
Abstract
Improper food handling by consumers at home is a major cause of foodborne illness. Therefore, effective education strategies are essential to change consumers' food safety attitudes and behaviors. The purpose of this scoping review was to identify and characterize primary literature examining the effectiveness of consumer food-safety education interventions. Ten bibliographic databases were searched using a comprehensive search strategy. Citations were identified; two reviewers screened them for relevance and characterized relevant articles. To ensure results would be applicable to end users, stakeholders were engaged to provide input on the review scope, methods, and results. We identified 246 relevant articles, of which 150 were quantitative, 66 qualitative, and 30 mixed-method research studies. Most studies (64.2%) were published in the United States, using an uncontrolled before-and-after study design (31.3%), and investigated the effectiveness of community-based training sessions and workshops (52.0%). Research gaps were found in the number of randomized controlled studies conducted, academic- and school-based courses and curricula investigated, and interventions targeting high-risk populations (e.g., pregnant women, those who are immunocompromised) and using new media channels (e.g., social media). Key opportunities to enhance the utility of future primary research investigating consumer food-safety interventions include the following: using studies based on behavior-change theories and formative research; engaging the target population in the research; using validated instruments to measures outcomes; and reporting intervention characteristics and outcomes completely. Results of this review can be used to prioritize future primary research and decision-making in this area.
Introduction
F
Research shows that foodborne illness can be significantly attributed to unsafe consumer-level food handling (Worsfold and Griffith, 1997; Redmond and Griffith, 2003, 2004; Lee and Greig, 2010; Smadi and Sargeant, 2013). Consumers' food safety practices can have major implications in preventing foodborne illness, regardless of how well the food production industry performs (Haines, 2004; Munro et al., 2012).
Theories of behavior change, such as the Theory of Planned Behavior and Health Belief Model, indicate that as a precursor to implementing food-safety practices at home, consumers must first believe that they are susceptible to foodborne illness and that they are able to take measures to prevent it (Schafer et al., 1993; Takeuchi et al., 2005; Mullan, 2011). However, previous surveys found only 8–23% of consumers in the United States, Britain, and Canada believe they can contract foodborne illness through their practices at home (Redmond and Griffith, 2003; Nesbitt et al., 2009, 2014). Most consumers believe that food-processing plants and restaurants are responsible for the majority of foodborne illness (Redmond and Griffith, 2003; Nesbitt et al., 2009, 2014). The underestimation of risk associated with home preparation results in consumers often neglecting safe food-handling techniques.
Educational interventions to improve consumers' food-safety knowledge, attitudes, and behaviors are critical to mitigate the burden of foodborne illness from food prepared and consumed at home. Previous systematic reviews that summarized research in this area are outdated (Campbell et al., 1998; Mann et al., 2001) or had narrow inclusion criteria that limited the number of studies reviewed (Milton and Mullan, 2010). Therefore, we conducted a scoping review to identify and characterize global research investigating the effectiveness of consumer food-safety education interventions, inclusive of all possible education interventions and study designs. Scoping reviews use structured and transparent knowledge synthesis methodologies to “map out” the quantity, distribution, and characteristics of a broad research area (Arksey and O'Malley, 2005; Pham et al., 2014).
Methods
Review team, protocol, question, and scope
The review team consisted of all seven co-authors with multidisciplinary expertise in the topic area (i.e., consumer food safety) and methodology (i.e., knowledge synthesis). In addition, an expert advisory group was formed consisting of six individuals from various knowledge-user groups (Arksey and O'Malley, 2005). The group was consulted via email prior to conducting the review to provide input on the review protocol, scope, and search strategy.
A review protocol, developed a priori, outlined the methods and tools used in this review. The review question was, “What are the key characteristics of research investigating the effectiveness of consumer food-safety education interventions?” The review scope included all primary research (quantitative, qualitative, or mixed-method) published in English, French, or Spanish in any of the following formats: peer-reviewed journal articles, research reports, dissertations, and conference abstracts or papers. We defined consumers as home cooks and food handlers not employed in the food industry, including the following: the general public, targeted consumer groups (e.g., high-risk populations, students, ethnic groups), and volunteer food handlers for special food events. We also included any studies on educators of consumers (e.g., train-the-trainer). Relevant interventions included the following: community-based training sessions and workshops; academic institution- and school-based courses and curricula; social-marketing campaigns; and other educational materials and messaging (e.g., brochures, videos). Studies were excluded if the intervention was not directly related to food safety (e.g., generic hand-washing).
