
Abstract
Estimating the actual occurrence of foodborne illness is challenging because only a small proportion of foodborne illnesses are confirmed and reported. Many studies have attempted to accurately estimate the overall number of cases of foodborne illness, but none have attempted to estimate the burden of foodborne disease in South Korea. This study used data from the Health Insurance Review and Assessment Service (HIRA), a public health surveillance system in South Korea, to calculate the number of cases and hospitalizations due to 18 specific pathogens and unspecified agents commonly transmitted through contaminated food between 2008 and 2012 in South Korea while accounting for uncertainty in the estimate. The estimated annual occurrences of foodborne illness were 336,138 (90% credible interval [CrI]: 258,379–430,740), with inpatient stays (hospitalizations), outpatient visits (foodborne disease infections), and patients' experiences (without visiting physicians) accounting for 2.3% (n=7809 [90% CrI: 7016–8616]), 14.4% (n=48,267 [90% CrI: 45,883–50,695]) and 83.3% (n=280,062 [90% CrI: 201,795–374,091]), respectively. Escherichia coli, including enterohemorrhagic E. coli, caused most illnesses, followed by nontyphoidal Salmonella spp., Staphylococcus aureus, hepatitis A virus, and norovirus. These results will be useful to food safety policymakers for the prevention and control of foodborne pathogens in South Korea.
Introduction
E
In national-level initiatives, England, The Netherlands, and the United States were the first countries to study the burden of foodborne disease, followed by Australia, Canada, and Ireland (Flint et al., 2005). These efforts identified many data gaps and methodological limitations, and now, better-developed data and methods have become available (Scallan et al., 2011a). Although the estimation of the overall number of episodes of foodborne illness is helpful for allocating resources and prioritizing interventions (Thomas et al., 2013), no attempts have been made yet to accurately estimate the burden of common foodborne diseases in South Korea. In addition, eating habits and differences in local food cultures may affect foodborne disease occurrence (Havelaar et al., 2010). The unique food culture of South Korea varies significantly from other countries and therefore may highlight key differences in the role of food culture in the occurrence of foodborne diseases patterns. Understanding the characteristics and causes of foodborne disease in South Korea is a critical component of understanding foodborne disease internationally.
The current study used data from the Health Insurance Review and Assessment Service (HIRA, 2013), an institute that reviews medical fees, to calculate the number of cases and hospitalizations due to 18 specific pathogens and unspecified agents commonly transmitted by contaminated food from 2008 to 2012 in South Korea.
Methods
Data collection on foodborne illness and infectious enteritis
Data on foodborne illness incidence were collected from the HIRA (2013) for the years 2008–2012. The HIRA reviews medical fees and evaluates the appropriateness of medical benefits provided to all South Korean patients. These data include the occurrence of foodborne illness and many other infectious diseases. From this data set, cases in which bacterial, viral, and protozoan foodborne diseases and intestinal infections had been diagnosed were collected using the Korean Standard Classification of Diseases (KSSC, 2014). Foodborne illnesses caused by natural toxins and chemical agents were not included because they fell outside the scope of the current study. The Korean Standard Classification of Diseases is based on and highly similar to the World Health Organization International Classification of Diseases, 10th Revision (ICD-10, 2010 update) but is adapted for use in South Korea. The ICD-10 assigns numeric codes to specific illnesses to standardize diagnostic criteria for epidemiological, health management, and clinical purposes (WHO, 2010). Thirty-seven ICD-10 codes define bacterial, viral, and protozoan foodborne illness and infectious enteritis (i.e., gastroenteritis): A02.0, A02.8–9, A03, A03.0–3, A03.8–9, A04.0–6, A04.8–9, A05.0–4, A05.8–9, A07.1–2, A07.8–9, A08.0–4, A32, B15, and B58 (Table 1). Cases that correspond to these codes were included and classified accordingly. Cases were then grouped according to inpatient stays (i.e., hospitalizations) and outpatient visits (i.e., foodborne disease infections).
