
Abstract
In Mexico, information of Salmonella enterica cases linked to food consumption is scarce. The objective of this article was to assess how S. enterica affect public health in Mexico. To conduct this study, data on the epidemiology of nontyphoidal S. enterica (NTS), Salmonella Typhi, and Salmonella Paratyphi A collected from 2000 to 2017 through the National Epidemiological Surveillance System of Mexico (Sistema Nacional de Vigilancia Epidemiológica de Mexico [SINAVE]) were used. Geographical distribution, season, age groups, and gender were variables considered to analyze S. enterica incidence. An estimation of cases caused by S. enterica in Mexico was calculated while considering data underestimation and the proportion of foodborne diseases. Information of the prevalence of the pathogen in food and the antimicrobial resistance of isolates from food and human cases were obtained from published studies. Outbreaks of S. enterica derived from imported Mexican products in the Unites States are discussed. In 2017, the numbers of reported cases of NTS (92,013) were two and seven times higher than the reported cases of Salmonella Typhi (45,280) and Salmonella Paratyphi A (12, 458). The NTS incidence was higher in lower socioeconomic Mexican regions. The gaps in the surveillance system make it impossible to establish a reliable tendency among age groups, geographical distribution, and gender. In 2017, the estimated frequency of NTS foodborne cases was 49 times higher than that reported in SINAVE, whereas for Salmonella Typhi and Salmonella Paratyphi A it was 23 times. Fresh meat showed the highest prevalence of S. enterica, and most of their isolates had multidrug resistance. Salmonella Typhimurium was the most common serotype isolated from human cases and food. Food safety agencies in Mexico need to prioritize efforts and resources to establish guidelines to ensure the absence of S. enterica in food.
Introduction
The World Health Organization (WHO) confirmed that nontyphoidal Salmonella enterica (NTS) serotypes and S. enterica serotype Typhi are major foodborne pathogens in the world that cause a high number of illnesses and deaths (WHO, 2015). NTS cause salmonellosis, a typical gastroenteritis characterized principally by diarrhea, abdominal pain, nausea, and sometimes vomiting; whereas Salmonella Typhi and Salmonella Paratyphi cause typhoid fever and paratyphoid fever, respectively. Both have similar symptoms: fever (39–40°C), fatigue, cephalea, nausea, abdominal pains, and constipation (Bhunia, 2008; Ao et al., 2015; WHO, 2015 WHO, 2018). It is well known that NTS is usually acquired through the consumption of contaminated food and water (Carrasco et al., 2012; Eng et al., 2015). However, the transmission of these pathogens can also occur from animals to humans (Sanchez et al., 2002; Bhunia, 2008; Behravesh et al., 2010; Freitas-Neto et al., 2010; Hoelzer et al., 2011). It is estimated that NTS causes 93.8 million illnesses annually worldwide, of which 85.6% are foodborne (Majowicz et al., 2010). In Latin America and the Caribbean (excluding Cuba), the WHO estimates that 7,049,467 foodborne illnesses, 814 foodborne deaths, and 54,495 foodborne disability-adjusted life years occur annually due to NTS (WHO, 2015). Due to a lack in data collection, especially in low-income regions, it is difficult to accurately estimate the health and economic impact caused by these pathogens.
S. enterica is the most reported foodborne pathogen annually in Mexico, according to a database from the National Epidemiological Surveillance System of Mexico (Sistema Nacional de Vigilancia Epidemiológica de Mexico [SINAVE]) (DGE, 2019). S. enterica in Mexico can be traced since 1545 according to an investigation conducted by Vågene et al. (2018). They suggested that Salmonella Paratyphi C was the most responsible of the major epidemics in the 16th century that affected many parts of Mexico.
In this review, an analysis of available information in the SINAVE database from 2000 to 2017 of S. enterica incidence in humans is presented. The prevalence of the pathogen in food items reported in published articles, as well as serotypes, antimicrobial resistance of S. enterica strains circulating in the country, and the Mexican food items linked to outbreaks reported in the United States, are also presented and discussed.
Data availability
S. enterica incidence data
Data for S. enterica epidemiology analysis were obtained from the SINAVE morbidity yearbook, in which the data are divided by age, state, age group, or health center (
S. enterica prevalence in food and antimicrobial resistance of isolates data
S. enterica prevalence in food items and antimicrobial resistance of isolates data was obtained from online published papers from 2000 to 2017. The electronic databases used were PubMed, Google Scholar, and Science Research, and the keywords for the search were: “prevalence, occurrence, frequency or incidence,” “antimicrobial resistance,” “Salmonella,” “human cases,” “the specific food item (produce, fresh meat, processed meat products, eggs, dairy products, and seafood),” and “Mexico.” All available papers found in the databases mentioned earlier were used. Regarding S. enterica prevalence in food, 33 papers were retrieved, and only 10 were retrieved for antimicrobial resistance.
Epidemiology analysis of S. enterica in Mexico and illness estimation for food consumption
SINAVE information reported the epidemiological situation of NTS, Salmonella Typhi, and Salmonella Paratyphi A in Mexico. The information presented in this article did not represent the total coverage of S. enterica illnesses in the country, because only laboratory-confirmed cases are reported, causing an underestimation. The underestimation is mainly presented, because not all people have access to health services, not all sick people go to medical care units that belong to the National Health System of Mexico, and not all people who receive medical attention are diagnosed by a laboratory test. The National Health System of Mexico includes medical care units of the public sector attending people with and without social security (Dantés et al., 2011). The 99.1% of the population that has access to health services is attended by the public sector (CONEVAL, 2018). Over time, the percentage of people who lack access to health services has been decreasing, from 58.6% in 2000 to 15.5% in 2016 (CONEVAL, 2017). In addition, improvements in data coverage collection and analysis have been observed over time (SS/DGE, 2014), and coverage of reported cases has been increasing, having an impact on the incidence rate (IR). The improvements in health services and data collection may lead to a bias in the available information before 2013, the year in which changes in legislation and health care system were implemented.
Despite these limitations, the data presented later can help to understand the actual epidemiological situation of NTS, Salmonella Typhi, and Salmonella Paratyphi A in Mexico and their changes over time.
According to the available data from the morbidity yearbook of SINAVE from 2000 to 2013, the number of cases of NTS and Salmonella Paratyphi A was presented together, reporting a total of 1,538,909 cases. From 2014, data were separated, reporting 317,685 cases of NTS and 48,939 cases of Salmonella Paratyphi A until 2017 (DGE, 2019). Regarding Salmonella Typhi, 654,636 cases were reported from 2000 to 2017. The cases reported are classified according to the source of the etiological agent, making it impossible to distinguish those that are specifically attributed to food consumption.
The last complete annual report in 2017 showed 92,013 cases of NTS, 45,280 cases of Salmonella Typhi, and 12, 458 cases of Salmonella Paratyphi A, which means that the number of NTS cases were two and seven times higher than those of Salmonella Typhi and Salmonella Paratyphi A (DGE, 2019).
Figure 1 shows the number of cases and IR per 100,000 people for NTS, Salmonella Typhi, and Salmonella Paratyphi A in Mexico. From 2000 to 2002, the number of typhoid fever cases reported was lower than NTS, and from 2003 this increased over time, showing a small reduction in 2016. However, in the case of NTS and Salmonella Paratyphi A, in 2013, a decrease of 38.7% and 37.9% in IR and the number of reported cases was observed, respectively. From 2014, NTS and Salmonella Paratyphi A were separated in the Morbidity Yearbook, showing in 2017 an increase in NTS IR (23.5%) and reported cases (23.5%). The difference in the trend of Salmonella Typhi, Salmonella Paratyphi A, and NTS cases and IR suggests that the Mexican population has a higher exposure to NTS and that nontyphoidal serotypes could be circulating more than Salmonella Typhi and Salmonella Paratyphi A.