Search strategy
A comprehensive search strategy was developed by reviewing key terms in the titles and abstracts of 15 preselected relevant articles. A preliminary search algorithm was pretested in Scopus to ensure that all preselected articles were captured. The final search algorithm (Table 1 and Supplementary Data; Supplementary Data are available online at
Categories of terms combined with the AND operator. Search was conducted in the title, abstract, and keywords of citations.
The Environmental Health Review and the Journal of Nutrition Education and Behavior GEMs (Great Educational Materials) Collection were hand-searched to identify any references not captured by the electronic search. The expert advisory group provided potentially relevant unpublished studies or websites containing reports of relevant studies. Websites of 24 organizations and agencies were searched to identify relevant gray literature (e.g., research reports). The search strategy was verified by hand-searching the reference list of 15 relevant review articles and 15 purposively selected relevant primary research articles (lists available in Supplementary Data).
Relevance screening
Unique citations identified through the search strategy were screened for relevance at the title and abstract level using a relevance screening form (Supplementary Data) that contained one key question to assess the citation's relevance to the review question. When the relevance of a citation could not be determined with certainty, the full article was evaluated.
Article characterization
Full documents for all citations considered potentially relevant were characterized using a prespecified form containing 29 questions (Supplementary Data). The relevance of each article was confirmed and key characteristics extracted include the following: publication type and year; study design and data collection methods; details of interventions, populations, outcomes investigated; and reporting characteristics.
Review management and analysis
Search results were uploaded to RefWorks (Thomson ResearchSoft, Philadelphia, PA), manually de-duplicated, and imported into DistillerSR (Evidence Partners, Ottawa, ON, Canada) to conduct relevance screening and article characterization. We used 50 and 10 purposively selected abstracts and articles to pretest the screening and characterization forms, respectively. Pretest results were discussed among all reviewers and the forms were revised to clarify areas of uncertainty. Kappa scores for inclusion/exclusion agreement were assessed and additional citations were assigned as necessary until between-reviewer agreement was >0.8, which indicates almost perfect agreement and that the forms and eligibility criteria are sufficiently clear (Higgins and Green, 2011). Relevance screening and article characterization were conducted by two independent reviewers for each citation. Disagreements between reviewers were resolved by consensus and, when necessary, by judgment of a third reviewer.
Article characterization results were exported into Microsoft® Excel 2010 (Microsoft Corporation, Redmond, WA) and descriptively analyzed. Evidence maps were created to graphically represent cross-tabulations between publication year and region, study design, and intervention type. Publication year categories were selected so that each category would have a roughly similar number of articles.
Results
A total of 9559 unique citations were screened for relevance, of which 566 were characterized and 246 were confirmed as relevant (Fig. 1). The 246 relevant articles included 150 quantitative, 66 qualitative, and 30 mixed-method research studies that reported on 173 quantitative intervention efficacy studies and 86 qualitative studies with relevance to intervention research. A citation list of relevant articles is available in the Supplementary Data.