Determining diagnostic accuracy
One concern with using the HIRA data is the accuracy of diagnosis by hospital physicians because HIRA data are collected from the first medical examination only. According to a study of medical diagnoses in South Korea in 2006 (KCDC, 2007), the proportion of false-diagnosis (including nonjudgment) was approximately 2.3% for inpatient stays and 8.0% for outpatient visits; these values were considered the diagnostic specificities, which were defined as 1 minus the false-diagnosis rate (i.e., 97.7% for inpatient stays and 92.0% for outpatient visits, as shown in Fig. 1). In addition, the agreement rate between the first and confirmed diagnoses by disease code was about 75.9% for inpatient stays and only 55.8% for outpatient visits; these values were considered the true-positive rates (diagnostic sensitivities). Thus, to capture the uncertainty associated with diagnostic specificity and sensitivity, 90% CI were calculated for the proportion of diagnostic accuracy (i.e., specificity and sensitivity) (Bluman, 2009). As shown in Figure 1, PERT (Project Evaluation and Review Techniques) distributions were used to capture the ranges (5th and 95th percentiles) and most likely values for the proportions of diagnostic specificities and sensitivities.
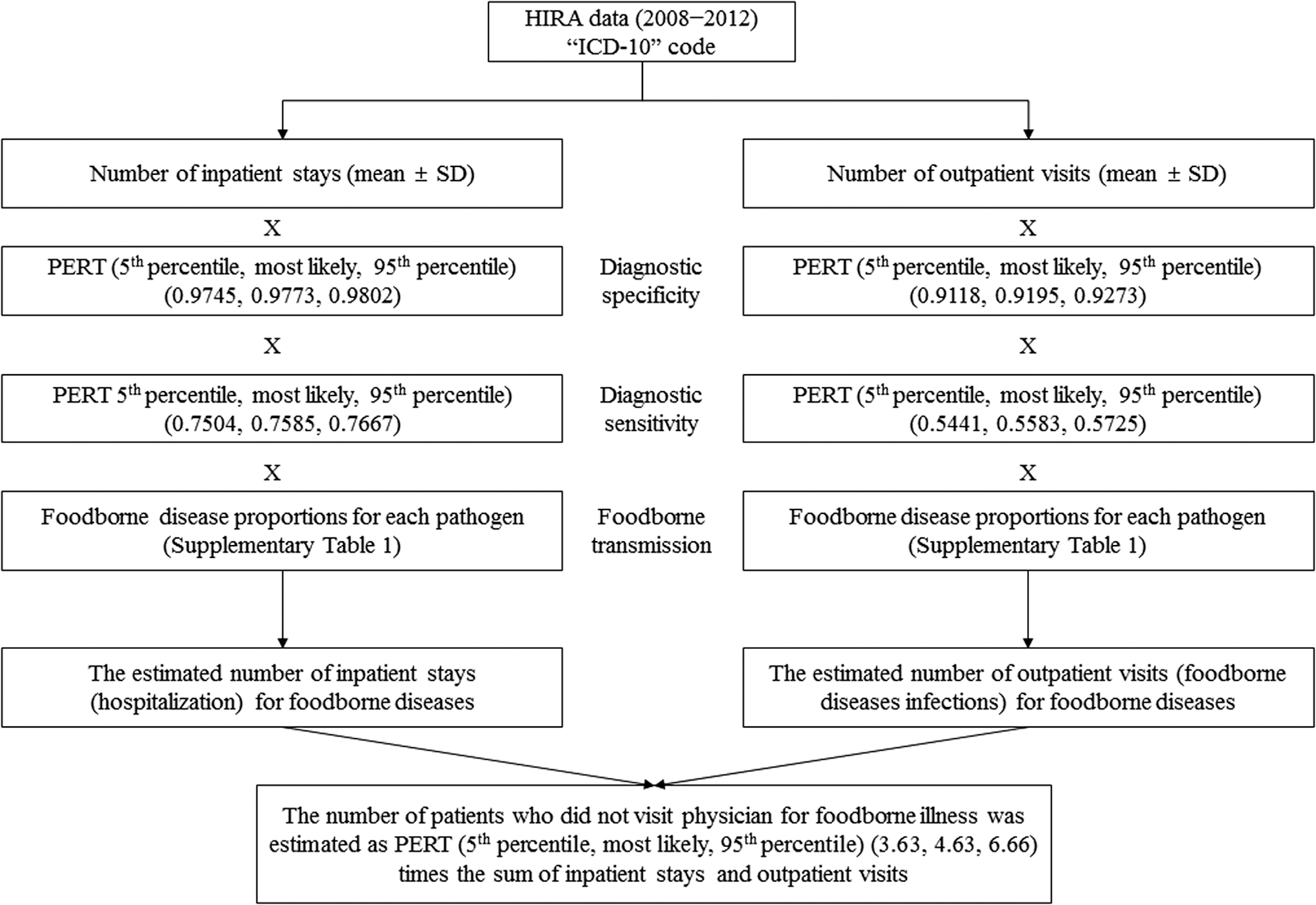
Scheme of data sources and methods used to estimate the number of inpatient stays (hospitalizations), outpatient visits (foodborne disease infections), and patients' experiences (without visiting physicians) of foodborne diseases in South Korea. HIRA, Health Insurance Review and Assessment Service; ICD-10, International Classification of Diseases, 10th Revision; ICD-10 codes are listed in Table 1; PERT, Project Evaluation and Review Techniques.
