and external validity
Information on reporting of factors related to internal validity (risk of bias) and external validity (generalizability) were extracted to allow for further exploration. Ten criteria were extracted. Factors related to internal validity were study directionality, the source of data, method of diagnosis for both the pathogen and sequelae, follow-up time, and reporting the specific criteria used for the sequelae diagnosis. The definitions for sequelae diagnosis were divided into two categories: the method of diagnosis (physician versus self-reported versus other) and whether specific diagnostic criteria were provided (e.g., a description of the laboratory criteria used in diagnosis of HUS). Factors related to external validity were reporting of relevant population information (country, gender distribution, and age range of E. coli O157 cases).
Statistical analysis
The primary outcome was the proportion of people with E. coli O157 who developed a specific chronic sequela. This was calculated as the number of persons developing a sequela divided by the total number of cases of E. coli O157. Standard errors and confidence intervals for a single proportion were derived. Prior to analysis adjusted proportions were calculated using a logit transformation (Sanchez et al., 2007).
All statistical analyses were performed in Stata Version 12 (Statacorp 2012). Meta-analysis for each sequela was performed using a random-effects model and the DerSimonian and Laird method to derive the summary estimate (Egger et al., 2001). Heterogeneity was assessed using the I2 value, where values closer to 100% indicate that heterogeneity is due to actual differences between studies and values closer to 0% indicate that heterogeneity is due to chance (Higgins and Thompson, 2002). For studies reporting on the same populations (for example, multiple reports from the same outbreak using the same outcome measure), the publication that provided the most complete ancillary information was included. A count of 0.5 was added (to those reporting 0%) or subtracted (from those reporting 100%) to allow for inclusion in the meta-analysis (Borenstein et al., 2007). Meta-regression was used to explore sources of heterogeneity if the I2 value was higher than 25% and if >10 outcome measures were available. The source of data, method of pathogen diagnoses, age group, country (England and Wales were combined into a single category), decade of data collection, season, outbreak source, group size, and whether the design was retrospective or prospective were factors considered. Meta-regression was performed using logit transformed outcomes and logit transformed within-study standard errors, and factors were only included if there was variation in the factor among studies. Significance tests were performed using univariable analysis where those presenting a p-value≤0.05 were considered significant. Significant variables were then entered into a backwards multivariable model, and those that remained significant (p≤0.05) were explored with subgroup meta-analysis.
Categorical variables representing group size and age group were generated prior to meta-regression. For group size, the studies were classified based on the number of cases (extra small <50 cases, small=51–200 cases, medium=201–500 cases, large=501–1000 cases, and extra-large >1000 cases). Age group was classified as all ages, adults (≥18 years), or youth (<18 years). A separate category for children was generated to acknowledge and explore those studies that reported on children only (<10 years).
Results
Systematic review
Study selection
The results of the search are summarized in Figure 1. The screening process included three foodborne pathogens until the final step, which was specific to E. coli O157. After final screening of full text articles and evaluation of the reference lists of relevant studies, there were 82 studies containing relevant information on E. coli O157.