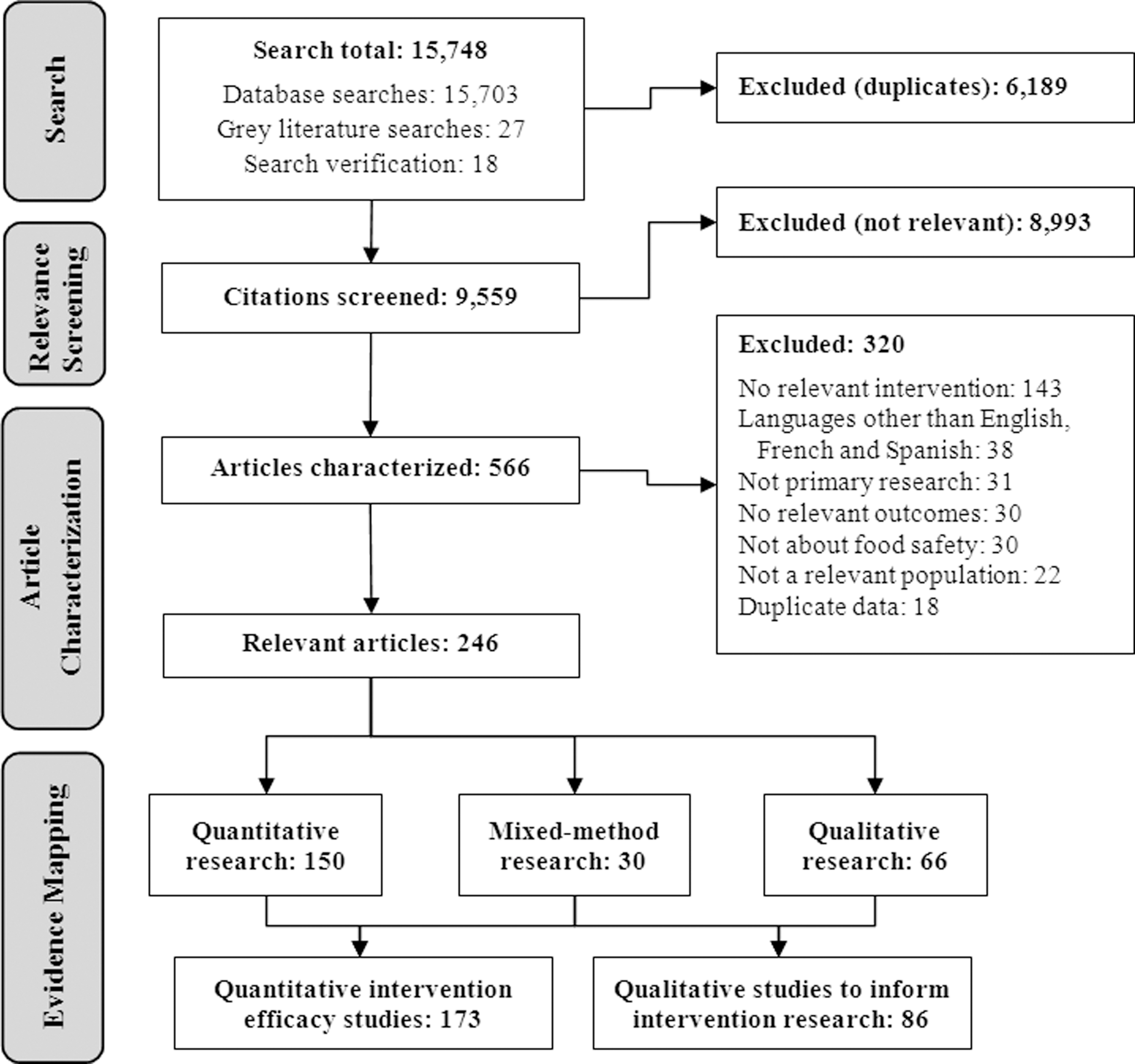
Scoping review flow-chart. Articles in other languages excluded from this review were published in Chinese (n=11), Korean (n=8), Portuguese (n=5), Japanese (n=5), Italian (n=2), German (n=2), Turkish (n=2), Polish (n=1), Lithuanian (n=1), and Hebrew (n=1). The numbers for “quantitative intervention efficacy studies” and “qualitative studies to inform intervention research” exceeds total number of included studies (n=246), as mixed-method research studies with both quantitative and qualitative components were included in both category counts.
The median publication year of relevant articles was 2006 (range: 1980–2014). All relevant articles were published in English, except for one published in Spanish. Table 2 shows the descriptive characteristics of all 246 articles. Most studies were conducted in North America (70.7%), mainly the United States (64.2%) (Table 2). Of the 173 quantitative studies, the majority (n=77) were uncontrolled before-and-after (UBA) studies (44.5%). Randomized controlled trials (RCTs) represented only a small proportion of all quantitative studies (13.9%). Figure 2 shows that the number of published UBA studies and RCTs has been increasing over the last 34 years.