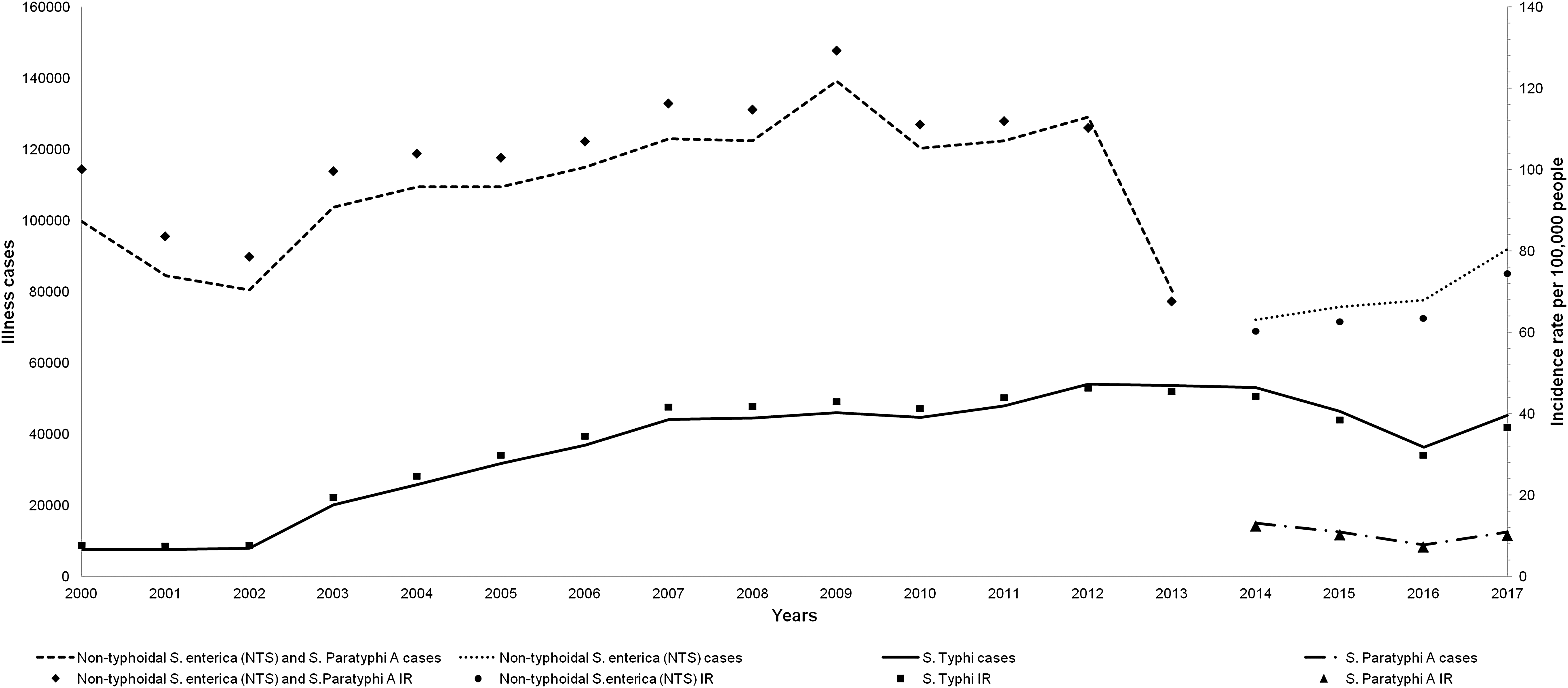
Cases of illness and IR caused by Salmonella enterica in Mexico. Figure was prepared by using the available information of reported cases by yearbook morbidity of SINAVE. IR per 100,000 people. IR, incidence rate; SINAVE, Sistema Nacional de Vigilancia Epidemiológica de Mexico.
The implementation of the Mexican norm “NOM-017-SSA2-2012” for the information collection and the increase in the coverage of health access at that time resulted in increased coverage of collected data from 2013.
In the whole country, the average IR per 100,000 for NTS (2014–2017), Salmonella Typhi (2000–2017), and Salmonella Paratyphi A (2014–2017) were 65.2, 32.4, and 10.1, respectively. According to the National Institute of Statistics and Geography of Mexico (Instituto Nacional de Estadística y Geografía [INEGI]), the country is divided into seven socioeconomic regions grouped according to seven factors: home infrastructure, home quality, home equipment, overcrowding, health, education, and employment. The socioeconomic level could be related to the IR of these diseases (Fig. 2). NTS had the highest IR per 100,000 people in the whole country, with Chiapas (IR = 396.7 per 100,000 people) and Tabasco (IR = 338.4 per 100,000 people) being the most affected states. In the case of Salmonella Typhi, the state of Sinaloa had the highest IR (IR = 267.6 per 100,000 people), followed by Tamaulipas (IR = 145.0 per 100,000 people), Tabasco (IR = 133.9 per 100,000 people), and Zacatecas (IR = 122.3 per 100,000 people). For Salmonella Paratyphi A, the state of Tabasco was most affected, reporting an 82.7 IR per 100,000 people, followed by Chiapas, Sinaloa, and Quintana Roo, with 39.4, 31.4, and 30.4 IR per 100,000 people, respectively. Chiapas and Tabasco, states with the highest NTS IR values, are classified within the less favorable socioeconomic regions in Mexico (CONEVAL, 2017). Even though the access to health services across the states is not equal, having a minimal impact on the number of reported illnesses, the health infrastructure could be crucial for the correct diagnosis; as a result, this could produce a bias in the reported incidence of Salmonella Typhi.
