
Abstract
Takeaway food services are an emerging business in China and have a potential impact on food safety. An unusual foodborne illness associated with takeaway food delivered through a logistics company on August 27, 2018 is reported. Epidemiological investigations showed that 28 patients from 2 companies were diagnosed with gastroenteritis symptoms. The major symptoms included nausea (24, 85.71%), vomiting (24, 85.71%), diarrhea (22, 78.57%), and abdominal pain (22, 78.75%). Laboratory investigations showed that six Staphylococcus aureus isolates, three Salmonella enteria serovar livingstone isolates, and one Vibrio parahaemolyticus isolate were detected. Six S. aureus isolates were detected from one patient, food, and a food handler, and all six S. aureus isolates had the same pulsed-field gel electrophoresis (PFGE) pattern and multilocus sequence typing (MLST) genotype. Staphylococcal enterotoxin A was detected from food and the six S. aureus isolates. These results confirmed that S. aureus isolates were the major agent causing this foodborne illness. Three Salmonella isolates with the same PFGE pattern and MLST genotype were detected from patients. This was the first time that Salmonella isolates have been identified as causing a foodborne disease outbreak in China. Only one O4:K8 serotype of V. parahaemolyticus with the tdh gene isolate was detected from one patient. These results confirmed that this was an unusual foodborne illness that included an outbreak associated with two different pathogens and a third pathogen sporadic illness. Takeaway services pose a risk to public health because they have the potential to distribute contaminated products over a large geographic area within a short time. Therefore, more attention should be paid to prevent and control foodborne illnesses caused by contaminated food from takeaway services.
Introduction
Foodborne illnesses are a major public health concern and are an important cause of morbidity and mortality worldwide. Foodborne illnesses are usually caused by the consumption of food or water contaminated with infectious microorganisms and/or toxic chemicals. Bacteria are a common cause of foodborne illness. In China, Salmonella species, Vibrio parahaemolyticus, Staphylococcus aureus, and diarrheagenic Escherichia coli have been the most common foodborne pathogens leading to outbreaks (Liu et al., 2004). The symptoms vary depending on the causative pathogen. The common clinical manifestations include vomiting, diarrhea, and abdominal pain (Havelaar et al., 2015). Other symptoms associated with V. parahaemolyticus and Salmonella spp. infection include watery diarrhea and fatigue. The incubation period is usually several hours. However, in some cases, such as Staphylococcal food poisoning, the onset of illness can be as soon as 30 min after ingesting contaminated food. Although foodborne illnesses may be mild and self-limiting, occasionally they are sufficiently severe to warrant hospitalization, particularly among young, old, pregnant, or immunosuppressed patients (Murray et al., 2005).
In China, people's life style, especially in big cities, has changed immensely along with the increased popularity of the internet in the past few years. Takeaway food has become more popular through online ordering systems. Takeaway food is often more convenient and economical compared with eating in restaurants. Takeaway food is usually prepared by restaurants, and then delivered to people through logistic companies. As takeaway food is fresh, it must be delivered to consumers in a short period. In China, takeaway food is usually consumed over a wide geographical area, but in the same city. As a result, contaminated takeaway food is also likely to be widely distributed, causing illnesses in multiple locations in the same city. Thus, takeaway food sold in this way could have a large impact on public health.
On August 27, 2018, the Jinshan District Center for Disease Control and Prevention, Shanghai, China (SHJSCDC) was notified of many gastroenteritis clusters by local hospitals. Note that in China, foodborne disease cases must be reported to the relevant government according to the regulations. In 2009, China established the National Foodborne Disease Surveillance Network, focusing on diarrheal cases and foodborne outbreak reporting. Jinshan district is one of the 16 districts in Shanghai. The 16 hospitals in Jinshan district are surveillance hospitals according to the National Foodborne Disease Surveillance Network. At 1 of the 16 hospitals, all the victims complained of symptoms at approximately the same time and were diagnosed with gastroenteritis. The SHJSCDC then conducted epidemiological and laboratory examinations. This article reports this unusual foodborne illness, including outbreak and sporadic illness, associated with takeaway food delivered through a logistics company.