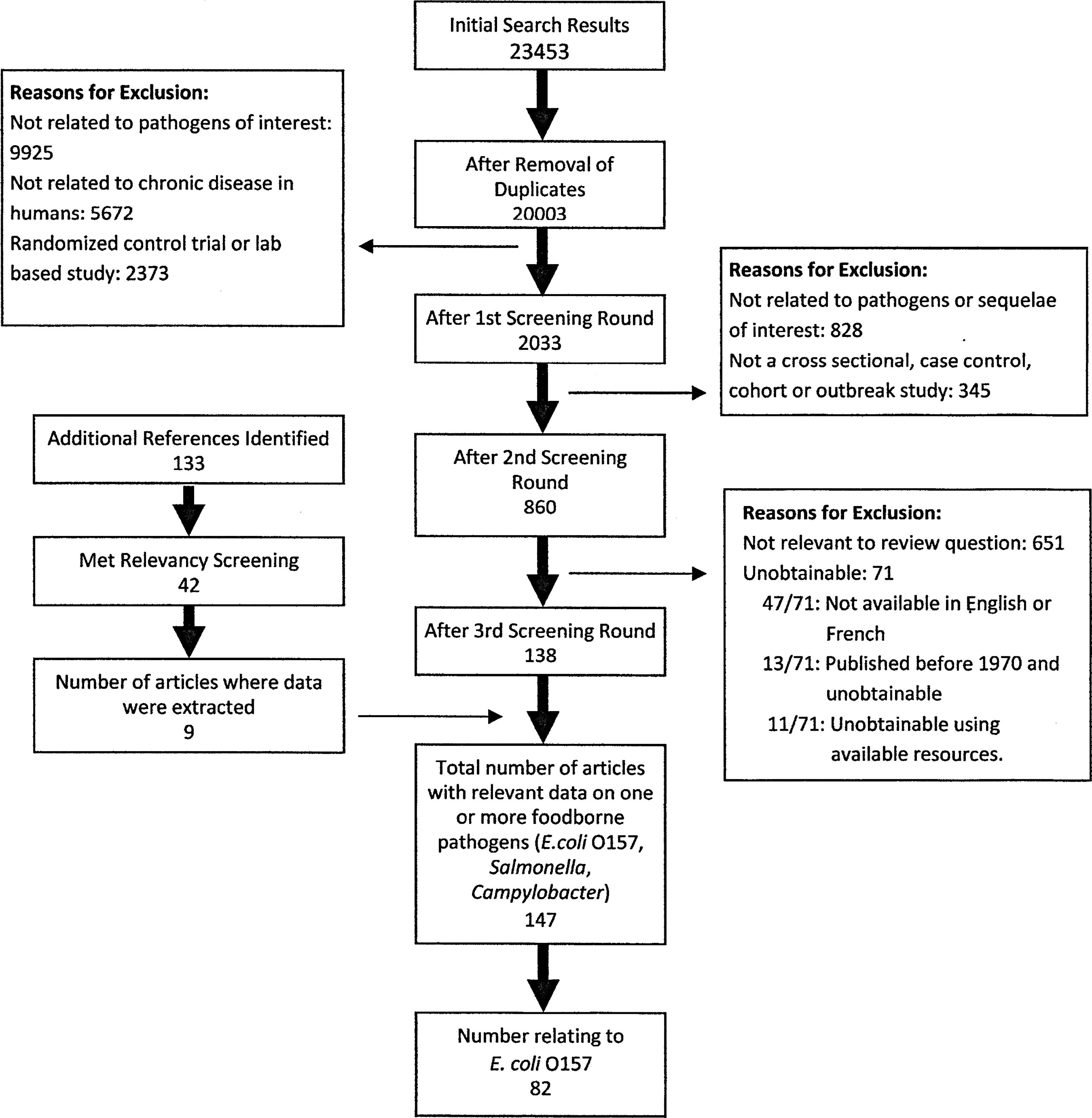
Results from the literature search for studies relating to chronic sequelae associated with Escherichia coli O157 published prior to July 2011.
Study descriptions
The 82 studies reported on 121 different populations from 18 different countries (Table 1). All but two studies were from North America (n=44), Europe (n=26) and Japan (n=10). Seventy-nine studies related to E. coli O157 and HUS, two evaluated E. coli O157 and HUS or thrombotic thrombocytopenic purpura (TTP), and one study investigated E. coli O157 and ReA. No studies on the other chronic sequelae were found.
Other denotes studies using hospitalized cases of E. coli O157 where it was not possible to determine directionality.
Surveillance included laboratory and notifiable disease registries, sporadic cases, and other population surveillance.
Indicates publications identified as duplicate populations, excluded from meta-analysis.
Other includes person to person transmission, environmental (non-water) contamination or unidentified source.
HUS, hemolytic uremic syndrome; NR, not reported; NA, not applicable; TTP, thrombotic thrombocytopenic purpura; ReA, reactive arthritis.
