
Abstract
A study was conducted over a 2-year period in the Perth District and Wellington-Dufferin-Guelph health units in Ontario, with an objective of using comparative genomic fingerprinting (CGF) with a 40-gene assay (CGF40) to investigate the association between human cases of campylobacteriosis and spatially and temporally related Campylobacter isolates from retail chicken. CGF results were available for isolates from 115 human cases and 718 retail chicken samples. These data were combined with CGF results from a large reference database of Campylobacter isolates. Isolates were categorized into types based on >90% CGF40 fingerprint similarity (CGF-90%). CGF-90% types were categorized as chicken associated (CA90) when the proportion of animal isolates in the given type that originated from chicken was at least 80% and was statistically significant. Risk factor data were collected from cases by questionnaire. Urban cases were significantly more likely than rural cases to be CA90 and there were significantly fewer CA90 cases in the second year of the study. Due to the population distribution in Canada and most industrialized countries, the majority of campylobacteriosis cases are urban dwellers. Therefore, the association between urban cases and chicken-associated types of Campylobacter emphasizes the importance of educational and food safety efforts to reduce the impact of Campylobacter from retail chicken on public health. Sources other than chicken may be more important for rural dwellers.
Introduction
C
In order to fully investigate the epidemiology of Campylobacter, it would be useful to distinguish epidemiologically linked isolates by molecular subtyping methods. Currently available methods, including pulsed-field gel electrophoresis, fla typing, amplified fragment length polymorphism, and multilocus sequence typing (MLST), have been problematic due to issues with their discriminatory ability as well as the financial resources and expertise they require (On et al., 2008; Clark et al., 2012; Taboada et al., 2012). The recently developed comparative genomic fingerprinting (CGF) method is a rapid, low cost and highly discriminatory alternative to MLST (Taboada et al., 2012). A study was conducted over 2 years in the Perth District (PD) and Wellington-Dufferin-Guelph (WDG) health units in Ontario, with an objective of investigating the relationship between sporadic cases of campylobacteriosis in humans and Campylobacter from retail chicken based on CGF subtyping.
Materials and Methods
Data collection and laboratory methods for this project have been previously described (Deckert et al., 2010, 2013). In brief, laboratory-confirmed human cases of campylobacteriosis living in these health units during the study period were eligible for inclusion in the study. Health unit personnel contacted cases, obtained consent for participation, and administered a telephone questionnaire. Case isolates were forwarded from private and hospital laboratories to the Public Health Ontario Laboratory for confirmation, speciation, and antimicrobial susceptibility testing. Isolates were matched with cases based on laboratory identification numbers. Over the same time period and geographical area, retail chicken samples were obtained according to a representative sampling plan. These samples were cultured at the Laboratory for Foodborne Zoonoses, Public Health Agency of Canada (LFZ-PHAC), and the resulting isolates were speciated and tested for antimicrobial susceptibility. Minimum inhibitory concentrations were determined by the E-test (Biomerieux, Durham, NC) for nine antimicrobials including ciprofloxacin (breakpoint: >4 μg/mL).
CGF utilizing a 40-gene assay (CGF40) was performed at the LFZ-PHAC on the study isolates from human cases and retail chicken (Taboada et al., 2012). Briefly, eight multiplex polymerase chain reaction (PCR) analyses were performed (each targeting five loci), and these PCR results were converted to binary values. Clusters were identified using the simple matching distance metric and unweighted-pair group method with average linkages at the 90% (CGF-90%) and 95% (CGF-95%) fingerprint similarity levels (Taboada et al., 2012). A reference database (RD) of over 6000 Campylobacter isolates from environmental, food, clinical, and animal (38% chicken, 6% wildlife, 51% other food animals, 5% horses, and 0.4% cats and dogs combined) sources from multiple surveillance and research initiatives was analyzed by CGF40 at LFZ-PHAC. This database included the retail chicken isolates from this study as well as retail chicken isolates from the C-Enternet program (Government of Canada, 2012) and the Canadian Integrated Program for Antimicrobial Resistance Surveillance (Government of Canada, 2010) as well as chicken fecal isolates.
Potential risk factor data for cases including age, gender, date of illness, income, underlying medical conditions, severity including hospitalization, antimicrobial use, chicken contact, chicken consumption, urban/rural residence, health unit of residence, and international travel were collected as part of the telephone questionnaire (Deckert et al., 2013). The University of Guelph Research Ethics Board approved this study.