Materials and Methods
Epidemiological investigation
The foodborne illness investigation was conducted in the afternoon at 5:30 p.m. on August 27, 2018. Epidemiologists from the local health departments first conducted the investigation to ascertain the full extent of the foodborne illness and its sources. Some of the epidemiologists were responsible for conducting an investigation of patients. They collected information of these patients including clinical symptoms, food and water histories in the last 3 d. At the same time, some of the epidemiologists were responsible for conducting an environmental investigation of the takeaway service, reviewing food process, and sales of food and purchase history of materials. They took further samples from patients, environmental, food, and food handlers for further laboratory investigation.
Laboratory investigation
The following samples were collected, including 1 stool sample from each of the 12 patients, 1 sample each of 3 leftover food items from the takeaway, 1 rectal swab from each of the 8 food handlers, 9 environmental items from the food processing environment, and 1 sample from each of 6 leftover food items from 2 companies (Table 1). All the samples were examined for bacterial pathogens in the SHJSCDC laboratories. All the samples were tested to isolate Salmonella spp., Shigella spp., E. coli, Vibrio spp., S. aureus, and Bacillus cereus according to the GB4789.4-2016, GB4789.5-2016, GB4789.6-2016, GB4789.7-2016, GB4789.10-2016, and GB4789.14-2016 National Food Safety Standards, respectively. In brief, the strains were inoculated onto selective medium after previous enrichment culture in selective enrichment broth. The strains were then identified using standard biochemical tests. B. cereus in the food samples was quantified as the colony-forming unit per gram. The food samples were tested for staphylococcal enterotoxins (SEs) SEA, SEB, SEC, SED, and SEE using the colloidal gold method.
Laboratory Investigation Results
The genetic traits of the pathogen isolates were examined in Shanghai municipal center for disease control and prevention.
The S. aureus isolates were subjected to enterotoxin gene isolation using polymerase chain reaction according to a previously described method (Zhang et al., 2012). The S. aureus isolates were screened for the expression of SEA, SEB, SEC, SED, and SEE using colloidal method. In addition, the S. aureus isolates were subjected to pulsed-field gel electrophoresis (PFGE) and multilocus sequence typing (MLST) (Enright et al., 2000; Harmsen et al., 2003).
One Salmonella isolate was subjected to serotyping, as determined by a conventional serotyping method according to GB 4789.4-2016. All Salmonella isolates were subjected to PFGE genotyping (Ribot et al., 2006).
One V. parahaemolyticus isolate was subjected to serotyping, detection of toxic genes tdh and trh, and analysis by PFGE genotyping using previously described methods (Zhang et al., 2013).
The antimicrobial susceptibility of all the isolated strains was determined using the minimal inhibitory concentration method according to the Clinical and Laboratory Standards Institute (CLSI, 2018). The antimicrobial agents tested for S. aureus were linezolid, nitrofurantoin, penicillin G, quinupristin–dalfopristin (SYN), rifampin, teicoplanin, tetracycline (TET), trimethoprim–sulfamethoxazole (SXT), and vancomycin. The antimicrobial agents tested for Salmonella enteria serovar livingstone and V. parahaemolyticus were ampicillin, ampicillin/sulbactam, cefazolin, TET, chloramphenicol, ciprofloxacin, SXT, ceftazidime, imipenem, nalidixic acid, cefoxitin, cefotaxime, gentamicin, and azithromycin. E. coli strain ATCC25922 and S. aureus strain ATCC29213 were used as controls.