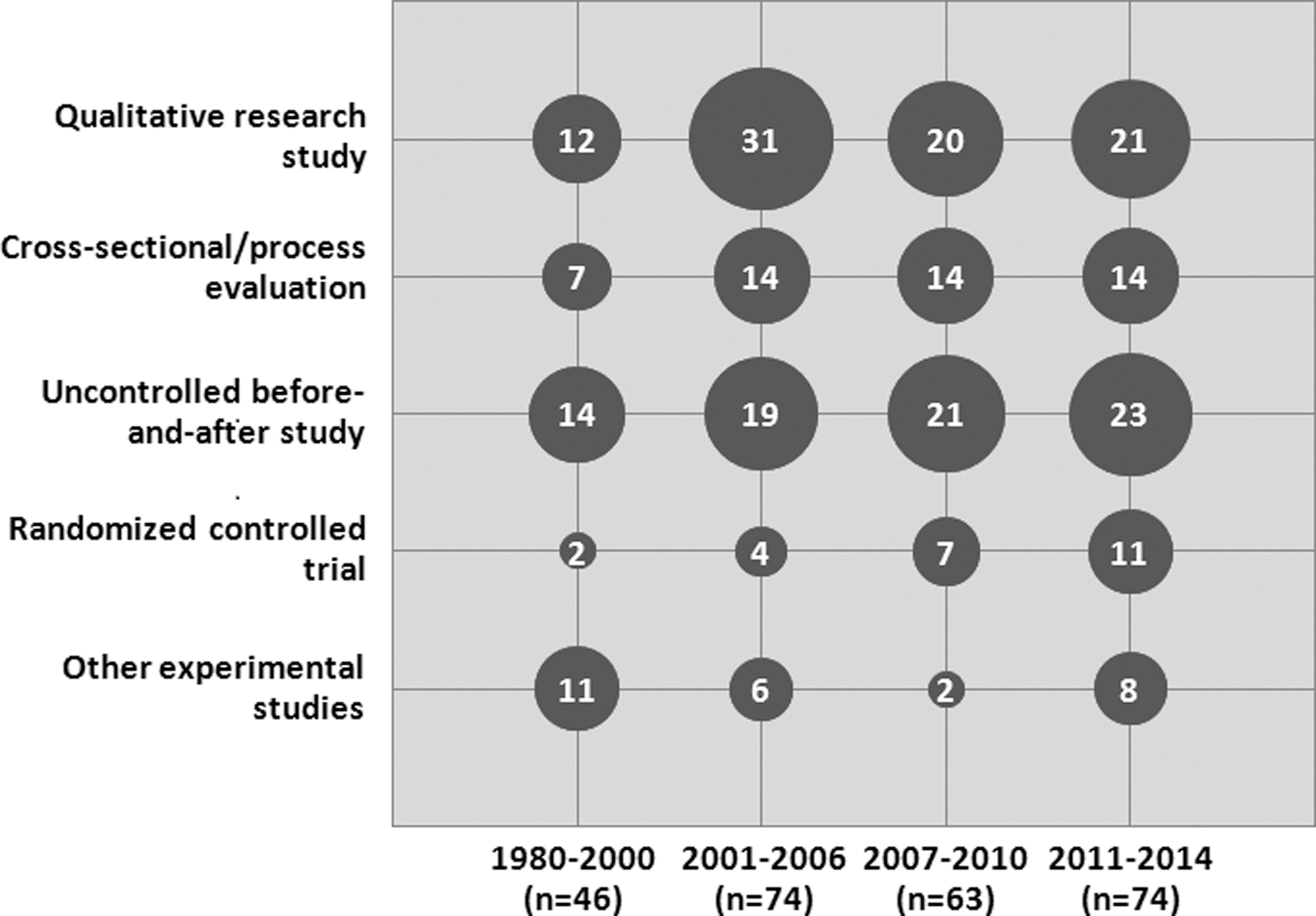
Evidence map of study design by publication year for 246 studies that investigated the effectiveness of food-safety education interventions for consumers. “Other experimental studies” includes controlled before-and-after studies, nonrandomized controlled trials, and a combination of both designs. Some articles reported more than one study design.
North America included United States (158) and Canada (16); Europe included the United Kingdom (12), Italy (6), Germany (4), Belgium (2), Netherlands (2), Turkey (2), Norway (1), Switzerland (1), Ireland (1), Greece (1), Denmark (1), Sweden (1), Malta (1), and Finland (1); Asia included India (9), Bangladesh (5), Vietnam (2), South Korea (2), China (2), United Arab Emirates (1), and Iran (1); Central and South America/Caribbean included El Salvador (2), Cuba (2), Jamaica (1), Brazil (1), and Guatemala (1).
Multiple selections were allowed for these questions; thus, column percentages do not add up to 100%.
This question was only tabulated for quantitative articles (n=173).
Other included microbiological and food testing (5), self-reflection (2), workshops (1), website analytics (1), scenario realism checks (1), and questionnaire via kiosk (1).