Statistical analysis
Stata Intercooled version 12 (Stata Corporation, College Station, TX) was used for the analysis.
Using animal-origin isolates from the RD, CGF-90% types were classified as “chicken associated” (CA90) when the proportion of isolates in the given type that originated from chicken was at least 80% and was statistically significant with chi-square (CS) or Fisher's exact (FE) analysis, as appropriate. This process was repeated to classify “chicken associated” types at the CGF-95% level (CA95). Not included in this analysis were environmental and human clinical isolates from the RD.
Exact logistic regression, with CA90 as the outcome, was used to identify risk factors for human infection with “chicken associated” types. Variables significant at a p≤0.2 were considered for inclusion into the multivariable analysis. Variables with a prevalence of <2% among cases were omitted from further analysis. When variables were highly collinear (p<0.05), one was selected for inclusion into the multivariable analysis based on level of significance, number of missing observations, and reliability. This analysis was repeated using the CA95 classification as the outcome.
The preliminary main-effects exact logistic regression model was developed utilizing manual backward selection. When all remaining variables were significant at p≤0.05 or were confounders (removal changed the coefficient of another covariate by >20%), variables that were not significant in the univariable analysis were introduced and evaluated for significance and plausible interaction terms were assessed. The model was evaluated by comparing the observed and the expected values for each covariate pattern.
Results
Demographic and isolate speciation and susceptibility data from human cases and retail chicken from this study have been previously reported (Deckert et al., 2013). Briefly, 317 human cases were eligible for inclusion in the study, 250 (79%) consented to participate and completed the questionnaire, and isolates from 124 cases were received at the laboratory. Isolates from the remaining 126 cases were discarded in error at the primary laboratory or were unable to be matched with case data. One hundred and twenty-one isolates (97.6%) from human cases were Campylobacter jejuni and 3 (2.4%) were C. coli. Campylobacter was isolated from 749 of 1256 (59.6%) retail chicken samples (C. jejuni 90.4%, C. coli 8.7%, C. lari 0.9%). The prevalence of Campylobacter from retail chicken did not significantly differ between health units or between stores located in cities, towns, or villages but was significantly lower in year 2 of the study (year 1: 63.3%, year 2: 51.1%, p<0.001). Fourteen human isolates (1.9%) and six retail chicken isolates (4.8%) were resistant to ciprofloxacin.
Results from CGF analysis were available from 115 human isolates with 55 CGF-90% types or 75 CGF-95% types. There were 21 CA90 types, and nine of these were found in 30 human cases from this study (Fig. 1). There were 32 CA95 types, and 10 of these were found in 23 human cases. Eighteen cases had a CGF-90% type that was not present in the RD and thirty cases had a CGF-95% type that was not found in the RD. These cases were dropped from the CA90 and CA95 analyses respectively, since it could not be determined from the available data whether or not they were “chicken associated.” There were 2922 animal-source isolates from the RD, including 718 chicken isolates from this study, included in the CS/FE analysis.