Results
According to the sales records, a total of 201 takeaway food items were sold on August 27 to 4 companies where the workers were employed: 120 takeaway food items to company A (foodborne disease outbreak), 40 takeaway food items to company B company (foodborne disease outbreak), 29 takeaway food items to company C, and 12 takeaway food items to company D. A total of 28 patients from companies A and B were determined as having gastrointestinal symptoms. The major symptoms were nausea (85.71%), vomiting (85.71%), diarrhea (78.57%), and abdominal pain (78.75%) (Table 2). The median incubation period was 3 h (range, 0.5–5 h). Among these patients, 9 were men and 19 were women. All of them were hospitalized and none died. All 28 patients felt sick after consuming takeaway food at lunch. The investigation showed that they did eat the same food, and they did not contact the other patients in the past 3 d. They ate no food other than the takeaway food on August 27. Companies A and B supply hot drinking water to their employees; therefore, there was a very small possibility of contamination of the water in the two companies on the same day. As a result, these cases were determined as having a foodborne illness. The lunch included five kinds of food. The manufacturing practices of these foods were similar. All the materials used to produce these foods were purchased in the same market, and the purchase records were clear and intact. First, all these foods were cooked at a high temperature, usually >100°C, which was too high for microbial growth. Second, all these foods were subpacked in boxes by food handlers, which might represent a potential source of cross-contamination. Finally, all these foods were delivered to the four companies at the same time by the same logistics company.
Epidemiological Investigation Results
SFP, Staphylococcal foodborne poisoning.
Six S. aureus isolates were recovered from one patient, one food handler in the takeaway service, and four leftover items. Three Salmonella spp. isolates were recovered from three patients. The foodborne illness could be identified as outbreak according to World Health Organization (2008). An outbreak is defined as two or more cases of a similar illness resulting from ingestion of a common food, or if the food vehicle was undecided, sharing a common meal or food facility. A sporadic case is one that cannot be linked epidemiologically to other cases of the same illness. Only one V. parahaemolyticus isolate was recovered from one patient (Table 2), which caused sporadic illness. All the three pathogens were recovered from one patient. All the environmental swabs tested negative for bacterial pathogens. SEA was detected from two leftover food items.
The results showed that all the six S. aureus isolated from six samples expressed enterotoxin SEA, which was the same as that detected in the food items. In addition, the enterotoxin gene sea was detected in all the S. aureus isolates. Genotyping revealed that all six S. aureus isolates recovered from the patient, foods, and the one food handler had an identical PFGE pattern and the same MLST (ST7) (Fig. 1). Comparing the traits of three S. aureus isolates with those isolated from outbreak in 2012, the difference of PFGE patterns was significant, although they had the same MLST type, sea gene, SEA.

Dendrogram constructed from PFGE images of SmaI-digested genomic DNA of six Staphylococcus aureus isolates from this outbreak and three S. aureus isolates from outbreak in 2012. Strain identification number, year, source, toxin genes, enterotoxins, multilocus sequence type, spa type, and resistance are indicated. PFGE, pulsed-field gel electrophoresis.
The three Salmonella spp. isolates from three patients were identified as Salmonella enteria serovar livingstone and had an identical PFGE pattern (Fig. 2). The PFGE patterns among three S. livingstone isolates from this outbreak and one S. livingstone isolate from food in 2012 were the same (Fig. 2).
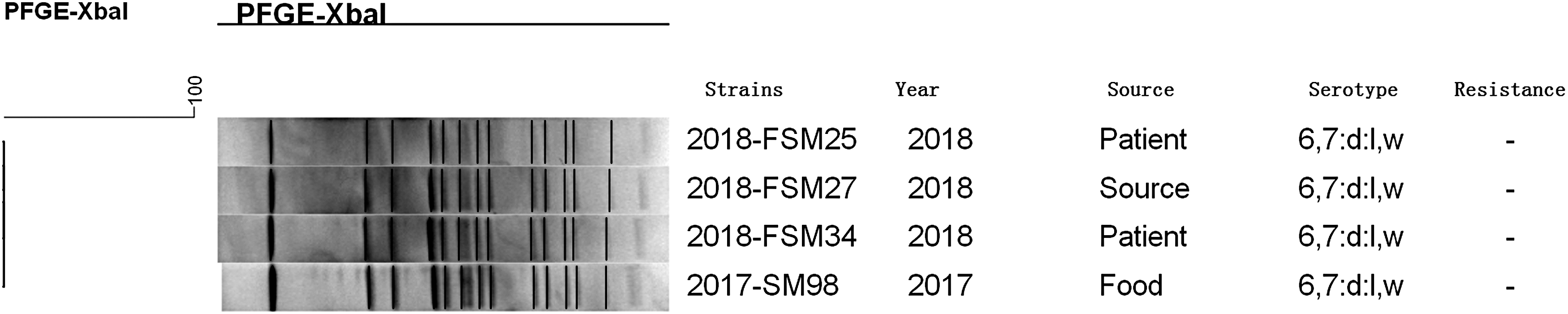
Dendrogram constructed from PFGE images of XbaI-digested genomic DNA of three Salmonella enteria serovar livingstone isolates from this outbreak and one S. livingstone isolate from food in 2017. Strain identification number, year, source, serotype, and resistance are indicated.