Of the 121 populations reported, 90 were based on outbreaks. Of those outbreak-based populations that reported seasonality, 63% (54/86) of outbreaks occurred in the spring and/or summer. Only 41% (37/90) of those reported the source of the outbreak, of which 57% (21/37) were foodborne. Of the remaining study designs (surveillance and hospital-based), 26 were based on population surveillance, of which 16 were prospective, six focused on hospitalized cases of E. coli O157, and a single study looked at sporadic cases in the community.
E. coli O157 and HUS
Outcome measures
There were 141 different outcome measures for the probability of developing HUS following E. coli O157 infection from the 120 different populations (Table 2 and Fig. 2). The proportion of cases of E. coli O157 was variable across studies, and estimates for development of HUS ranged from 0% to 100% (Fig. 2). In the outbreak studies, E. coli O157 case numbers ranged from 2 to 2311 persons. Of the population surveillance studies, E. coli O157 case numbers ranged from 25 to 3464 persons, and the hospitalized cases of E. coli O157 ranged in size from 2 to 2313 persons. For diagnosis of E. coli O157, 63% (90/141) reported “confirmed” cases of E. coli O157, with the proportion of cases that developed HUS ranging from 0% to 100%. Of the 39 outcomes reporting probable cases of E. coli O157, the probability of developing HUS ranged from 0% to 67%. There were 10 studies that assumed all cases of HUS were positive for E. coli O157 and therefore included them as a case (classified as “other” for pathogen diagnosis). In these studies, the number of cases developing HUS ranged from 1.8% to 50%.
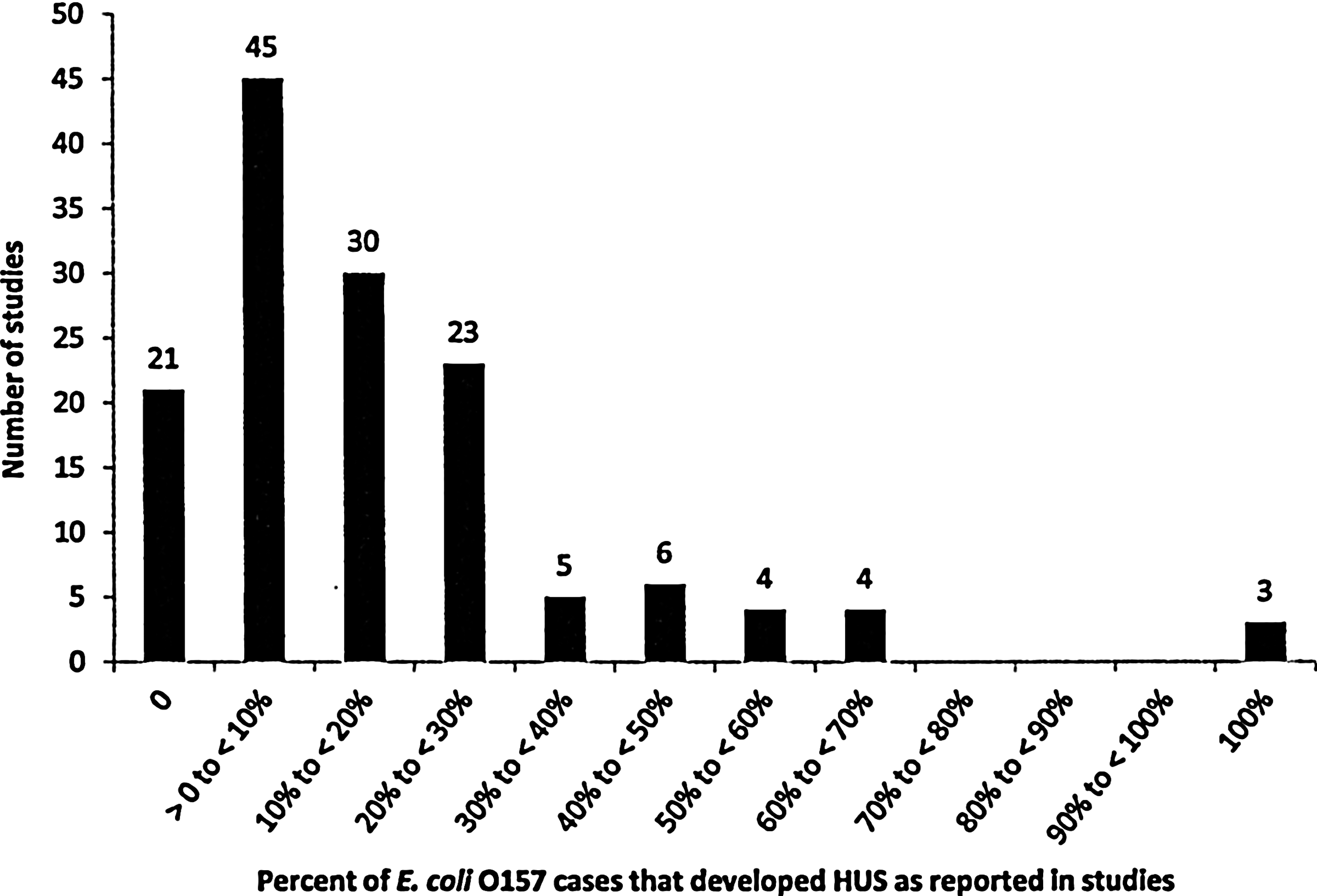
Distribution of outcome estimates of the proportion of Escherichia coli O157 cases that developed hemolytic uremic syndrome (HUS) from studies published prior to July 2011.
Pathogen diagnosis: Confirmed included those confirmed for E. coli O157 by culture, serology, or DNA-based tests. Probable included cases of E. coli O157 that met clinical case definition of study or were associated with an outbreak. Other included those where a case of HUS was considered positive for E. coli O157 in case definition.
Sequelae diagnosis: Medical records/physician included those hospitalized for sequelae or diagnosed by a physician.
Indicates publications identified as duplicate populations, excluded from meta-analysis.