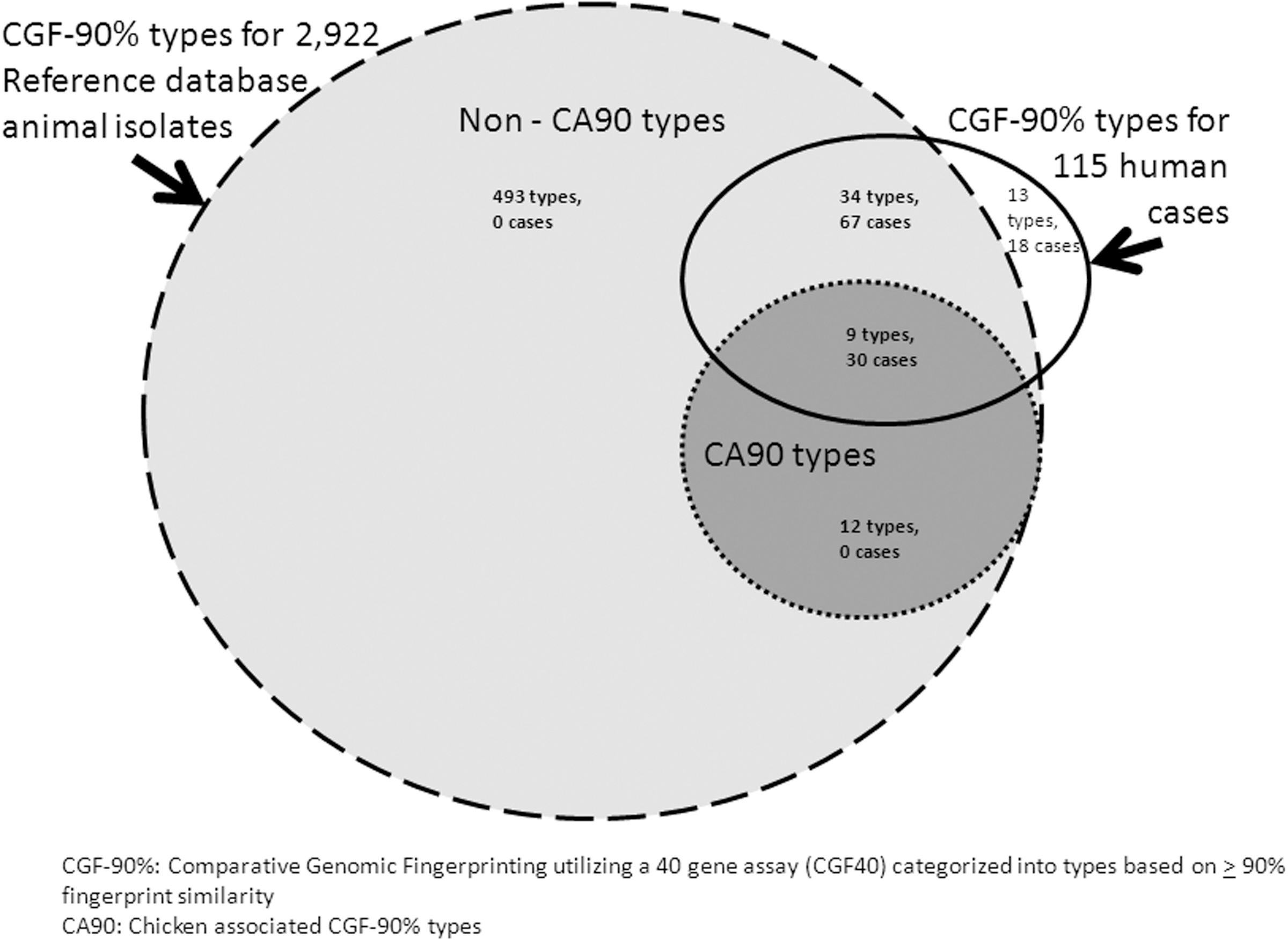
Comparative genomic fingerprint types with 90% fingerprint similarity in a reference database and in laboratory-confirmed cases of campylobacteriosis in Perth District and Wellington-Dufferin-Guelph health units.
Exact logistic regression analysis
Among cases included in the analysis, the median age was 24.5 (range: 0.3–85.7) years, 78% of cases occurred between June and November, the hospitalization rate was 9.3%, and approximately 50% of cases occurred in each year of the study. The proportion of urban cases was very similar in the two health units (WDG: 68%, PD: 66%). Furthermore, the proportion of urban and rural cases from the overall study that were included in the model dataset was similar (urban: 33%, rural: 41%, p=0.22). In the univariable analysis, season and year of illness were significantly associated with CA90 and collinear (r<− 0.3, p<0.001) (Table 1). Year (1 versus 2) was included in the multivariable model because it was more significantly associated with CA90. Residence type was self-reported and defined in the questionnaire as city or town/village/hamlet or rural. Categorization of urban (city, town, village, or hamlet) versus rural for the multivariable analysis was determined based on the results of univariable analysis. Additional variables that were assessed in the univariable analysis are described in Table 2. Although handling raw chicken was significantly associated with the outcome on univariable analysis, it was not submitted to the multivariable model due to the high proportion of missing observations (19.6%) (Table 2). The following variables were included in the multivariable model prior to backward selection: urban/rural residence, living on a farm with chickens, egg consumption, having a ciprofloxacin-resistant Campylobacter isolate, and year of illness. Following backward selection, the preliminary multivariable model included urban/rural residence and year of illness.
Model score: 19.93615; p=0.0001.
Comparative Genomic Fingerprinting with 40-gene assay.