The V. parahaemolyticus isolate from one patient was identified as serotype O4:K8, having tdh gene.
All six S. aureus isolates were sensitive to most antibiotics in this study. They are resistant to penicillin and tetracycline. All 3 S. livingstone isolates and the 1 V. parahaemolyticus isolate were sensitive to all 14 antibiotics.
Discussion
This was an unusual foodborne illness for two reasons. First, the foodborne illnesses included two outbreak-related pathogens and the detection of another pathogen causing sporadic illnesses. Second, to the best of our knowledge, this is the first description of foodborne illness outbreak occurring in more than one company where the workers were employed at the same time caused by takeaway food in China. There is a little difference between takeaway food and fast food. The latter is produced according to standardized protocols, and is labeled. Chinese food is complex. In the past, food with complex cooking procedures was usually consumed at private residences or in restaurants. Nowadays, these foods, as takeaway food, can be delivered to consumers in a short period after being made by the restaurants. The takeaway food could then be consumed immediately with no other processing. The most common factors in outbreaks are improper cooking, contaminated ingredients, cross-contamination, and improper storage. However, for takeaway food, there are other factors. For example, improper packaging and an improper temperature could increase the potential hazard. Takeaway food has the potential to cause large-scale outbreaks because they can be distributed to a large geographical area within a short period. In this study, this unusual foodborne illness illustrates the food safety challenges posed by takeaway food.
In this case, multiple pathogens were detected. Six S. aureus isolates were recovered from leftover food, a patient, and a food handler. The major symptoms (namely vomiting and nausea), incubation period (0.5–5 h), and the presence of the enterotoxin SEA and enterotoxic gene sea among all six S. aureus isolates and food samples indicated that these S. aureus isolates were the most likely causative agent of the outbreak. By far the most common cause of staphylococcal food poisoning worldwide is SEA (Argudin et al., 2010), and our data showed SEA was the major agent that caused an outbreak during 2010 and 2012 in Shanghai, China (data unpublished). This was also the case in the present foodborne illness, with findings of enterotoxin A at the phenotypic and genotypic levels among the S. aureus isolates from the patient, food handler, and leftover food items (Fig. 1). At the same time, three S. livingstone isolates were recovered from three patients in this foodborne illness. The epidemiological investigations revealed the major symptoms (namely diarrhea and fatigue) and incubation period (the longest period time 5 h). As a result, we could confirm that S. livingstone isolates were the etiological agents of the outbreak according to WHO (2008). The PFGE fingerprints of the three isolates were the same (Fig. 2), which indicated they belonged to a single clone genetically. Of interest, only one V. parahaemolyticus isolate was recovered from one patient, which indicated that it caused a sporadic illness. The V. parahaemolyticus isolate was O4:K8 serotype with a tdh gene, which was also the major agent causing sporadic illness in China (data unpublished).