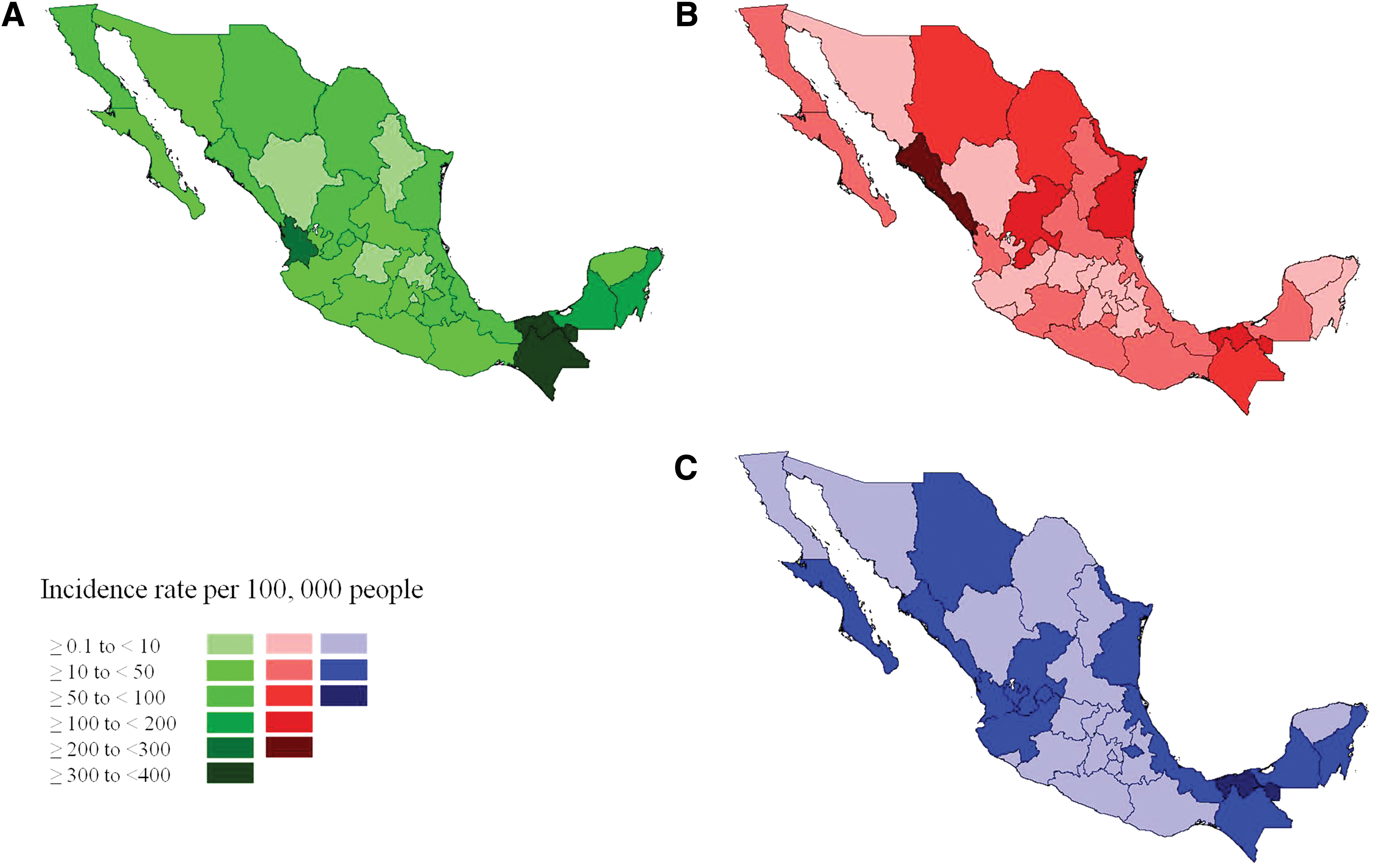
Geographical distribution of Salmonella enterica IR in Mexico.
Focusing on age grouping, people between 44 and 49 years had the highest IR per 100,000 for the three types of illnesses (Fig. 3). The incidence of NTS, Salmonella Typhi, and Salmonella Paratyphi A increased with age, showing the highest peak in the range between 44 and 49 years. These results do not match the information reported for S. enterica by the Centers for Disease Control and Prevention (CDC), in which children <5 years had the highest IR (63 per 100,000 people); whereas the other age groups (>5 years old) had an IR ranging from 10.67 to 18.31 per 100,000 (CDC, 2017a). The discrepancy among the data could be related to the fact that, in Mexico, the etiological agent is often not identified; thus, these clinical cases are included in the “undefined intestinal infection” classification, in which the highest IR is for children <1 year, followed by children between 1 and 4 years (DGE, 2019). The IR for “undefined intestinal infection” for <1-year-old children in comparison with the age group of 44–49 was at least four times higher in the analyzed period. The lack of a diagnosis may underestimate the S. enterica cases. This could be related to the fact that children usually are prescribed with antibiotics without receiving a laboratory-confirmed diagnose, to save time and avoid health complications. The lack of a proper diagnosis could have an important impact on the data interpretation, generating bias.
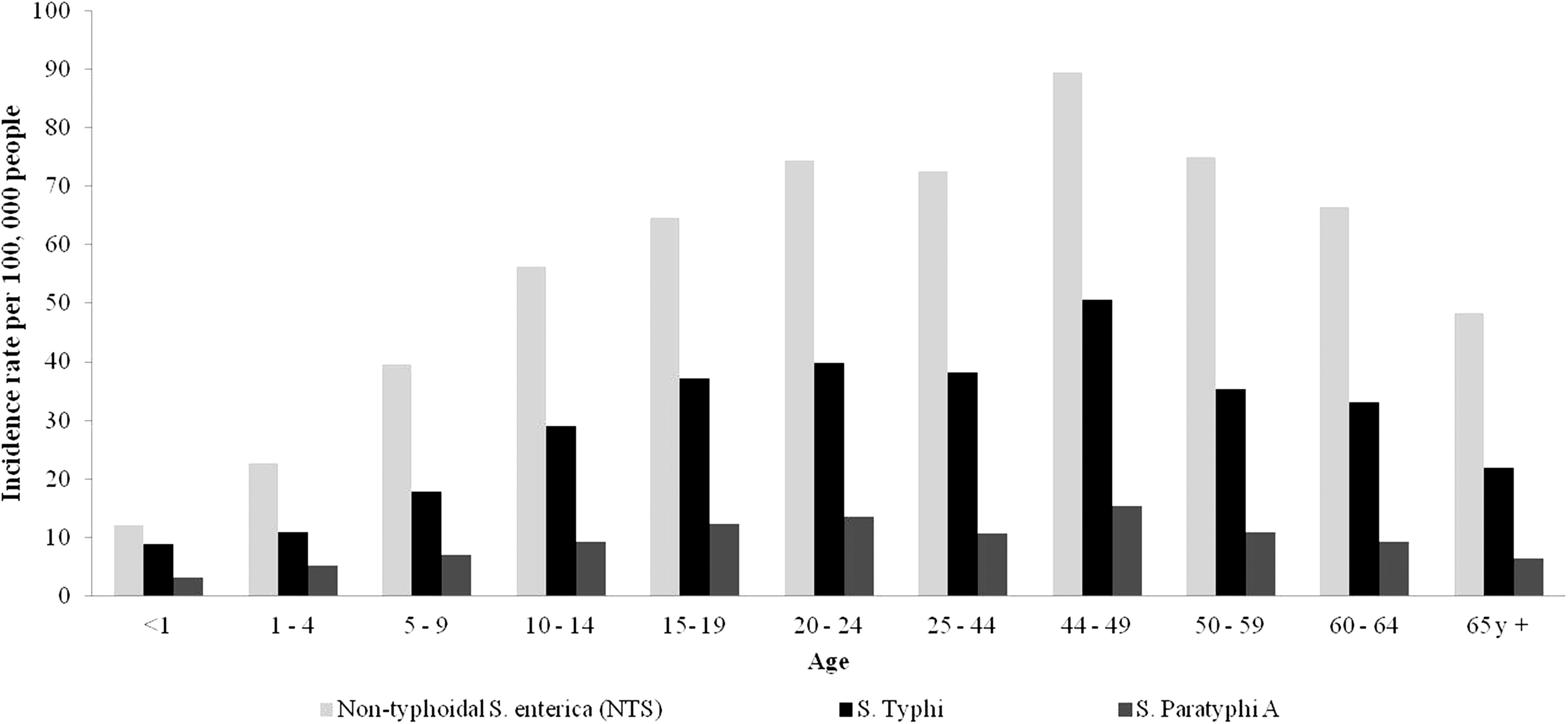
Distribution of the IR of illnesses caused by Salmonella enterica in Mexico by age group. Figure was prepared by using the available information of reported cases by yearbook morbidity of SINAVE. IR, incidence rate; SINAVE, Sistema Nacional de Vigilancia Epidemiológica de Mexico.
According to gender, in all cases, women presented nearly double the number of cases compared with men (Fig. 4). This tendency could be influenced by the fact that women more frequently attend health care units (SS/INSP, 2012).
