
Abstract
Background:
Enterotoxigenic Escherichia coli (ETEC) is one of the major causes of infectious diarrhea in developing countries. This study aimed to characterize the prevalence and phenotypic and genotypic features of ETEC isolates from Shenzhen, China.
Methods:
ETEC isolates were obtained from acute diarrheal patients and evaluated for enterotoxin, classical colonization factors (CFs), serotypes, antimicrobial susceptibility, and multilocus sequencing typing (MLST).
Results:
A total of 168 (1.3%) ETEC strains were isolated from 13,324 diarrheal outpatients during 2009 and 2014. A vast majority of ETEC-infected patients (82.1%) belonged to the age ranging 20–59 years and only six patients were children aged <5 years. Heat-stable toxin (ST) was most frequently detected (81.5%), followed by heat-labile toxin (LT) (13.1%). One or multiple colonization factors (CFs) were identified in 91 ETEC strains (54.2%). The most frequently detected CF was CS6 (with or without other CFs) (84/91), followed by CS21 (14/91). The most common serotype was O159:H34 (n = 36), followed by O148:H28 (n = 25) and O27:H7 (n = 17). High resistant rate was observed to nalidixic acid (77.4%), cephalothin (41.7%), ampicillin (34.5%), and tetracycline (21.4%). Antimicrobial resistance profiles differed among different serogroups. Sequence type (ST) 10 complex, integrated with connected ST218, ST48, ST4, and ST1312 subgroups, covered 73 (43.5%) isolates.
Conclusions:
ETEC isolates in Shenzhen of China appeared highly diverse, yet some isolates belonged to well-defined clonal groups sharing a unique set of virulence factors, serotypes, and MLST sequence types. Facing the challenge of ETEC antigenic diversity and geographic variation, novel molecules and/or classical antigens designed by novel strategies might contribute to ETEC vaccine development.
Introduction
E
Two major virulence determinants, enterotoxins and colonization factors (CFs), have been identified in ETEC strains (Gaastra and Svennerholm, 1996). Human ETEC isolates produce either or both types of enterotoxins, heat-stable toxin (ST) and heat-labile toxin (LT), and produce one or more CFs. ST can be further divided into human heat-stable toxin (STh) and porcine heat-stable toxin (STp) (Qadri et al., 2005; Konishi et al., 2011). Distinct types of CFs have been described in human ETEC isolates and more than 29 different CFs have been designated to date (e.g., CFA/I, CS1-CS8, CS12-CS15, and CS17-CS28) (Rania et al., 2011). Besides determination of the toxins and CFs, serotyping has been used to identify and characterize ETEC. More than 100 different serotypes have been record for ETEC (Steinsland et al., 2010).
Considering the great impact of ETEC infections on morbidity and mortality in developing countries, efforts to control infections through vaccination are actively being developed (Bourgeois et al., 2016). To ensure successful production and effective introduction of a vaccine, an inventory of global ETEC strain diversity is necessary.
Foodborne outbreaks caused by ETEC have been reported in China (Wang et al., 2007), but limited information about ETEC infections in sporadic diarrheal patients was recorded. Based on a laboratory-based sentinel surveillance system on infectious diarrheal disease in Shenzhen, a southern coastal city in China, we investigated the ETEC infections in Shenzhen, China and characterized the ETEC strains using phenotypic and genotypic typing systems. The information of ETEC strains obtained will give insights in developing effective vaccines.
Materials and Methods
Strain isolation and DNA extraction
Stool samples were collected from outpatients with acute diarrhea (defined as the passage of three or more stools per day with stool property abnormal, and the duration lasting no more than 2 weeks) in Shenzhen from 2009 to 2014. A sample collection form, including patient information of demographics, travel history, and clinic symptoms, was completed by the physician. Stool property, defined as loose, watery, or bloody stool, was identified by microbiologists who were responsible for strain isolation. Stool samples were enriched or directly inoculated on selective medium to isolate bacterial pathogens, including Salmonella spp., Shigella spp., Vibrio cholerae, V. parahaemolyticus, and diarrheagenic E. coli. For ETEC, stool samples were directly inoculated on CHROMagar ECC plates and incubated overnight at 37°C. Then, three E. coli-like blue colonies on ECC plates were randomly selected and inoculated on triple sugar iron (TSI) agar for further incubation, identification, and serotyping. After overnight incubation at 37°C, one loop of culture from each TSI agar was carefully picked and suspended into 200 μL of sterile purified water. After shaking thoroughly and boiling for 5 min, slurry was centrifuged at 12,000 rpm for 1 min and supernatant was collected as DNA templates for polymerase chain reaction (PCR).