Determining proportion of illnesses caused by contaminated food
Foodborne illness is defined as any infectious gastroenteritis caused by eating food, including food contaminated just before eating (Hall et al., 2005). Therefore, it is important to estimate the proportion of pathogen-specific illnesses resulting from the consumption of contaminated food. Because not enough data are available in South Korea regarding the proportion of pathogens found in contaminated food, PERT distributions were used to account for uncertainty based on values estimated from Australian (Hall et al., 2005) and U.S. (Scallan et al., 2011a) data (Supplementary Table S1; Supplementary Data are available online at
Estimating patients' experiences of foodborne disease
Patients in the community who did not visit physicians were also considered when calculating the actual occurrence of foodborne diseases (Flint et al., 2005). Thus, we estimated the number of experiences (i.e., patients who did not visit physicians) of foodborne disease using survey results (Kim et al., 2015). According to this study, the number of patients' experiences of foodborne diseases in South Korea was about 4.63 (90% CI: 3.63–6.66) times the sum of inpatient stays and outpatient visits for foodborne diseases. As with the diagnostic specificities and sensitivities, the PERT distribution was also used to capture the range (5th and 95th percentiles) and most likely value for the proportion of patients' experiences of foodborne diseases (Fig. 1).
Data analysis and simulation for uncertainty
As shown in Figure 1, the estimated annual numbers of inpatient stays, outpatient visits, and patients' experiences with foodborne diseases were obtained by multiplying PERT distributions corresponding to diagnostic specificity and sensitivity, foodborne transmission, and patients' experiences with foodborne illness in proportion to the number of inpatients and outpatients extracted from HIRA data. The final estimates were generated using Monte Carlo simulation by @RISK6 software (Palisade, Newfield, NY), and the results from at least 100,000 iterations were analyzed to produce the overall simulation results. In simulation using @RISK, a Latin Hypercube sampling was selected for the sampling type, and for the generator seed, a seed was fixed as 1 to avoid variations between scenarios. Uncertainty in data was accounted for by the 5th and 95th percentile values (i.e., 90% credible interval [CrI]) from the simulation results following previously published methods (Hall et al., 2005; Scallan et al., 2011a). The estimates were based on the approximate South Korean population in 2010 (48,580,000 people) as a midpoint of the selected time period 2008–2012 (KOSIS, 2010).
Results
The 5-year annual average number of cases reported in HIRA from foodborne illness and infectious enteritis (i.e., acute gastroenteritis) in South Korea during 2008–2012 was 192,611±6132, with inpatient hospital stays and outpatient hospital visits estimated at 25,079±1495 and 167,532±8149, respectively (Table 1). From these data and using the method presented in Figure 1, foodborne disease cases caused by contaminated food were estimated at 336,138 (90% CrI: 258,379–430,740), with 2.3% (n=7,809 [90% CrI: 7,016–8,616]), 14.4% (n=48,267 [90% CrI: 45,883–50,695]), and 83.3% (n=280,062 [90% CrI: 201,795–374,091]) accounting for inpatient stays (hospitalizations), outpatient visits (foodborne disease infections), and patients' experiences (without visiting physicians), respectively. An estimated 314,104 cases (90% CrI: 241,456–402,649) were caused by bacterial infections (93.4%), 20,746 cases (90% CrI: 15,111–27,783) by viral infections (6.2%), and 1288 cases (90% CrI: 902–1,762) by parasites (0.4%). An estimated 92,444 (27.5%) cases were caused by 18 known foodborne pathogenic agents, whereas 243,694 (72.5%) cases were caused by miscellaneous (unspecified) (A04.8, A05.8, A08.3, A07.8) (17.4%) and unknown (A04.9, A05.9, A08.4, A07.9) (55.1%) agents (Table 1).