Table 3 shows the key sociodemographic characteristics of participants investigated in the studies. Most studies focused on consumers (93.1%) as the target population compared to educators of consumers (16.7%). The studies examined a wide range of target population groups. Interventions targeting caregivers (26.8%) and those with low-income/socioeconomic status (18.7%) were most common.
Multiple selections were allowed for these questions; thus, column percentages do not add up to 100%.
No interventions were identified that specifically targeted males.
Classified as high or low if stated in the original article.
Others included volunteers/staff at local community centers/food banks (n=6), food safety advisors/experts (3), farmers (2), extension agents (2), media personnel (1), sanitarians (1), fish suppliers (1), and government employees (1).
Caregivers include parents/caregivers of children, elderly, and ill individuals.
Other includes people who consume certain foods (e.g., fish, deli meat) (n=3), developmentally disabled (2), children living in single-parent households or two-working-parent households (1), home food preservers (1), and people involved in consumer organizations (1).
Quantitative research studies were further described by intervention type, content, delivery methods, and outcomes (Tables 4 and 5). Most quantitative studies examined the effectiveness of community-based training sessions and workshops (52.0%), compared to other intervention types. However, the number of studies evaluating published media campaigns and other messaging interventions has increased in recent years (Fig. 3). Included studies examined a wide range of intervention delivery methods, the most common being in-person training (62.4%), and content areas (Table 4). Approximately 26.6% and 40.5% of studies informed their interventions with a theory of behavior change or formative research, respectively. In addition, 45.7% of studies examining a theory-based intervention reported their outcomes in the context of theory. Most studies included a facilitator or instructor in the intervention delivery (65.9%), and 45.1% engaged participants in the development, delivery, and/or evaluation of the intervention. Intervention settings varied widely, most commonly being school or academic locations (32.4%).
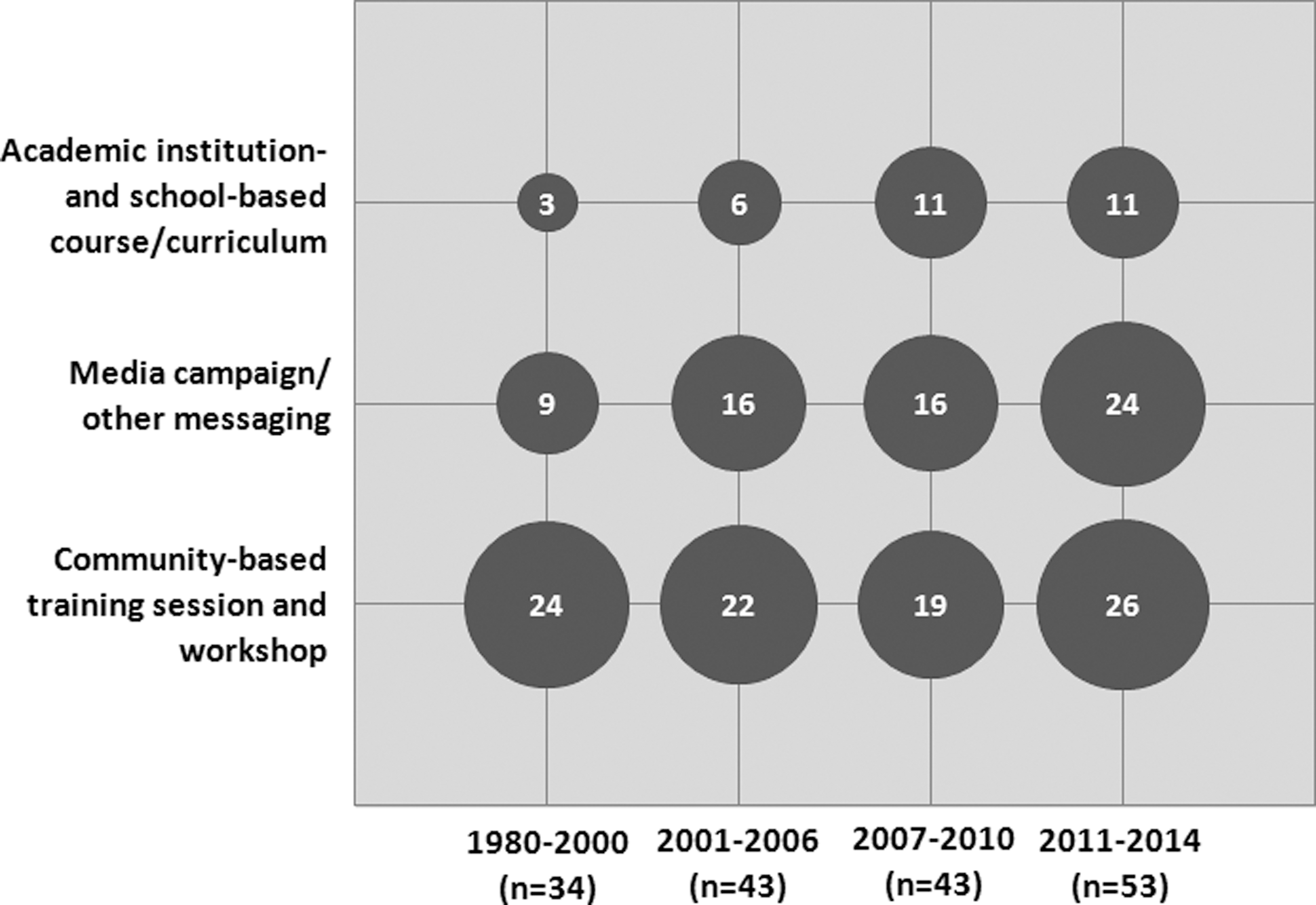
Evidence map of intervention type by publication year for 173 quantitative studies that investigated the effectiveness of food-safety education interventions for consumers. Some articles reported more than one intervention type.
Multiple selections were allowed for these questions; thus, column percentages do not add up to 100%.
Other includes experiential learning activities (n=4), self-audit/checklist of kitchen (3), mass emails (2), web-based video games (1), medical alerts (1), loudspeaker announcements (1), and online newspapers (1).
Other includes food preservation techniques (n=3), food-recall information (1), and Hazard Analysis Critical Control Points (1).