HUS, hemolytic uremic syndrome; NR, not reported; TTP, thrombotic thrombocytopenic purpura; ReA, reactive arthritis.
Assessment of internal and external validity
Thirty percent (25/82) of studies reported the length of time between diagnosis as a case and assessment for HUS. No studies reported on sequelae status prior to the study. All studies reported study directionality and source of data. Two studies did not provide information on how the pathogen was diagnosed. Due to the severity associated with HUS symptoms, all sequelae were physician diagnosed. However, 37% (30/82) of the studies did not provide a definition for the diagnosis of HUS. For population variables, 26% (22/82) did not report age range, and 44% (36/82) did not report gender distribution. Country was specified for all populations.
Meta-analysis/meta-regression
Prior to analysis, duplicate reports from the same outbreak or reports that presented on a subset of the same data were identified as “duplicate populations.” Removal of information on duplicate populations resulted in the exclusion of nine studies, for a total of 131 outcome measures included in the meta-analysis. The overall estimate for the proportion of cases of E. coli O157 that developed HUS was 13.1% (95% confidence interval 10.1%–17.1%, I2=91.3%). Due to the large amount of heterogeneity, meta-regression was performed.
The influence of age group, country, season, outbreak source, decade of data collection, study directionality, source of data, pathogen diagnosis, and group size was explored using meta-regression. Individually, all variables except for group size (p<0.0001) and season (p=0.016) were nonsignificant. After multivariable analysis, only group size remained significant (p<0.0001). Subgroup analysis demonstrated large variability between summary estimates, with extra-small groups (<50 cases) having a higher proportion of cases developing HUS (17.2%) with less heterogeneity (I2=48.9%), and extra-large groups (>1000 cases) having a significantly lower proportion of cases developing HUS (4.2%) with extremely high heterogeneity (I2=94.8%) (Table 3).
CI, confidence interval.
E. coli O157 and ReA or TTP
In the single study on E. coli O157 and ReA, the number of culture-confirmed cases that developed reactive arthritis was 0.25%. For TTP, proportions were reported as 2% for culture-confirmed cases and 7% in probable cases.