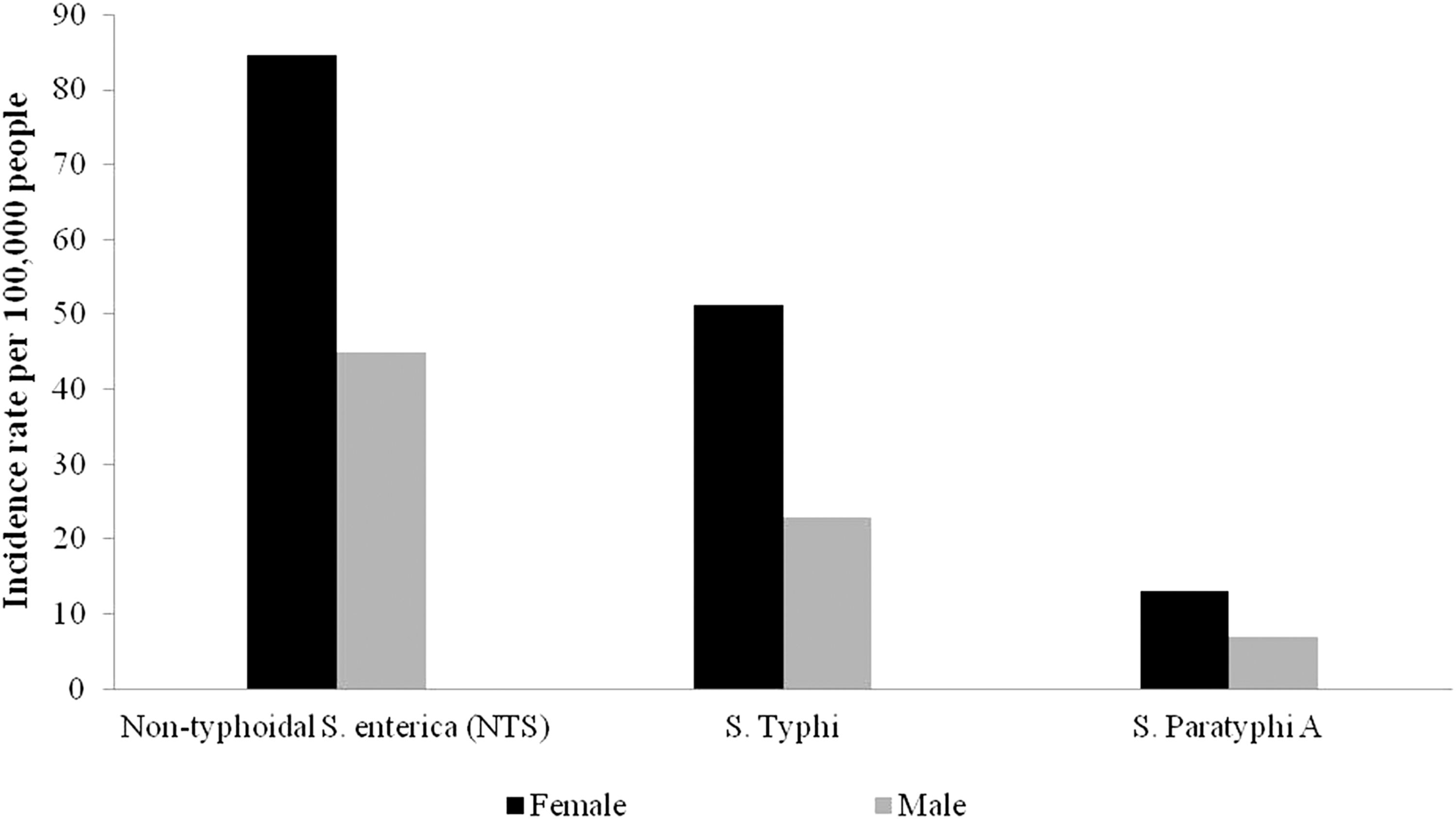
Distribution of the IR of illnesses caused by Salmonella enterica in Mexico by gender. Figure was prepared by using the available information of reported cases by yearbook morbidity of SINAVE. IR, incidence rate; SINAVE, Sistema Nacional de Vigilancia Epidemiológica de Mexico.
On the other hand, S. enterica cases showed a seasonal variation, with a higher number of reported cases in June and a lower number in December (Fig. 5). This tendency coincides with reports of some European countries, Australia, and the United States, where an increase in salmonellosis infections occur in the summer when the environmental temperature is higher (Kovats et al., 2004; Hall et al., 2006; Zhang et al., 2010; CDC, 2016a, 2017a).
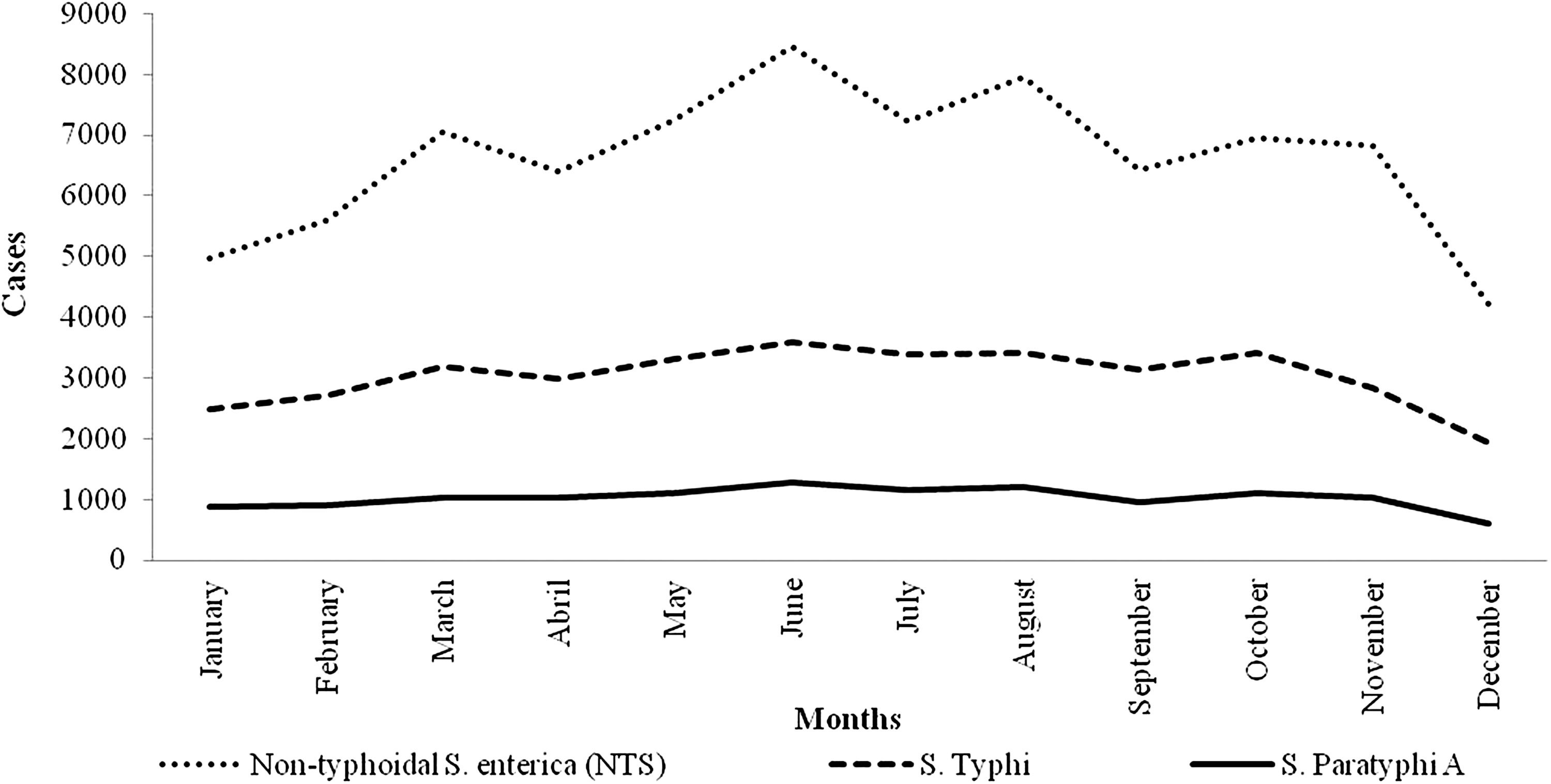
Stationary variation of illnesses caused by Salmonella enterica in Mexico. Figure was prepared by using the available information of reported cases by yearbook morbidity of SINAVE. SINAVE, Sistema Nacional de Vigilancia Epidemiológica de Mexico.