Pathogenic Escherichia coli (ICD-10 code A04.0–4) (87.4 cases per 100,000) caused most of the total foodborne illnesses, followed by nontyphoidal Salmonella spp. (A02.0, A02.8–9), Staphylococcus aureus, hepatitis A virus, and norovirus. However, the leading causes of hospitalizations were norovirus (60.3%), Clostridium botulinum (49.6%), enterohemorrhagic E. coli (46.3%) of pathogenic E. coli, Listeria spp. (46.3%), and hepatitis A virus (44.0%) (Table 2).
Discussion
In this study, the estimated annual number of foodborne disease cases caused by contaminated food in South Korea (attributed to 18 known pathogens and unspecified and unknown agents) was 336,138, including 7809 inpatient stays (hospitalizations), 48,257 outpatient visits (foodborne disease infections), and 280,062 patients' experiences (without visiting physicians), between 2008 and 2012. During the same period, 769 foodborne disease outbreaks affecting a mean of 6773 individuals per year were reported (KMFDS, 2013). This reported figure only accounts for cases identified and reported in South Korea. The estimated total number of cases caused by contaminated food was approximately 49.6 times the reported numbers.
In the current study, the methods used were suggested by Flint et al. (2005) and Hall et al. (2005) to estimate the extent of foodborne illness and included three components: (1) the total number of gastroenteritis cases in the country, (2) the proportion of gastroenteritis caused by foodborne pathogens, and (3) the proportion of experiences of foodborne diseases using survey results. The sum of these three estimates gives the actual burden of foodborne disease. The number of gastroenteritis cases (i.e., foodborne illness and infectious enteritis) in South Korea was determined based on the 37 ICD-10 codes from the HIRA data set. The HIRA data represent the total patient population in South Korea (HIRA, 2014). These HIRA data include the occurrence of foodborne illness and many other infectious diseases and can be used for public health surveillance. Therefore, the number of inpatient stays and outpatient visits is a more accurate indicator of the prevalence of foodborne illness. However, some weaknesses are associated with the HIRA data. The first is the limited accuracy of hospital physician diagnosis, even if sensitivity and specificity are considered. Although Hall et al. (2005) noted that any missed or faulty diagnoses for specific pathogens can be included in an unknown or a miscellaneous category; the current study used probability distributions to account for diagnostic uncertainty and performed Monte Carlo simulations to generate a mean estimate and 90% CrI. A second weakness is that it is unclear from the HIRA data what proportion represents cases in which a patient's illness was actually caused by contaminated food. In addition to contaminated food, transmission of foodborne pathogens to humans may occur from infected persons with secondary transmission, contaminated environments, or animals (Chin, 2000). As shown in Supplementary Table S1, some pathogens, such as Bacillus cereus and Clostridium perfringens, are believed to be transmitted by contaminated food, whereas others such as rotavirus and adenovirus are largely or probably transmitted by a fecal–oral route, with possible contact or respiratory spread through nonfoodborne routes (Koopmans and Duizer, 2004). Most foodborne pathogens have various paths of transmission to humans (Hall et al., 2005); therefore, it is difficult to accurately estimate the proportion of pathogen-specific illnesses resulting from the consumption of contaminated food (Scallan et al., 2011a). However, Hall et al. (2005) suggested that the overall proportion of infectious gastroenteritis in the community from foodborne transmission is estimated by dividing the sum of all cases from known pathogens by the sum of foodborne cases from known pathogens. Assuming that the proportion of gastroenteritis caused by foodborne pathogen transmission is the same internationally, the current study used values estimated from Australian (Hall et al., 2005) and U.S. (Scallan et al., 2011a) data because Korean data were unavailable. However, there are limits applied to these data and in particular for underdeveloped countries. Therefore, in order to take advantage of these data, the environmental and sanitary or food safety conditions in each country should be compared with the reference state (i.e., Australian and U.S. data). In this study, adjustments were made for the proportion estimated as acquired overseas for individuals and unknown pathogens. To reflect this uncertainty, probability distributions and Monte Carlo simulations were used to describe a range of plausible values for foodborne pathogen transmission. Finally, to estimate the number of individuals who experienced foodborne diseases but did not visit the hospital or a physician, we used survey results (Kim et al., 2015) because HIRA only collects hospital (inpatient and outpatient) diagnostic data. However, the proportion of experiences of foodborne illnesses was applied equally regardless of the type of causal pathogens. These survey results were used to adjust for underreporting, but the appropriate values for each pathogen are difficult to estimate. Therefore, further studies are needed to give more robust estimates of the true level of underreporting of the types of pathogens in the community.