Discussion
This study used the results of a systematic literature search and meta-analysis to provide an estimate for the proportion of cases of E. coli O157 that developed chronic sequelae. Although there is a large body of literature available on E. coli O157, information on chronic sequelae was primarily limited to those studies that investigated the relationship with HUS. Within this body of research, the proportion of E. coli O157 cases developing HUS varied greatly. The large variation between studies makes developing a single summary estimate for the proportion of cases of E. coli O157 that develop HUS difficult. Group size was the only characteristic that had a significant effect on heterogeneity. All but three of the 102 outbreak-related outcome measures presented less than 100 cases of E. coli O157. The high proportion of HUS estimated from these smaller groups is concerning, considering the high number of small outbreaks that were located during the search. Previous studies have indicated as many as 12% of HUS cases result in death or end-stage renal disease, and 25% of HUS cases develop long-term renal sequelae (Karmali, 2004). In contrast, for larger populations those proportions were significantly lower, which may have more implications in the development of BOD estimates for E. coli O157 as they could be more representative of the incidence of HUS at the population level. The biggest concern, however, with interpreting these estimates is the high heterogeneity in the data even after subgroup meta-analysis, as this indicates that the study-level variables considered in this review were potentially not as influential as other host, pathogen, and environmental factors.
Some potential explanations and areas for further investigation could be virulence differences between E. coli O157 strains, severity of acute illness in cases, dose of E. coli O157 received, immune status of cases prior to infection, and age range of HUS cases. Although an association between HUS and age is generally accepted (Karmali et al., 2010), age was not found to be a significant contributor to heterogeneity in this review. This may be a factor of categorization as opposed to a true lack of association. In this study, the population was categorized based on the age range for E. coli O157 cases, not HUS cases. For those categorized as “all ages,” the occurrence of HUS could have been limited to children; however, this was not captured by our approach due to data-reporting limitations in the primary studies. The difficulty with capturing the effects of the other potential sources of heterogeneity is that this level of detail was often not reported within the primary studies. In order for these areas to be addressed in future meta-analyses, more detailed descriptions of the characteristics of HUS cases and identification of the E. coli O157 strains should be reported.
In addition, the inter-relatedness among variables and lack of variation between studies could explain why no associations were found. Due to the nature and severity of HUS, all of the sequelae cases were considered “medically diagnosed,” follow-up time was not reported in most studies, and most of the publications were small-outbreak studies. Differences in the case definitions for HUS and for cases of E. coli O157 could also be potential factors explaining the large amount of unexplained heterogeneity between studies. Additionally, there were no consistent criteria used to identify “probable cases of E. coli O157” between studies, contributing to the difficulties in comparing results between studies. The potential for misclassification as a case of E. coli could bias the results and increase or decrease prevalence estimates, depending on whether the case definition used had a high number of false positives or false negatives. Although the exploration of confirmed versus probable cases in the meta-regression attempted to explore the effects of this issue, clear and consistent case definitions for both E. coli O157 and HUS should be implemented and reported in future studies to allow further exploration of potential sources of heterogeneity.
An important issue identified by this systematic review was the lack of data pertaining to all other potential chronic sequelae. There are a few explanations for why these relationships may not have been evaluated in the available literature. The timing between illness and the assessment for chronic sequelae was short, or not reported, in the majority of studies, which may prevent the detection of illnesses that take longer to develop (for example, HUS typically manifests with severe symptoms in days versus ReA or IBS, which can take months to develop.) Another potential reason is that the studies themselves did not consider sequelae other than HUS, so their development would not have been captured. Finally, there is the possibility that other sequelae do not occur after E. coli O157 infection. Whether this relationship exists or not was not possible to determine given the available data. Developing accurate BOD estimates for E. coli O157 is limited until a better understanding of all chronic sequelae is known.