Detecting genes of ETEC virulence factors
All templates prepared were screened for genes of estA1, estA2-4, and eltB, encoding STp, STh, and LT enterotoxins (Nada et al., 2010), respectively, using a modified molecular beacon-based multiplex real-time PCR assay (Chen et al., 2014). ETEC isolates were captured if any of these three genes was positive.
Genes encoding 20 CFs, including CFA/I, CS1 to CS8, CS12 to CS15, CS17 to CS22, and PCFO71, were determined using multiplex PCR assay described previously (Nada et al., 2010).
Serotyping
O and H antigens were determined using 52 O and 22 H (H2-H7, H9-H12, H16, H18-K21, H27, H28, H34, H40-H42, H45, and H51) antisera (Denka Seiken Co. Ltd., Tokyo, Japan) according to the instructions from the manufacturer. Isolates that did not react with any of the O or H antisera used were classified as nontypeable (ONT or HNT), and those that were nonmotile were denoted HNM (Blanco et al., 1991).
Antimicrobial resistance testing
Disc diffusion assay was used to determine the susceptibility of ETEC isolates to a panel of 21 antimicrobial agents. All antibiotic disks were purchased from Oxoid Ltd. (Hampshire, England). Breakpoints for sensitive, intermediate, and resistant were defined by the Clinical and Laboratory Standards Institute (CLSI) document M100-S26 (Clinical and Laboratory Standards Institute, 2016). E. coli ATCC25922 was used as a quality control.
Multilocus sequence typing
ETEC isolates were analyzed by multilocus sequencing typing (MLST) using the E. coli MLST (EcMLST) scheme, 1 which is based on sequencing of the internal regions of seven housekeeping genes adk, fumC, gyrB, icd, mdh, purA, and recA (Wirth et al., 2006; Nicklasson et al., 2010). PCR was performed as described on the MLST website. The allele numbers and corresponding sequence for each identified ETEC were obtained and MLST sequence type (ST) was assigned according to the EcMLST system website. Clonal complexes were analyzed using eBURST v3.0.
Results
Demographics of ETEC infections
A total of 168 (1.3%) ETEC strains were isolated from 13,324 enrolled outpatients. Only one genotype ETEC was captured from each of the 168 patients and no other bacterial pathogens tested were detected in these stool samples. Of all the 13,324 subjects enrolled, more than half were male (53.7%). Patients ranged from <1 month to 98 years (median age 26 years) and 1794 (14.7%) cases were children aged <5 years. While among the 168 ETEC-infected patients, 91(54.2%) were male and patients ranged from 4 months to 68 years (median age 30 years) without travel history in the past week. Vast majority of patients were adults aged from 20 to 59 years (82.1%) and only six patients were children aged <5 years. Most subjects had watery diarrhea (63.7%), 103 (61.3%) had abdominal pain, 34 (20.2%) experienced vomiting, and 25 (14.5%) had fever (Table 1). Altogether 135 ETEC infections detected (80.4%) were distributed in warm weather months from June to September, with the peak in August.
ETEC, enterotoxigenic Escherichia coli.
Genes of virulence factors and serotypes
Of all the 168 ETEC strains, ST-positive ETEC (ETEC-ST) was most frequently detected (81.5%), followed by LT-positive ETEC (ETEC-LT) (13.1%), and only nine strains were detected positive for both LT and STh (ETEC-LT-STh) (5.4%). STh was most frequently identified in the 137 ETEC-ST strains (74.4%) (Table 2).
CF, colonization factor; STh, human heat-stable toxin; STp, porcine heat-stable toxin; LT, heat-labile toxin.
One or multiple CFs were identified in more than half of ETEC strains (54.2%). The most frequently detected CF was CS6 (with or without other CFs) (84/91), followed by CS 21 (14/91). Other four CF members, including CS1, CS2, CS3, and CS8, were detected in concurrence with CS6 or CS21 (12/91) (Table 2).