Nonfood safety topics included nutrition (n=43), food security (13), general sanitation/environmental hazards (13), physical activity/other life skills (10), other infectious diseases (3), childcare (2), agricultural literacy (1), and cultural diversity (1).
Other includes theories that were investigated in <5 articles.
This question was only tabulated for articles that indicated that the intervention was informed by a theory/model (n=46).
Other includes unspecified formative research (n=6), participant observations (n=4), and scenario realism checks (n=1).
Community members include student/adult volunteers from the community who helped out with the intervention.
Other includes researchers (n=5), food service personnel/students (n=4), job coaches (n=1), professional events management agency (n=1), change agents (n=1), social workers (n=1), and other specialized instructors (n=1).
Other includes school-teacher conventions (n=2), food-service centers (n=2), research centers (n=1), food banks (n=1), and community events (n=1).
Multiple selections were allowed for these questions; thus, column percentages do not add up to 100%.
Other includes health measures (n=3), campaign recall frequency (n=2), sources of information (n=1), emotions after reading messages (n=1), and economic measures (n=1).
This question was only tabulated for studies where intervention efficacy was measured (n=167).
Many different outcomes were used to measure the effectiveness of interventions, and many studies employed more than one (Table 5). Food-safety behaviors (67.1%) and knowledge (64.2%) were most commonly investigated. Most studies that measured behavior outcomes used self-reported measures (57.8%) compared to observing actual behaviors of participants (13.9%). Outcome measurement frequently occurred only once or twice (83.2%). Approximately 52% of quantitative studies did not specify whether measurement instruments were assessed for psychometric properties; 35.3% did not report the length of participant follow-up, while >40% reported some outcomes in an insufficient format to allow for potential meta-analysis.
Discussion
This review identified a variety of studies investigating the effectiveness of consumer food-safety education interventions. The majority of the studies were conducted in the United States, using a quasi-experimental UBA study design, and investigated the effectiveness of community-based training sessions and workshops. The data for many of these studies came from U.S. extension programs such as the Expanded Food and Nutrition Education Program, Supplemental Nutrition Assistance Program—Education, and the Special Supplemental Nutrition Program for Women, Infants, and Children. These programs generally target families and individuals with financial need (Trepka et al., 2006; National Institute of Food and Agriculture, 2013; USDA Food Nutrition Service, 2004). Although minor differences exist in specific topics covered by individual programs, they often include a range of related health topics (i.e., nutrition, physical activity, and food safety), which may help improve implementation cost-effectiveness (Trepka et al., 2006; USDA Food Nutrition Service, 2004).