Significant at p<0.2.
Not submitted to multivariable model due to high proportion of missing observations.
None of the nonsignificant variables in the univariable analysis were significant when added to the preliminary model. The residence/year interaction term was not significant. The evaluation of the model indicated that the observed and expected values were very similar.
Therefore, the final model included urban/rural residence and year of illness (Table 1). Cases living in a city or town were 6.3 times more likely to have an isolate with a CGF-90% type that was associated with chicken (i.e. CA90) than rural cases (Table 1). Cases from the second year of the study were 84% less likely to have a CA90 isolate (Table 1). An urban case in year 2 had a 3% less chance of having a CA90 isolate than an urban case in year 1, and a rural case in year 2 had an 84% less chance of having a CA90 isolate than a rural case in year 1. Although age was not statistically significant in the model, there was a significantly higher proportion of cases under the age of 5 in rural versus urban cases (35% versus 4%, p<0.001) and 85% of cases under the age of 5 were rural.
Exact logistic regression was also performed with CA95 as an outcome; however, no risk factor variables remained in the preliminary model, which was also nonsignificant.
Discussion
Urban cases (those self-reportings living in a city, town, village, or hamlet) were substantially more likely to have an isolate with a CGF-90% type that was chicken-associated than were nonurban cases (those self-reporting rural) (OR 6.3 [1.8–26.6]). This suggests that retail chicken may be a more important source of Campylobacter infection for those in an urban environment, while other sources may be more important for those living in a rural environment. These findings are consistent with studies in New Zealand and Scotland where urban cases were more likely to be infected with chicken MLST types than rural cases, particularly in children (Strachan et al., 2009; Mullner et al., 2010). Since age was not significant on univariable analysis or in the multivariable model, other factors may also play a role in the CA90 differences seen between rural and urban cases. These factors may include sources of Campylobacter other than chicken, such as cattle (direct contact, unpasteurized milk), and drinking or recreational water. Previous research has shown that ruminants may be a significant source of Campylobacter in human cases, particularly for young, rural children (Strachan et al., 2009, Mullner et al., 2010). Due to the low prevalence of Campylobacter on retail beef, it is likely that direct exposure to cattle, consumption of unpasteurized milk, and/or consumption of untreated water would be more important pathways of exposure than consumption of contaminated beef (Strachan et al., 2009; de Haan et al., 2010, Mullner et al., 2010). It would be expected that these pathways would put rural residents at a higher risk than urban residents. Also, older children and adults in rural environments may have higher levels of immunity to Campylobacter due to previous repeated exposure to these risk factors (Mullner et al., 2009; Government of Canada, 2010), which may have resulted in the relatively higher frequency of campylobacteriosis in rural children under the age of 5. The self-reporting of type of residence by cases may have resulted in misclassification bias.
There was no significant difference in the prevalence of Campylobacter on retail chicken between stores in cities versus towns and villages. This is not unexpected since there are three large corporations in the retail grocery business in Canada and meat products are primarily sourced at the corporate level, not the local level. Therefore, the source of poultry for an individual store is dependent on its corporate affiliation and not its location.
Year of illness was a significant variable in this model. The breakdown of cases between years in this study was similar (year 1: 56%, year 2: 44%, p>0.05). There was no significant difference in the proportion of the total cases from each year that were included in the model (year 1: 50/110, 45.5%; year 2: 39/122, 32.0%; p>0.05). There were approximately twice as many urban as rural cases in both years. There were also no significant differences between years with respect to bovine contact, drinking unpasteurized milk, or living on a farm with cattle. There was, however, a significant decrease in the prevalence of Campylobacter on retail chicken sampled in this study in year 2 versus year 1 (year 1: 304/480, 63.3%; year 2: 225/440, 51.1%; p<0.001). Therefore, the substantial drop in the proportion of human cases with a CA90 from year 1 to year 2 may be due to differences in the prevalence of Campylobacter on retail chicken, and/or risk factors not included in this study (e.g., climatic factors). It may also be due to risk factors that were included in the questionnaire but had a high number of missing observations. Although the odds of having a CA90 type were significantly reduced in year 2, urban cases in year 2 were still significantly more likely to have a CA90 type than rural cases.