The presence of CFs varies among ETEC strains with different enterotoxins. All the 35 ETEC-STp strains were detected positive for CS6 (100%). The percentages of CF-positive strains in ETEC-LT and ETEC-LT-STh strains were 81.8% (18/22) and 77.8% (7/9), respectively, while only 30.4% (31/102) of ETEC-STh strains were detected presenting CFs (Table 2).
Of all the 168 isolates, 13 O groups were detected, together with two strains with O nontypeable. The most common O groups were O159 (36.3%) and O148 (17.3%). Thirteen H types were detected in 91 strains, while 28 strains were H nontypeable and 8 were nonmotile. The most common serotype was O159:H34, followed by O148:H28 and O27:H7 (Table 2).
CF detectable strains in this study belonged to seven O groups, including O148, O159, O167, O169, O25, O27, and O6. The CF detection rate varied in different O groups. All O148, O167, and O169 strains were detected positive for at least one of the 20 CFs, while only 29.5% (18/61) of O159 strains had any of the 20 CFs. Multiple CFs were commonly found in the O6 group. However, none of the 20 CFs was detected in O15, O153, O168, O152, O44, O8, and ONT strains (Table 2).
Antimicrobial resistance
The 21 antimicrobial agents tested are listed in Table 3. Resistance to nalidixic acid was most common (77.4%) in the 168 ETEC isolates, followed by cephalothin (41.7%), ampicillin (34.5%), tetracycline (21.4%), and streptomycin (18.5%). No resistance to imipenem and meropenem was detected. Multidrug-resistant (MDR) isolates, defined as isolates resistant to at least three CLSI classes of antimicrobials (Clinical Laboratory Standards Institute, 2016), accounted for 18.5% of all studied isolates. The antimicrobial-resistant profiles differed among different serogroups. Higher resistance was found in serogroups O148, O27, and O25, especially to nalidixic acid, ampicillin, and cephalothin. MDR isolates were frequently distributed in serogroup O25 (47.1%) (Table 3).
NAL, nalidixic acid; CEP, cephalothin; AMP, ampicillin; TCY, tetracycline; STR, streptomycin; TMP, trimethoprim; SXT, trimethoprim/sulfamethoxazole; AMC, amoxicillin/clavulanic acid; CTX, cefotaxime; CRO, ceftriaxone; GEN, gentamicin; SAM, ampicillin/sulbactam; FEP, cefepime; KAN, kanamycin; CIP, ciprofloxacin; LVX, levofloxacin; CAZ, ceftazidime; FOX, cefoxitin; AMK, amikacin; CHL, chloramphenicol; IPM, imipenem; MEM, meropenem.
MDR, multidrug resistant, defined as resistant to at least three Clinical and Laboratory Standards Institute classes antimicrobials.
MLST analysis
The 168 ETEC isolates were represented with 56 different STs, of which only 23 STs were found in the database and the other 33 were novel types (ST3103-3152, except 3106, 3108, 3110-3115, 3119, 3120, 3122, 3128, 3136, 3141, 3144, 3146, and 3148) when submitting to the EcMLST database. Thirty-seven (66.1%) of the 56 STs were represented by single isolates, while the remaining 19 STs contained 2–33 isolates. The most prevalent genotypes were ST218 (n = 33), ST94 (n = 22), and ST316 (n = 16). These data indicted a very high degree of genetic diversity of ETEC.
The eBURST analysis separated the 56 STs into nine groups and 15 singletons. Of those nine groups, three were identified as ST complex, including ST10, ST94, and ST3103 complex. ST10 complex together with connected ST218, ST48, ST4, and ST1312 subgroups composed an integrated complex covering 73 (43.4%) isolates (Fig. 1). Relatively large numbers of isolates were found as ST316. However, only ST3152 was included in the same group as a single-locus variant of ST316.