High-risk populations are under-represented in the literature as targets of food-safety education strategies; these populations are more susceptible to foodborne illness and have unique needs requiring tailored interventions. A recent Canadian survey reported that consumers from high-risk groups such as immunocompromised (28%), pregnant women (27%), and elderly persons (11%) do not identify themselves as high risk (EKOS Research Associates Inc., 2010). Thirty-seven studies specifically targeted females, and no studies targeted males. Men are increasingly involved in household food handling, and greater numbers of single men are the primary caregivers of children (Cabrera et al., 2000; Gauthier et al., 2004). Future research should investigate gender-based differences in consumer food-safety education, as previous surveys found more high-risk food-handling practices (e.g., thawing frozen meat at room temperature) among males than females (Altekruse et al., 1999; Byrd-Bredbenner et al., 2007b; Nesbitt et al., 2009).
The majority of studies used an UBA design, which measured changes in outcomes using a pre- versus post-test without a control group. They are simpler and logistically easier than controlled trials; however, their utility to inform decision-making is limited due to the Hawthorne effect and other potential biases (Grimshaw et al., 2000; Eccles et al., 2003; Coalition for Evidence-Based Policy, 2007; Bhattacharyya et al., 2011). The Hawthorne effect is the overestimation of intervention effects because participants alter their behaviors due to the knowledge of being observed (Grimshaw et al., 2000). In addition, the possibility of secular trends and other external changes between pre- and post-tests limits our ability to attribute outcome changes to the intervention (Eccles et al., 2003; Coalition for Evidence-Based Policy, 2007; Bhattacharyya et al., 2011). The primary utility of UBA studies is to show “proof of concept” for the efficacy of interventions to inform more robust experimental designs (Coalition for Evidence-Based Policy, 2007). RCTs are the “gold standard” for determining intervention efficacy because the random allocation of participants to control and intervention groups controls for unmeasured confounding variables that could otherwise influence the results (Coalition for Evidence-Based Policy, 2007; Higgins and Green, 2011). Future RCTs should be prioritized for food-safety education interventions shown to be effective in UBA studies.
Effective community-based training sessions and workshops (52%) made up the majority of interventions. This is not surprising, since this category encompasses the U.S. Department of Agriculture–funded food-safety programs already described. Less research investigated the effectiveness of school-based courses despite arguments supporting the likelihood of health behaviors continuing into adulthood when introduced at a young age (Bandura, 2004; Viner and Macfarlane, 2005). Undergraduate college and university courses are other key points for food-safety education, as undergraduates typically begin to prepare their own food during this time (Morrone and Rathbun, 2003; Booth et al., 2013).
Studies on the use of media campaigns and other education tools (e.g., brochures, videos, web content) have increased in recent years (Fig. 3). We identified 7 articles published since 2010 that explored the effectiveness of social media-based interventions and 22 studies published since 2001 that investigated the effectiveness of online information/training interventions. This largely aligns with increasing accessibility to the Internet and preferences of young adults for social media and web-based food safety information (Jacob et al., 2010; Mayer and Harrison, 2012; Nesbitt et al., 2014). Alternatively, previous focus groups of elderly populations indicate a preference for traditional media (e.g., television, print media) (Cates et al., 2004; Powell, 2007; Kosa et al., 2011). This evidence highlights the need for researchers to carry out formative research to understand preferences, behaviors, and motivations of their target populations prior to designing interventions (Wright et al., 1998; Jacobs et al., 2012). Less than half of the studies in this review reported formative research in their studies. Only 41.5% of studies reported engagement of the target population in the development, delivery, and evaluation of interventions; this important step enhances research quality and credibility, health and community capacity outcomes, and research uptake (Viswanathan et al., 2004).
The 86 qualitative research studies were conducted for 2 main purposes: (1) to understand the needs of the target population prior to development of an intervention; and (2) to evaluate why an existing intervention was effective or not. Qualitative studies complement quantitative research by providing a better understanding of the underlying mechanisms and barriers to intervention effectiveness (Dixon-Woods et al., 2005). They should be considered for future primary research on food-safety education interventions in the context of formative research or to aid in process and outcome evaluation.