Estimation of S. enterica real cases
It is known that reported data represent only a portion of the true cases. The WHO estimates that between 60% and 80% of NTS cases are not registered as part of an outbreak and either are classified as sporadic cases or are not diagnosed (WHO, 2017). To estimate the true cases, it is necessary to adjust the reported cases by using a multiplication factor. The multiplication factor for underestimated NTS in different countries varies from 0.4 to 2082.9 (Gibbons et al., 2014). In this study, we propose multiplication factors of 49 for NTS, and 23 for Salmonella Typhi and Salmonella Paratyphi A (Table 1). The multiplication factor was calculated by taking into account the underestimation factor and the proportion of foodborne diseases. In Mexico, it is estimated that only 1% of foodborne diseases are reported to the surveillance system (COFEPRIS, 2015) and that there is an underestimation of 1% in the diarrheic diseases (Fernandez-Escartín, 2008). In addition, the WHO estimates that, among people living in the America region B (in which Mexico is included), 49% and 23% of the NTS and Salmonella Typhi cases are attributable to the consumption of contaminated food, respectively (WHO, 2015). In 2017, according to INEGI, 123.5 million people lived in Mexico; using the estimations shown in Table 1, 1 of 27, 1 of 119, and 1 of 431 people in Mexico suffered from NTS, Salmonella Typhi, and Salmonella Paratyphi A linked to the consumption of contaminated food in 2017. These estimations highlight the impact of S. enterica (principally NTS) on the public health of Mexico and the necessity to implement effective control strategies to improve food safety.
Estimation of Foodborne Cases Caused by Nontyphoidal Salmonella enterica, Salmonella Typhi, and Salmonella Paratyphi A in Mexico in 2017
Proportion foodborne cases was taken from America region B in which Mexico is included reported in “WHO estimates of the global burden of foodborne diseases” (WHO, 2015). Proportion foodborne cases for Salmonella Paratyphi used in this estimation was the same as Salmonella Typhi.
Underestimation factor was obtained from COFEPRIS (2015) and Fernandez-Escartín (2008).
NTS, nontyphoidal S. enterica; SINAVE, Sistema Nacional de Vigilancia Epidemiológica de Mexico; WHO, World Health Organization.
Serotypes of S. enterica causing illnesses in Mexico
S. enterica serotypes most frequently isolated from clinical human samples collected from ill people from 1972 to 1999 in Mexico were Salmonella Typhimurium (20.4%), Salmonella Enteritidis (18.3%), Salmonella Typhi (7.1%), Salmonella Agona (5.5%), and Salmonella Newport (5.5%) (Gutiérrez-Cogco et al., 2000).
In a study conducted in the state of Yucatan from 2000 to 2002, S. enterica was detected in 18.7% of stool samples of people who had diarrhea; the serotypes Salmonella Typhimurium (21.8%), Salmonella Agona (21%), and Salmonella Anatum (5.8%) were the most frequently found (Zaidi et al., 2006). In this same state from 2005 to 2011, S. enterica was found in ill children, with an incidence of 13.5%, with the most frequently isolated serotypes being Salmonella Typhimurium (19–21%), Salmonella Agona (9%), Salmonella Muenchen (6–7%), Salmonella Muenster (6–11%), and Salmonella Enteritidis (5–7%) (Zaidi et al., 2013). A similar study conducted in the State of Mexico showed the presence of S. enterica in 56.9% of children's stool samples with diarrhea; the main serotypes identified were Salmonella Ohio (28.6%), Salmonella Typhimurium (16.9%), Salmonella Infantis (10.4%), Salmonella Anatum (0.43%), and Salmonella Newport (0.43%) (Paniagua-Contreras et al., 2008).
From 2002 to 2005, a study was conducted in four states (Sonora, Michoacan, San Luis Potosi, and Yucatan) of Mexico, representing different regions of the country, to determine which S. enterica serotypes were present in stool samples from ill people and asymptomatic children. In that study, we found that the most common serotypes in ill people were Salmonella Typhimurium (22.2%) and Salmonella Enteritidis (14.5%); whereas in asymptomatic children, the most common were Salmonella Agona (8.3%), Salmonella Anatum (8.0%), and Salmonella Typhimurium (6.7%) (Zaidi et al., 2008). According to this information, Salmonella Typhimurium has been the most common serotype in infected and ill people in Mexico for the past five decades.
Prevalence of S. enterica in food samples collected in Mexico
Even though S. enterica illnesses are widely reported in Mexico, it is unfortunately unknown as to which cases are caused by food consumption and, from those, which are linked to outbreaks or sporadic cases. Nonetheless, different studies have been conducted in Mexico to determine the prevalence of S. enterica in food of produce and animal origin (Table 2). Such valuable information could be used to perform a risk assessment of S. enterica in food consumed in Mexico. It is important to mention that the Mexican legislation of food items for human consumption requires the absence of S. enterica. In NOM-210-SSA1-2014, the protocol to detect this pathogen in food items is specified, which is harmonized with the international norm ISO 6579 (DOF, 2015).
Prevalence of Salmonella enterica spp. in Different Types of Food Collected in Mexico
NS, not specified.
Fresh fruits and vegetables have been the most studied food items. The presence of this pathogen has been assessed in Coahuila, Hidalgo, Jalisco, Mexico City, Nayarit, Nuevo Leon, and Queretaro (Castillo et al., 2006; Gallegos-Robles et al., 2008, 2009; Quiroz-Santiago et al., 2009; Ragazzo-Sanchez et al., 2009; Castro-Rosas et al., 2010, 2011; Cardenas et al., 2013; Ávila-Vega et al., 2014; Leal-Cervantes et al., 2018). S. enterica was found in vegetables, such as potatoes (1%) (Quiroz-Santiago et al., 2009), Bola tomato (2.5%) (Cardenas et al., 2013), bell pepper (3%) (Ávila-Vega et al., 2014), celery (3%), Romaine lettuce (3%), beet (4%), Chinese parsley (6%), large lettuce (7%), watercress (7%), spinach (7%), broccoli (9%), cauliflower (9%), Purslane (9%) (Quiroz-Santiago et al., 2009), zucchini squash (10%) (Castro-Rosas et al., 2010), Serrano peppers (10%) (Castro-Rosas et al., 2011), coriander (11%) (Quiroz-Santiago et al., 2009), cherry tomatoes (11.17%) (Leal-Cervantes et al., 2018), and jalapeño pepper (2.5% and 12%) (Castro-Rosas et al., 2011). For fruits, there are fewer published studies. S. enterica was detected in mango (6.7%) (Ragazzo-Sanchez et al., 2009), orange (13.3%) (Castillo et al., 2006), and cantaloupe (40% and 45%) (Gallegos-Robles et al., 2008, 2009). Interestingly, cantaloupe melons show the highest S. enterica prevalence, and the exported products have also been linked to outbreaks in the United States (CDC, 2002).