All six S. aureus with the same PFGE patterns were MLST ST7 in this foodborne illness. The MLST types causing outbreaks are diverse. ST188 and ST6 have been reported as the predominant types in Shenzhen, Guangdong province, China (Wang et al., 2011; Yan et al., 2012). ST1, ST59, and ST30 strains have been reported to be the most frequently isolated clones associated with staphylococcal foodborne poisoning in South Korea, Japan, and Thailand (Cha et al., 2006). The ST7 clone has caused one outbreak in 2012, in Shanghai, China. However, the differences of their PFGE patterns were significant, although they have the same sea gene and antimicrobial resistance pattern (Fig. 1). The difference might reflect the evolution of ST7 in its capacity to adapt to the environment and cause illness.
It has been reported that S. livingstone isolates have caused many outbreaks worldwide (Guerin et al., 2004; Eriksson et al., 2005). However, this is the first report of a foodborne outbreak caused by S. livingstone serotype in China. Our laboratory has surveilled Salmonella spp. in food in the past 10 years. The data showed that S. livingstone isolates are rare in food, only one S. livingstone isolate was isolated from food in 2017, which was the same as those isolated in the present outbreak for the same PFGE patterns and serotype. Unfortunately, the food source of the S. livingstone isolates in this outbreak could not be identified. It has been reported that the food sources of outbreaks are identified in only ∼50% of all foodborne illness outbreaks investigated (Gould et al., 2013). These results suggested the potential hazard of S. livingstone isolates in China, although they are not a common food pathogen.
Surprisingly, all three pathogens were recovered from one patient. The reason may be the patient's immunity was weak. Unfortunately, the rectal swab was not available for further analysis.
Four of the six S. aureus isolates were detected from four leftover food items, two of which contained SEA. Therefore, these foods might be the agents causing this foodborne illness. The manufacturing processes of these foods are similar. A critical point in terms of biological hazards is cross-contamination. The four kinds of food were prepacked in boxes by food handlers, which posed a potential for cross-contamination with the same S. aureus isolate detected from one of the food handlers. These foods were then delivered by one logistics company to four different companies (A–D) for consumption by hundreds of people at the same time. Ultimately, 28 people developed a foodborne illness from 2 of 4 companies. The occurrence of this foodborne illness was different from the results of national foodborne disease molecular tracing network (TraNet), which showed that foodborne disease in China were reported usually in restaurants, schools, or canteens (Li et al., 2017). It has been reported that >1000 people across Taiwan were infected by contaminated food from takeaway services (Wei et al., 2014). This foodborne illness illustrates the food safety challenges posed by takeaway services. However, the cause of the foodborne illness, that is, improper food-handling practice, is similar to that reported by TraNet. That is, foodborne disease in China is typically the result of improper food-handling practices or local food contamination (Li et al., 2017). Therefore, to prevent and control foodborne illness, food workers and consumers should receive training on how to avoid cross-contamination (Wu et al., 2014).
Conclusions
This foodborne illness was unusual in that it included an outbreak of illness caused by S. aureus and S. livingstone, and a sporadic illness caused by a V. parahaemolyticus. SEA was the key agent causing the foodborne illness.
This is the first report of a foodborne outbreak caused by S. livingstone isolates in China. The O4:K8 serotype V. parahaemolyticus with the toxic tdh gene caused sporadic illness in this foodborne illness, which is typical of this agent. Although this foodborne illness was likely caused by improper food-handling practices, it could have an enormous impact on public health because takeaway services have the potential to distribute contaminated products to a large geographical area within a short time. Therefore, more attention should be paid to prevent and control foodborne illness caused by contaminated food from takeaway services.
Footnotes
Acknowledgments
The authors thank Yunchang Guo (China National Center for Food Safety Risk Assessment) and Haijian Zhou (National Institute for Communication Disease Controland Prevention) for kindly providing suggestions in ![]() section. This study was supported by a grant from the Shanghai Municipal Natural Science Foundation (No. 15ZR1435000 to Hongzhi Zhang).
section. This study was supported by a grant from the Shanghai Municipal Natural Science Foundation (No. 15ZR1435000 to Hongzhi Zhang).
Disclosure Statement
No competing financial interests exist.