We found that only 26.6% of studies based their intervention on a theory of behavior change. Theories are important to consider when designing interventions, as they provide a framework to understand the process of behavior change, identify constructs influencing behavior, and measure intervention effectiveness using important outcomes (Prochaska and DiClemente, 1983; Rosenstock et al., 1988; Ajzen, 1991). In this review, the most commonly examined theories of behavior change were the Health Belief Model, Stages of Change Theory/Transtheoretical Model, and the Theory of Planned Behavior. The PRECEDE-PROCEED model frequently provided a framework to build health-promotion campaigns (Richard et al., 1996). When designing future food-safety education interventions, an appropriate theory should be selected based on target population needs, the situation at hand, and goals of the intervention (Angus et al., 2013).
A significant proportion of quantitative studies used self-reported behaviors, and only 13.9% observed participant behaviors. Self-reported behaviors are easier to collect, but can be subject to social desirability bias, which results in over-reporting of healthy behaviors by participants to be viewed more favorably by researchers (Redmond and Griffith, 2003; Dharod et al., 2007; Milton and Mullan, 2010). For example, washing hands and using thermometers are commonly over-reported food safety behaviors (Anderson et al., 2004; Dharod et al., 2007). However, it is difficult to develop an objective measure of behavioral assessment, as observations are also subject to biases such as the Hawthorne effect. Knowledge and awareness were the second most frequently investigated outcomes and tend to be assessed more objectively (e.g., using a scored test) than other measures (e.g., attitudes) if measurement instruments are valid and reliable. Knowledge is an important precursor of behavior change (Prochaska and DiClemente, 1983; Rosenstock et al., 1988; Ajzen, 1991), but it should be used together with other constructs of behavior as it may not always predict food-safety behavior outcomes on its own (Redmond and Griffith, 2003; Milton and Mullan, 2010; Mullan, 2011; Nesbitt et al., 2014). No matter what outcomes are measured, it is critical to ensure that outcome measurement tools be assessed for their psychometric properties. Validation prior to implementation ensures that instruments measure what they are intended to measure and that responses will be reproducible and consistent (Medeiros et al., 2001; Byrd-Bredbenner et al., 2007a).
Many studies did not report key intervention characteristics (e.g., setting and length of follow-up). These characteristics are important for proper assessment of study methodology and risk of bias. Additionally, most studies reported outcomes in an insufficient format for potential use in follow-up systematic reviews and meta-analysis. This is concerning, as previous research has shown that fully reported outcomes are more likely to be statistically significant than insufficiently reported outcomes (Dwan et al., 2013), which might provide a misleading summary of the evidence when synthesized in systematic reviews and meta-analysis. We encourage primary researchers in this field to follow internationally recommended reporting guidelines such as CONSORT for RCTs and TREND for nonrandomized controlled trials (Des Jarlais et al., 2004; Schulz et al., 2010).
A limitation of this review is the exclusion of 38 articles published in languages other than English, French, and Spanish, with the consequent exclusion of research conducted in some geographic regions (e.g., Asia). Additionally, some potentially relevant articles could have been missed by the search; however, we attempted to minimize this potential bias by conducting a comprehensive search verification.
Conclusions
We used a structured and transparent scoping review approach to summarize the distribution and characteristics of research on the effectiveness of consumer food-safety education interventions. Engagement of knowledge-users in an expert advisory group was useful to ensure the scope of this review, and its results were relevant and applicable to key stakeholders. Most relevant studies were conducted in the United States, using a UBA study design. There is a need for more RCTs on this subject, particularly on interventions shown to be effective in uncontrolled designs. Additional research is warranted to investigate interventions incorporating new technologies (e.g., social media), interventions in academic institutions and school settings, and those targeting high-risk populations. Key opportunities to enhance the utility of future primary research include designing and implementing interventions based on theories of behavior change and formative research, engaging the target population in the research, ensuring measurement instruments are valid and reliable, and appropriately reporting key study characteristics and outcomes.
Footnotes
Acknowledgments
We thank Judy Inglis and Janet Harris for search strategy input; Shannon Harding, Carl Uhland, Lea Nogueira-Borden, and Malcolm Weir for assistance in relevance screening and article characterization; and the Public Health Agency of Canada (PHAC) library staff for procurement assistance. We also thank the following members of the expert advisory group for their valued input on this review: Ken Diplock, Daniel Fong, Jessica Morris, Dr. Mike Cassidy, Barbara Marshall, and Andrea Nesbitt. This study was funded by the Laboratory for Foodborne Zoonoses, PHAC.
Disclosure Statement
No competing financial interests exist.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.