The prevalence of S. enterica has also been evaluated in semiprocessed fruits and vegetables. The pathogen was detected in beet juice (4%) (Gómez-Aldapa et al., 2014), cooked ready-to-eat salads (4.1%) (Bautista-De León et al., 2013), raw salads (6.8%) (Gómez-Aldapa et al., 2013a), carrot juice (8.6%) (Torres-Vitela et al., 2013), and orange juice (9%) (Castillo et al., 2006). These data indicate that the prevalence of the pathogen is similar between fresh produce and semiprocessed products. The similar prevalence of S. enterica could be related to poor hygienic practice during the preparation of these products such as lack of washing and disinfection treatments, or the inappropriate use of utensils that cause cross-contamination (Gil et al., 2009; Carrasco et al., 2012).
In general, Salmonella Typhimurium (39%) is the serotype with the highest frequency in fruits and vegetables (Fig. 6A).
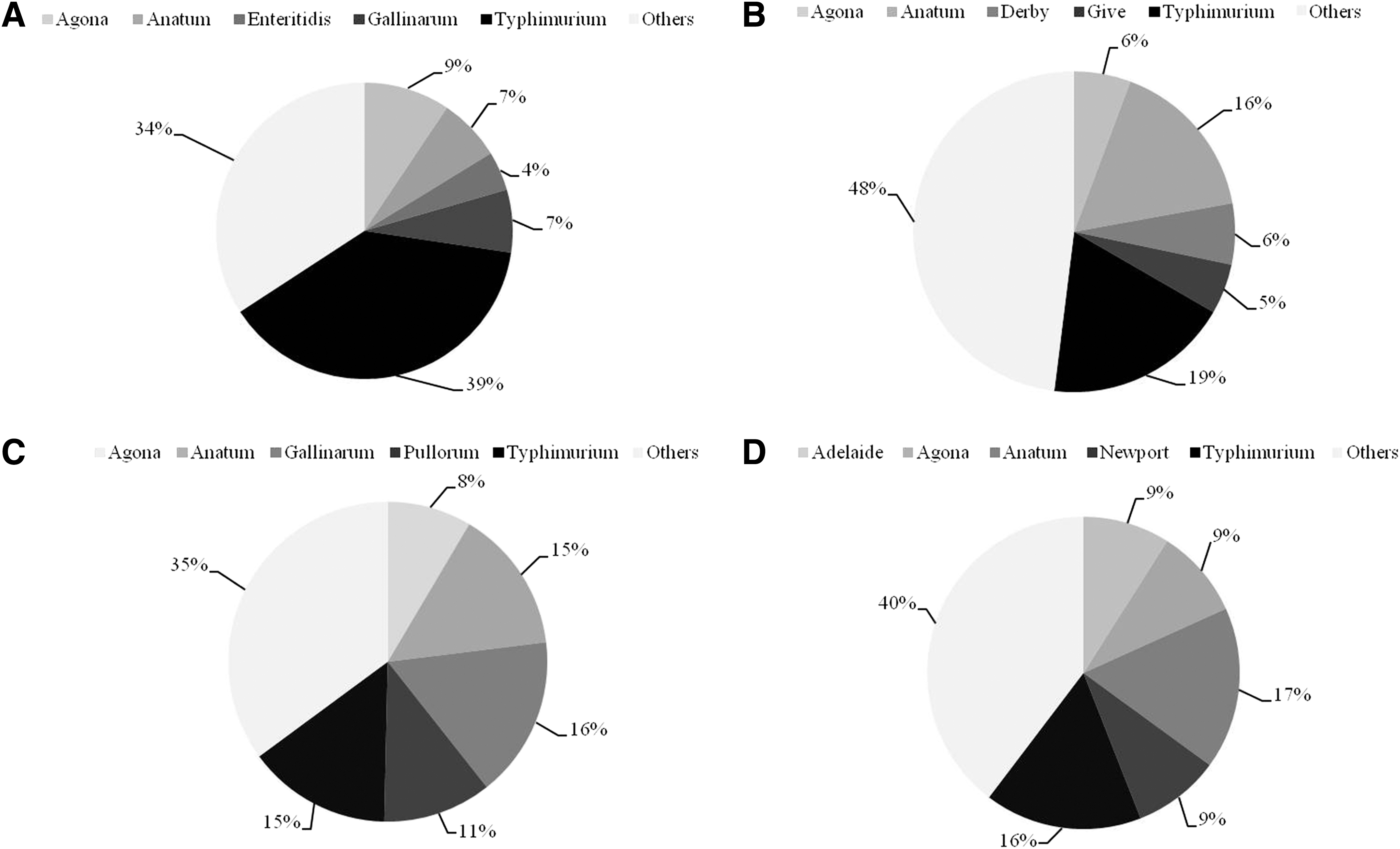
Frequency of the top five Salmonella enterica serotypes in food items.
The prevalence of S. enterica is more heterogeneous and higher in raw meats. The presence of this pathogen has been investigated in Mexico City, Hidalgo, Jalisco, and Yucatan. The results showed that S. enterica prevalence ranged from 6.1% to 54% in beef (Heredia et al., 2001; Zaidi et al., 2006; Miranda et al., 2009; Perez-Montaño et al., 2012; Cabrera-Diaz et al., 2013; Nayarit-Ballesteros et al., 2016; Pond et al., 2016; Villalpando-Guzmán et al., 2017), from 4.5% to 63.2% in chicken (Zaidi et al., 2006; Charles-Hernández et al., 2007; Miranda et al., 2009; Rodríguez-Ceniceros et al., 2016; Villalpando-Guzmán et al., 2017), and from 13.3% to 58.1% in pork (Zaidi et al., 2006; Miranda et al., 2009; Pond et al., 2016; Villalpando-Guzmán et al., 2017).
The top five most frequently isolated S. enterica serotypes from raw meat are shown in Figure 6B–D. Serotypes Typhimurium (19%) and Anatum (16%) were the most frequently found from beef; serotypes Gallinarum (16%), Anatum (15%), and Typhimurium (16%) were the most frequently found in chicken; and Salmonella Anatum and Salmonella Typhimurium were detected in 16% and 17% from pork samples, respectively. Salmonella Gallinarum and Salmonella Pullorum were only detected from chicken samples until 2010, because from August 2012, the Mexican territory was declared free from avian salmonellosis (Salmonella Gallinarum and Salmonella Pullorum) (DOF, 2012); these two serotypes could cause fowl typhoid and pullorum disease (Shivaprasad, 2000). In addition, serotypes Give, Havana, and Infantis were related exclusively to beef (Fig. 7).