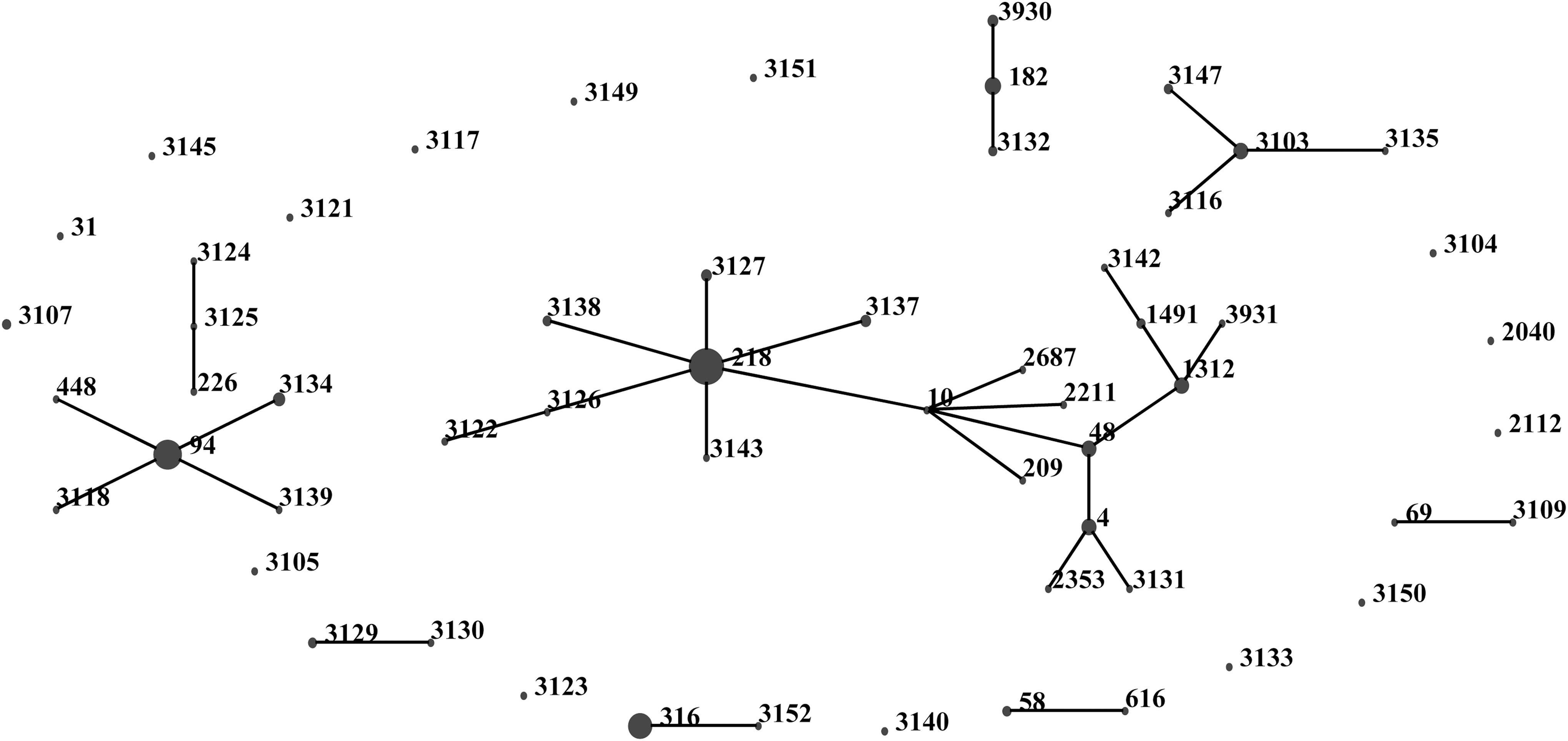
Enterotoxigenic Escherichia coli “population snapshot” obtained using eBURST v3. Nine groups were defined using stringent criteria (6/7 shared alleles). Among those nine groups, three were identified as clonal complexes, which were ST-10, ST-94, and ST3103 complex. STs that are single-locus variants of each other are shown connected by black lines. The sizes of the circles are relative to the number of strains in the ST. ST, stable toxin.
Clonal complexes had closed relationship with serogroup. ST218 subgroup and ST3103 complex were significantly related to serogroup O159, and ST94 complex was significantly related to serogroup O148. ST218 subgroup and ST94 complex were the dominant CCs in Shenzhen, so O159 and O148 ETEC isolates were largely found in this area. Similarly, clonal complexes had closed relationship with enterotoxin and CF types, for instance: ST218 subgroup and STh + ND, ST94 complex and STh + CS6, ST3103 complex and LT + CS6.