Variables that assessed exposure to chicken through food were not significant in this model. Handling of raw chicken was significant on univariable analysis but was not included in the multivariable model due to the percentage of missing observations (19.6%). Several other variables related to chicken consumption also had a substantial percentage of missing observations including fresh chicken consumption (26.8%) and barbecued chicken consumption (23.7%). The inability to include these variables due to missing data is a limitation of the analysis and may have resulted from difficulty in recalling food history or the questionnaire length. Multiple routes of exposure combined with overall high levels of chicken handling and consumption in the population make the identification of specific risk factors for campylobacteriosis from chicken through the food pathway difficult (Neimann et al., 2003; Friedman et al., 2004; Domingues et al., 2012). This is further complicated by the possibility that older children and adults in rural environments may have higher levels of immunity to Campylobacter and may therefore be less susceptible to campylobacteriosis from chicken sources (Engberg, 2006).
Culture methods were standardized for all retail chicken samples. Private and hospital laboratories providing primary diagnostic services from human samples in Ontario must participate in the provincial proficiency program ensuring competency, which includes primary isolation of enteric pathogens such as Campylobacter. However, a bias may have resulted from differences between culture methods for human and retail chicken samples.
When the analysis was repeated with CGF-95% categorization, there were no significant results. Due to the strong tendency of Campylobacter toward recombination and mutation and the highly discriminatory power of CGF (Blaser et al., 1987; Belongia et al., 2003), typing based on a lower level of similarity (i.e., 90%) may be more useful when examining the relationship between human cases and potential risk factors for campylobacteriosis. An incomplete representation of chicken types in the RD at the 95% level or insufficient power may also have contributed to the lack of significant results.
The low cost and high volume capacity of the CGF40 method facilitated the analysis of all available chicken and human isolates from this study. In order to represent the maximum diversity of CGF types possible, data from the chicken isolates in this study were combined with the RD.
Isolates from environmental sources were excluded from the analysis used to identify CA90 types since these Campylobacter were expected to be the result of contamination from other sources (Clark et al., 2012). It is likely that some of these environmental isolates originated from chicken sources. Unfortunately, it is not possible through existing methods to identify the original source of Campylobacter isolates from water, sand, and other environments. Therefore, it is not possible to categorize the CGF90 types identified from these sources as “chicken associated” or “not chicken associated.” Although fluff samples may have been collected in poultry barns, they may represent sources other than chicken such as wild birds, rodents, and other poultry and therefore were excluded. Humans are not a reservoir for Campylobacter; therefore, isolates from human cases were excluded from this portion of the analysis (Engberg, 2006; Olson et al., 2008; Mullner et al., 2009). The use of CS/FE analysis in the first step of screening the CGF types ensured a minimum number of isolates in a specific type and avoided the inclusion of types with very small numbers of isolates, all of which were chicken (e.g., 1 of 1=100%) from being classified as CA90. The criterion that 80% of isolates in that type originate from chicken prevented the loss in specificity that would result if types with relatively low proportions of chicken isolates were included in the analysis.
The RD included in this study comprised isolates made available to LFZ-PHAC from a variety of research projects and ongoing surveillance programs. Due to the ad-hoc nature of the isolate collection, there may have been sampling bias and the RD may not be fully representative of all potential reservoirs of Campylobacter. However, in order to increase representativeness, isolates continue to be added to the RD and it will be a valuable resource for full source attribution analysis, which would contribute to the understanding of Campylobacter epidemiology.
Conclusions
Urban cases in this study were 6.3 times more likely than rural cases to have an isolate with a CGF-90% that was associated with chicken. Further research is required into the epidemiology of Campylobacter among rural cases, as factors other than exposure to chicken through the food chain may predominate. However, due to the population distribution in Canada and most industrialized countries, the majority of Campylobacter cases are urban dwellers. Therefore, the association between urban cases and chicken-associated types of Campylobacter emphasizes the importance of efforts to reduce the impact of Campylobacter from retail chicken on public health.
Footnotes
Acknowledgments
We wish to acknowledge C. Clarke, J. de Grosbois, for questionnaire administration, participating hospital and private laboratories for providing isolates, and S. Brown and K. Harris for speciation and antimicrobial susceptibility testing. We acknowledge R. Bean, N. Bunimov, K. Farrell, C. Gill, R. Imgrund, A. Mather, M.B. Varughese, and V. Young, who contributed to the sample processing, isolation, and characterization of the Campylobacter chicken isolates.
Disclosure Statement
No competing financial interests exist.