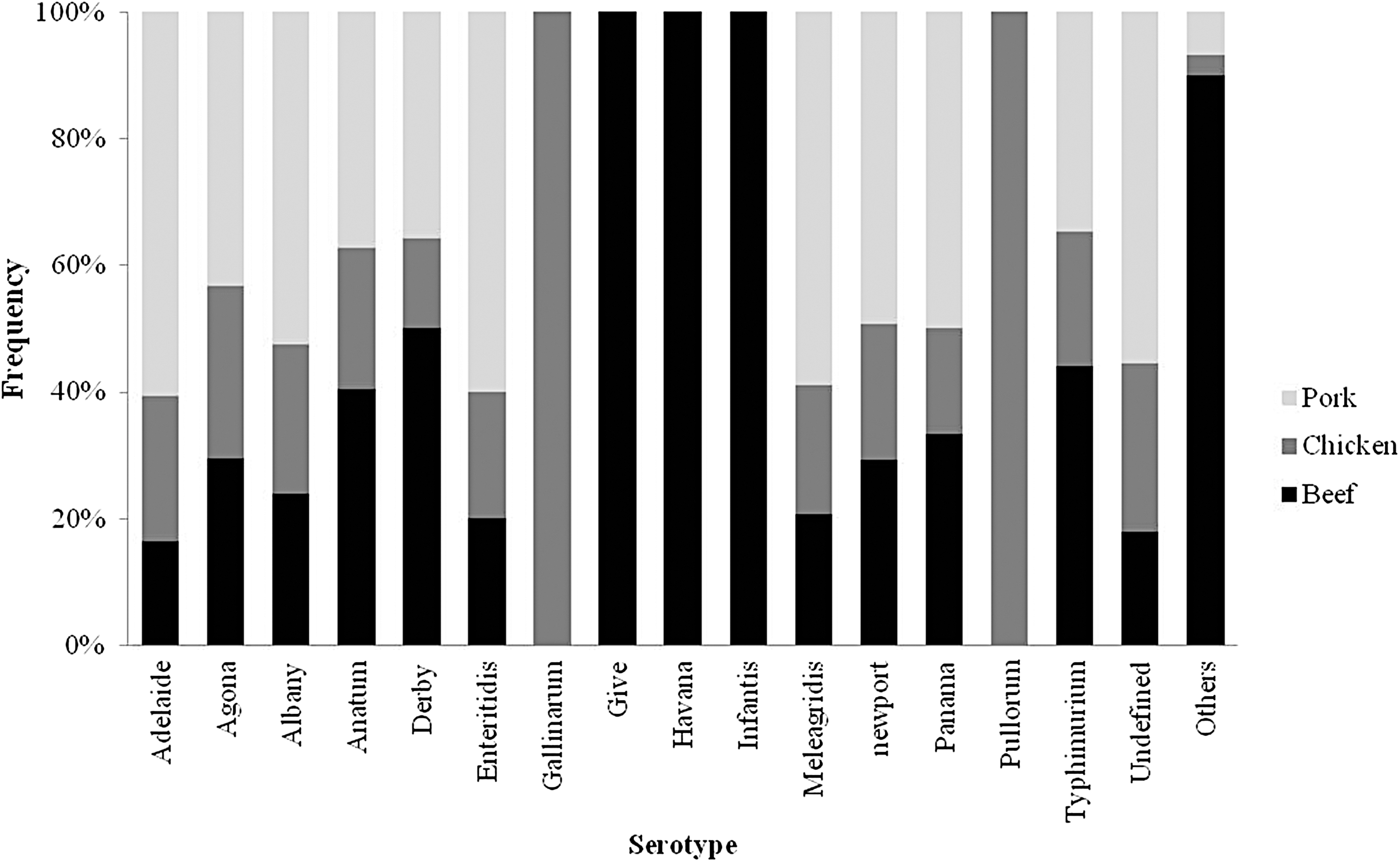
Frequency of Salmonella enterica serotypes in raw meat. Figure was prepared by using the information of published articles (Castillo et al., 2006; Zaidi et al., 2006; Gallegos-Robles et al., 2008, 2009; Quiroz-Santiago et al., 2009; Perez-Montaño et al., 2012; Cabrera-Diaz et al., 2013; Rangel-Vargas et al., 2015; Nayarit-Ballesteros et al., 2016: Villalpando-Guzmán et al., 2017).
In the case of processed meat products, the prevalence of S. enterica in chorizo (traditional Mexican stuffed meat sausage) and longaniza (traditional Mexican cured sausage) was 36% and 48%, respectively, in Jalisco state (Torres-Vitela et al., 2011) (Table 2). S. enterica serotype Derby (30%) and Adelaide (17%) were the most frequently isolated from processed meat products. The high prevalence of S. enterica in processed meat products could be related to the main raw material that was used to produce them as well as the unsafe handling practices that can generate a cross-contamination at plants and/or retail points (Reij et al., 2004; Pérez-Rodríguez et al., 2010).
In eggs, the prevalence of S. enterica is low (0.25–3%) (Table 2). These results are similar to those reported in developed countries, such as the United Kingdom and Ireland (Murchie et al., 2007; Little et al., 2008). However, in other countries with similar socioeconomic situations such as India and Uruguay, S. enterica prevalence in eggs ranged from 5.5% to 9.4% (Suresh et al., 2006; Betancor et al., 2010; Singh et al., 2010).
In the case of dairy products, studies carried out in the states of Jalisco and Hidalgo showed the presence of the pathogen in fresh cheese (1.1–34%) (Charles-Hernández et al., 2007; Miranda et al., 2009; Torres-Vitela et al., 2012). Only one study characterized the isolated strains, finding that Salmonella Amsterdam (22.5%) and Salmonella Anatum (16.9%) were the most frequent (Torres-Vitela et al., 2012). The high prevalence of S. enterica found in fresh Mexican cheese could be related to the common practice of using nonpasteurized milk for its production or to the absence of good manufacturing practices during processing (Cody et al., 1999; Oliver et al., 2005; Vargas et al., 2007; Torres-Vitela et al., 2012).
In seafood collected in fishing zones (the States of Veracruz and Campeche), such as octopus and raw clams, S. enterica was found in 11.7% and 11.0% of the tested samples, respectively (Quiñones-Ramírez et al., 2000; Estrella-Gómez et al., 2016). As for raw fish, only two studies were found to be showing a prevalence of 0% and 0.7% (Charles-Hernández et al., 2007; Miranda et al., 2009). Finally, in a sampling of raw and frozen shrimp designated for exportation, the pathogen was not detected (Casas et al., 2005).
Antimicrobial resistance of S. enterica isolates from human cases and food in Mexico
The presence of antimicrobial resistant (AMR) microorganisms has recently been prioritized in the world due to its great risk to human health (WHO, 2014, 2017; Ventola, 2015; Ferri et al., 2017).
Table 3 shows the percentages of antimicrobial resistance to S. enterica isolated strains from human cases and food. In all studies, the antimicrobial susceptibility was determined by using the disk diffusion method, except for the study done by Miranda et al. (2009), where the microdilution method was used. In Mexico, a higher number of S. enterica isolates had resistance to streptomycin, tetracycline, ampicillin, and chloramphenicol. The same trend was observed in the United States during the period 2004–2013, where a higher number of NTS isolates showed resistance to antibiotics mentioned earlier and also sulfamethoxazole/trimethoprim (Michael and Schwarz, 2016).
Percentage of Salmonella enterica Strains Resistant to Antimicrobials Isolated from Humans and Food in Mexico
Reported data were obtained by the disk diffusion method with the exception of those from Miranda et al. (2009) in which the microdilution method was used. Data were collected and interpreted according to CLSI criteria.
Includes resistant and intermediate strains.
AK, amikacin; AMP, ampicilin; AZT, azithromycin; CAZ, ceftazidime; CB, carbenzillin; CEP, cephalotin; CFX, cefoxitin; CHL, chloramphenicol; CIP, ciprofloxacin; CLSI, Clinical and Laboratory Standards Institute; CRO, ceftriaxona; CTX, cefotaxime; FZD, furazolidone; GEN, gentamicin; KAN, kanamycin; NAL, nalidixic acid; NET, netilmicin; NFT, nitrofurantoin; NR, not realized; NS, not specified; PEF, perfloxacin; STR, streptomycin; SU, sulfisoxazole; SXT, trimetoprim/sulfamethoxazole; TET, tetracycline.