Discussion
This study provided comprehensive data on ETEC infections in diarrheal outpatients in Shenzhen, China, from 2009 to 2014. It made a distinction that a vast majority of (82.1%) ETEC-infected patients in Shenzhen were nontravel adults. Data gathered from our study, Beijing and Shanghai (Qu et al., 2014; Pan et al., 2015), showed ETEC mainly infected adults in China, which is different from commonly reported that ETEC usually affected children in developing countries and travelers to developing area (Bourgeois et al., 2016). ST, the most frequently found ETEC enterotoxin in Shenzhen, was detected in 81.5% strains. This pattern was also reported dominant in ETEC from patients in Beijing (Qu et al., 2014), Shanghai (Pan et al., 2015), and countries in Asia and Africa (Japan, Bangladesh, and Malawi) (Qadri et al., 2007; Konishi et al., 2011; Trainor et al., 2016), while other studies conducted in diarrheal patients in Peru (Rivera et al., 2010) and Nicaragua (Vilchez et al., 2014) reported that LT-producing ETEC was predominant. The relative proportions of enterotoxin-possessing isolates seem to vary across countries, population, and over time (Qadri et al., 2007; Rivera et al., 2013; Oh et al., 2014; Vilchez et al., 2014; Pan et al., 2015; Trainor et al., 2016). However, ST-producing ETEC was predominant in adults in China might be explained by the immunogenic and pathogenic difference between two enterotoxins. LT was strongly immunogenic and protective against ETEC, but ST was a nonantigenic low-molecular-weight peptide (Nada et al., 2013; Trainor et al., 2016). It was possible for people to acquire immunity to LT-producing ETEC over age, so as to infections with LT-producing ETEC decreased but ST-producing ETEC infections demonstrated predominantly in adults. In addition, ETEC-producing ST alone or both LT and ST were found to cause relatively more severe disease than that caused by LT-producing ETEC strains (Qadri et al., 2000). So, adults infected with ST-producing ETEC were more likely to seek medical care because of their severe symptoms. Thus, ETEC isolated from adults demonstrated ST predominance. LT-targeting vaccine might fail to protect adults from ETEC infection.
CFs were among the first virulence factors identified in ETEC and remained important targets for vaccine development (Bourgeois et al., 2016). More than 29 different CFs have been designated to date. However, CFs had not been detected on all ETEC. We searched 20 of 29 CFs and found about half of the ETEC strains having no detectable CFs, which was similar to the summary that roughly 30–50% of strains worldwide were found with no known CFs (Qadri et al., 2005; Bourgeois et al., 2016). This could be due to detection methodology, currently unknown CFs, or true absence of CFs. CS6 was one of the most common CFs worldwide, which was also the most frequently detected CF in our study and expressing on 92.3% ETEC strains with detectable CFs. Obviously, if a vaccine was developed targeting CFs, CS6 might be the key candidate.
It was commonly accepted that the presence of CFs varies among different toxic-type ETEC strains, and LT-producing ETEC strains had lower prevalence of CFs than ST-producing ETEC strains (Qadri et al., 2005; Rivera et al., 2010). However, different results were obtained in our study that most ETEC-LT strains (81.8%) were detected presenting CFs while more than 2/3 ETEC-STh strains were absent CFs tested. Similar phenomenon was also documented in the study in the U.S. military personnel (Nada et al., 2013). This might be the characteristics of ETEC strains from adults.
O159 was the most common O group ETEC in Shenzhen area, which was also reported common in southeastern China (Chen et al., 2014). Two types of H-antigens were detected in the O159 group and O159:H34 was the most common serotype in our study. However, only 6 of the 36 O159:H34 isolates had any of the 20 CFs tested. More CFs needed to be tested to further understand O159:H34. O148:H28 and O27:H7 were the other two common serotypes in our study with CS6 detected in all isolates. These two serotypes were among the top four ETEC serotypes causing outbreaks in Japan (Konishi et al., 2011) and also reported commonly in southeastern China (Chen et al., 2014). Another two serotypes, O6:H16 and O169:H41, which were reported causing outbreaks in the United States (Mark et al., 2004), Japan (Konishi et al., 2011; Harada et al., 2013), and Korea (Cho et al., 2014), were greatly worthy of concern henceforth.