A number of long-term studies have looked at the sequelae associated with the Walkerton Outbreak of E. coli O157 and Campylobacter in Ontario, Canada in 2000 (Garg et al., 2003, 2005, 2006a, b, 2008, 2008a, b). The outbreak included cases infected with either or both pathogens. Due to the scale of the outbreak, confirming pathogen diagnosis was not conducted throughout the outbreak. The case definition for these studies was based on symptoms and potential exposure (Garg et al., 2006b). Because of this, distinguishing between cases of E. coli O157 and Campylobacter was not possible. Although these studies provide valuable insight into the issue of sequelae development after infection, the inability to distinguish between E. coli O157 and Campylobacter cases prevented their inclusion in this review. As a comparison, however, there were 27 confirmed cases of HUS in the Walkerton Health Study (Garg et al., 2006b). Based on the 995 cases of confirmed gastrointestinal illnesses included in the study, the proportion from this study is estimated at approximately 2.71%, on the lower end of our estimate for an extra-large group. However, when considering laboratory-confirmed cases of E. coli O157 or Campylobacter (n=188), the proportion was 14.9%, well within the confidence interval estimated in this study for a small group.
There are some additional limitations to the available data. Although efforts were made to remove outcomes on duplicate populations from the meta-analysis, due to the minimal information provided on each outbreak included in the overview study by Ammon et al. (1997), there is the possibility that some of the populations were also included in other studies. In addition, there was variation in outcomes reported from the same outbreak as demonstrated in the studies from Japan regarding the Sakai School Outbreak. The studies on this outbreak reported different outcomes for their subpopulations, and it appeared the overall estimates for the outbreak itself changed over time (Fukushima et al., 1999; Ikeda et al., 1999; Ikeda et al., 2000). Under-reporting for cases of foodborne disease, such as E. coli O157, is difficult to estimate and it is also possible that only the more severe cases of infection were captured during these studies. Together these could bias the summary estimates by inflating the reported prevalence of HUS.
Limitations specific to this systematic review and meta-analysis also need to be considered. A truly international perspective was not possible due to inaccessible articles and language restrictions. It is difficult to predict how the exclusion of 71 potentially relevant articles would affect the final outcome estimate. Considering the amount of unexplained heterogeneity and the lack of significance of the study-level factors explored in this review, further research into population-level effects is needed, and the exploration of results from countries such as those excluded from this review could be insightful. In addition, as multiple outcomes were taken from some studies, the assumption of independence of estimates for the meta-analysis was not met, which could lead to narrowing of confidence intervals. Post-hoc categorization of age group and group size should also be acknowledged as a limitation when interpreting the results and could potentially have contributed to the nonsignificant findings. Additionally, the use of a single reviewer for the first round of screening increased the potential to inappropriately exclude studies from this review; however, this round of screening was purposively designed to remove only the obvious irrelevant articles, and thus there was likely minimal impact. Finally, the methodological approach of using a logit transformation for the meta-analysis and regression introduces limitations to the resultant summary estimates, as the methodology may not be the most appropriate for low case counts. Currently, no formal methods exist to evaluate the potential impact of using the logit transform in this situation. Additional research comparing methodological approaches for prevalence estimates in a meta-analysis and meta-regression is required to clarify their effects on outcome estimates and the significance of these differences.
Conclusions
In conclusion, it was estimated that the number of cases of E. coli O157 that develop HUS ranged from 4% in groups with >1000 cases to 17% in groups with <50 cases. Although these proportions must be interpreted with caution due to the large amount of unexplained heterogeneity between studies, the high proportion of cases developing HUS indicates the need for further research to develop more accurate estimates of disease burden, as HUS is associated with severe or even fatal complications. Future studies are encouraged to report the following: 1. The follow-up between diagnosis as a case and sequelae diagnosis. 2. Detailed case definitions for the sequelae and probable cases of the pathogen. 3. Details of the diagnostic methods used to assess sequelae development. 4. Categorization of the sequelae by age categories to correspond to those used in international burden of illness studies. 5. Investigate potential sequelae following infection with non-O157 E. coli serogroups.
In addition, for accurate BOD estimates to be developed, a better understanding of additional chronic sequelae associated with E. coli O157 infection is required.
Footnotes
Acknowledgments
The authors thank Mai Pham, Ashley Whiteman, Dianna Wolfe, Tyler O'Neil, and Theresa Procter for technical assistance with this study. Funding for this research was received from a Canadian Institutes of Health Research (CIHR) Institute of Population and Public Health/Public Health Agency of Canada Applied Public Health Research Chair (awarded to J.M. Sargeant). In addition, financial and in-kind support was provided by the Public Health Agency of Canada.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.