In the United States, Scallan et al. (2011a) estimated that 31 known pathogens in contaminated food caused 55,961 hospitalizations annually. An Australian study estimated that 3640 hospitalizations occur annually because of food contaminated with 14 known pathogens (Hall et al., 2005). Our study shows that 18 known as well as unspecified and unknown pathogenic agents in contaminated food caused an estimated 7809 hospitalizations in South Korea. Comparisons among various country estimates are difficult to make, given the inherent differences in methodological approaches and data sources (Thomas et al., 2013). Furthermore, in this study in particular, the number of deaths from foodborne diseases was not included because HIRA data do not include mortality information. Thus, a direct comparison of mortality due to foodborne illnesses with other similar studies is not possible.
Compared with other countries, the main pathogens associated with foodborne diseases in South Korea are different, with E. coli, including enterohemorrhagic E. coli, and nontyphoidal Salmonella spp. representing about 61% of the total pathogen-specific diseases. However, many overseas national foodborne illness estimates, including those from the United States, Australia, The Netherlands, New Zealand, and France, indicate norovirus as a main contributor and Campylobacter spp. and nontyphoidal Salmonella spp. (particularly in the United States, Australia, New Zealand, France, the United Kingdom, and Greece) as the leading bacterial pathogens (Thomas et al., 2013). This difference may vary depending on the specific food culture (Havelaar et al., 2010), eating habits including the consumption of raw or lightly cooked food, and food consumption patterns and amounts (e.g., high intake of kimchi in South Korea, which is a unique traditional Korean food not typically consumed in other countries). In addition, environmental and sanitary conditions including food handling or public health systems for managing food safety policies in each country may be an important cause. The surveillance systems (e.g., lack of testing) and literacy of diagnostic systems operating in each country may influence this difference. On the other hand, the occurrence of foodborne pathogens depends on different time periods. Before 1960, the major causes of gastrointestinal disease were recognized as Salmonella spp., Shigella spp., and C. botulinum, and after the 1990s, they were norovirus, Campylobacter spp., and E. coli O157:H7 (Newell et al., 2010). However, norovirus and Campylobacter spp. infections have been increasingly recognized recently in South Korea (Korean Ministry of Food and Drug Safety, 2013), as in other countries. Therefore, future findings may be altered because of changing patterns in the pathogens responsible for foodborne diseases in South Korea.
Often, many foodborne illnesses are caused by unspecified or unknown pathogenic agents (Tauxe, 2002; Scallan et al., 2011b). Comprehensive diagnostic studies of intestinal infectious diseases indicate that between 50% and 60% of all causative agents are unidentified (Newell et al., 2010). The current study also shows that an estimated 55.1% and 17.4% of cases are caused by unknown and unspecified agents, respectively. In Australia, 30% of illnesses are caused by known pathogens (Hall et al., 2005), which is similar to the current finding of 27.5% in South Korea. Agents of foodborne illness continue to be discovered, such as Campylobacter spp. and E. coli O157, which were unknown only a few decades ago (Tauxe, 2002; Newell et al., 2010; Scallan et al., 2011b). More unknown pathogens are likely to be major causes of illness, some of which will become apparent with time and investigation (Hall et al., 2005).
Conclusions
Some of the methods and data used in the current study differ from those used in other countries (Hall et al., 2005; Scallan et al., 2011a; Thomas et al., 2013). There are not enough laboratory data from routine surveillance such as FoodNet (Jones et al., 2007) in the United States, except for data officially reported on foodborne diseases. Thus, we used the HIRA data as an alternative. Although this study provided an estimation of the annual number of foodborne disease cases caused by contaminated food in South Korea, future studies with high-quality data are needed to further refine foodborne illness estimates. Nevertheless, the current study is a first step toward improving data quality and methods to enhance the robustness of foodborne disease estimations in South Korea. This estimation will be useful for food safety policymakers to more precisely design prevention activities and to control and prioritize the effectiveness of risk management options for foodborne pathogen transmission in South Korea.
Footnotes
Acknowledgments
This research was supported by grants (13162KMFDS046) and (10162MFDS995) from Ministry of Food and Drug Safety in 2013 and 2014, Republic of Korea.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.