Antimicrobials are of benefit in the treatment of diarrhea of travelers but not used routinely in treatment of childhood diarrhea. However, antimicrobial resistance emerged with time in ETEC isolates from both diarrheal travelers and children (Qadri et al., 2005; Vilchez et al., 2014). Resistance to common antimicrobials such as ampicillin, cephalothin, and tetracycline was frequently detected in ETEC strains in our study, similar to the reports in Peru, Korea, and southeastern/eastern China (Rivera et al., 2010; Chen et al., 2014; Oh et al., 2014; Pan et al., 2015). High-level and multidrug resistance had developed in ETEC in our study, which might be due to the widespread use of antimicrobials in Shenzhen area. Patients were usually prescribed antibiotics when diagnosed with bacterial infection based on the doctor's experience. It is fortunate that more strict prescription for antimicrobial use has been implemented in China in recent years and the concept of rational use of antimicrobials is being widely accepted by clinicians and general public.
Shenzhen ETEC strains have a widely diverse phylogenetic distribution represented in 23 known and 33 novel STs. Ample genetic diversity among ETEC strains from different geographic regions worldwide was reported previously (Nada et al., 2013). Integrated ST10 complex, including ST10, ST218, ST48, and 16 other sequence types, is dominant in Shenzhen, which was also reported as the most prevalent genotype in southeastern China (Chen et al., 2014). So, it is possible that ST10 complex prevailed in China.
Vaccine development remains a priority for ETEC prevention. Adhesins and toxins have been primarily targeted in ETEC vaccine development. However, big challenges arise because of the high diversity of CFs and enterotoxins. Novel molecules and/or classical antigens designed by novel strategies contributed to ETEC vaccine development. It is inspiring that two leading cellular candidates, ETVAX (a mixture of four inactivated strains) and ACE527 (a mixture of three live attenuated strains), are developed and found to be safe and immunogenic in Phase 1/2 trials (Bourgeois et al., 2016). Other ETEC vaccine candidates targeting protein subunits, toxoids (both LT and ST), or novel ETEC antigens provided broader protection coverage (Turner et al., 2011; Zhang et al., 2013; Fleckenstein et al., 2014; Bourgeois et al., 2016).
There are limitations in our study. First, compared to the data reported in Shanghai (4.4%), China (Huang et al., 2016), a lower ratio (1.3%) of diarrheal outpatients with ETEC isolated was found. This might due to the variation in region and population, or be caused by our method of picking three E. coli-like blue colonies on ECC plates for PCR identification. A higher isolation rate might be reached by picking more colonies from one plate. Second, not all currently described CF genes were tested in this study, although we have included the 20 CFs. Third, using the quantitative method to test antimicrobial susceptibility should provide more precise information than the disk diffusion method. Fourth, there might be uncertain causality of the isolated ETEC strains, given no virus detection data nor the ETEC baseline in healthy people. However, taken together, these data we present comprehensively demonstrate the local ETEC prevalence in the southern coastal region of China combining use of phenotypic and genotypic methods.
Conclusions
In summary, diarrheal outpatients infected with ETEC in the southern coastal region of China are mostly nontravel adults. Clinical ETEC isolates from this region are a highly diverse group of intestinal pathogens possessing various combinations of toxin type, CFs, serotype, antimicrobial resistance, and MLST sequence types. Despite the phenotypic and genotypic diversity, two predominant ST complexes of ST10 complex and ST 94 complex associated with certain toxin types, CFs, and serogroups were found. Considering the challenge of ETEC antigenic diversity and geographic variation, novel molecules and/or classical antigens designed by novel strategies might contribute to the ETEC vaccine development.
Footnotes
Acknowledgments
We thank the participants from sentinel hospitals for specimen collection, strain isolation, and data collection. We are grateful to John D. Klena from the U.S. Centers for Disease Control and Prevention for his insightful suggestions on the study design. We thank Lai-king Ng from the National Microbiology Laboratories, Public Health Agency, Canada, and Professor Jianguo Xu, Biao Kan, and Lu Ran from the Chinese Center for Disease Control and Prevention for their support and instructions on our work. We also thank Dr. Shuyu Wu from the U.S. Centers for Disease Control and Prevention for her constructive comments on the article. This work was supported by the China National Science and Technology Major Projects Foundation (No. 2012ZX10004215-003-005 and No. 2017ZX10303406).
Disclosure Statement
No competing financial interests exist.