Multidrug-resistant (MDR) strains, resistant to three or more antimicrobials of at least three different antimicrobial categories (Magiorakos et al., 2011), dramatically affect the efficiency of antimicrobial therapy in humans; hence, the illness can last longer and the severity increases (WHO, 2014). Studies have revealed that antimicrobial MDR Salmonella Typhimurium strains have been associated with a risk of a massive infection, major infection frequency, longer hospitalization periods, and increased death risk as compared with infections caused by susceptible strains (Gupta et al., 2003; Helms et al., 2005; Gordon et al., 2008; Leekitcharoenphon et al., 2016).
Lack of information and gaps in surveillance system hinder the development of control measures for detection of S. enterica MDR strains in Mexico. Additional problems could be observed in the lack of data harmonization among the published information: (1) AMR percentage of each antibiotic is the only reported one; (2) isolates are not serotyped; (3) MDR profiles are not reported; and (4) MDR profiles are not specified by the origin of isolates. Despite this, some groups have evaluated MDR in S. enterica isolated from contaminated food and infected people in Mexico. However, the studies cover a few states of the country (Mexico City, Hidalgo, Jalisco, Mexico State, Michoacán, San Luis Potosi, Sonora, and Yucatan).
Zaidi et al. (2006) evaluated the relationship between S. enterica serotypes and MDR profiles of strains isolated from ill people, asymptomatic children, chicken, pork, and beef, finding that Salmonella Anatum (68%) and Salmonella Typhimurium (52%) isolates were the serotypes with the highest rates of MDR. Notably, most of the Salmonella Typhimurium isolates evaluated in the study came from patients with diarrhea. A similar result was found in a study conducted by Aguilar-Montes de Oca et al. (2017), who tested isolates from ground beef, swine, bovine, poultry, and clinical cases; 6.6% of the isolates had MDR; and from all MDR S. enterica isolates, the 56.3% corresponded to Salmonella Typhimurium isolates.
Among different food items, Miranda et al. (2009) found that isolates showing MDR profiles were obtained from meat, such as poultry (100%), pork (85.4%), and beef (63.7%), cheese (60%), and vegetables (47.1%).
In Mexico, the majority of reports in which the MDR profiles of S. enterica were investigated were performed in beef. In a study conducted in Jalisco, 33.3% (26/78) of the S. enterica strains isolated from beef carcasses were MDR. Of the strains showing MDR, 50% (13/26) were serotyped as Salmonella Typhimurium, which represents 92.9% (13/14) of isolates belonging to this serotype (Perez-Montaño et al., 2012). In ground beef, S. enterica isolates have shown MDR profiles ranging from 27.4% (37/135) to 73.7% (14/19). The serotypes that showed most MDR in ground beef were Salmonella Anatum (92.9%), Salmonella Typhimurium (62.5%), Salmonella Lomita (42.9%), and Salmonella Derby (10.8% and 7.1%) (Cabrera-Diaz et al., 2013; Nayarit-Ballesteros et al., 2016).
The high presence of MDR profiles among isolates from animal food products could be related to the frequent exposition of the animals to antimicrobials (Doyle, 2015; Economou and Gouisa, 2015; Gebreyes et al., 2017). According to the Mexican norm “NOM-040-ZOO-1995,” some of the antibiotics to which S. enterica is resistant can be used in animals, such as streptomycin, gentamicin, amikacin, tetracycline, trimethoprim, sulfametoxazol, chloramphenicol, nalidixic acid, and others (DOF, 1996).
It is complicated to establish whether predominant S. enterica clones with a particular MDR profile are circulating in food or humans in Mexico. This can be related to a lack of studies and the absence of harmonized protocols. Worldwide, some S. enterica strains with MDR profiles are considered more important, because they cause a higher number of cases of illness than the susceptible strains; for example, ASSuT (ampicillin, streptomycin, sulfonamides, and tetracycline) and ACSSuT (ampicillin, chloramphenicol, streptomycin, sulfonamides, and tetracycline) (Lucarelli et al., 2010; Michael and Schwarz2016). In Mexico, in spite of the limitations and low territorial coverage from the studies that recovered S. enterica isolates, the phenotypes ACSSuT and ASSuT were obtained from food and human clinical samples. From the available data in Mexico, the ACSSuT phenotype was found in humans, poultry, and pork isolates; whereas ASSuT was found in beef isolates (Table 4). In vegetables and cheese, none of these profiles was found.
Salmonella enterica Isolates from Humans and Food with Common Multidrug-Resistant Profile
ACSSuT, ampicillin, chloramphenicol, streptomycin, sulfonamides, and tetracycline; ASSuT, ampicillin, streptomycin, sulfonamides, and tetracycline; MDR, multidrug-resistant.
Mexican products linked to S. enterica food outbreaks
Fruits and vegetables are the exported Mexican products that have been linked to outbreaks in the United States (Table 5). From 2000 to 2002, three multistate outbreaks caused by Salmonella Poona were linked to the consumption of cantaloupe melons from Mexico, in which 158 patients were infected, 28 were hospitalized, and 2 died (CDC, 2002). In 2008, an outbreak of Salmonella Saintpaul was linked to the consumption of food in a Mexican restaurant; the related foods were pico de gallo (raw onions, tomatoes, and peppers), salsa, and tortillas. Salmonella Saintpaul was isolated from jalapeño peppers that were collected in Texas and on Serrano peppers grown in Mexico. In the outbreak, 1499 patients were infected and 2 died (Barton Behravesh et al., 2011). In 2012, an outbreak caused by S. Braenderup affected various states in the United States; it was linked to the ingestion of mangoes imported from Mexico, all of which were packaged in the state of Sinaloa, Mexico. The outbreak caused 106 infections and the hospitalization of 33 people (CDC, 2013a; FDA, 2013).
Salmonella enterica Outbreaks in the United States Linked to Imported Mexican Fresh Produce
Not specified the state.
NS, not specified.
Mexican papayas and cucumbers are products that have been frequently associated to outbreaks of S. enterica. In 2013, an outbreak of Salmonella Saintpaul was linked to the consumption of contaminated cucumbers grown in Culiacan, Sinaloa, Mexico (CDC, 2013b). In 2016, an outbreak related to the same product occurred, this time linked to a grower from Baja California, and Salmonella Poona was the identified serotype (CDC, 2016b; FDA, 2016). This outbreak caused the highest health damage among all outbreaks linked to imported Mexican food, with 907 infected people, 204 hospitalizations, and 6 deaths.
In the case of papayas, the Maradol variety was involved in the 2011 outbreak of Salmonella Agona linked to whole fresh papayas being imported from Mexico (CDC, 2011); later in 2017, a multistate outbreak was linked to the consumption of Maradol papayas imported from different Mexican regions (Colima, Baja California, Campeche, Jalisco) (FDA, 2017). Several S. enterica serotypes (Salmonella Newport, Salmonella Infantis, Salmonella Anatum, Salmonella Thompson, Salmonella Kiambu, Salmonella Agona, Salmonella Gaminara, Salmonella Senftenberg, and Salmonella Urbana) were detected in stools from patients, and most were also detected in papayas imported from Campeche (CDC, 2017d).
At a worldwide level, Mexico ranks second in the production of peppers, third in the production of melons, fifth in the production of mangoes and papayas, and ninth in the production of cucumbers (SIAP, 2017). Mexico is the main market provider of produce to the Unites States; this could be related with the number of foodborne outbreaks associated to fruits and vegetables imported from Mexico. In the past decade, the Mexican Federal Government has been working on the development and implementation of food safety programs to avoid foodborne pathogen contamination of fresh produce during pre- and postharvest (SENASICA, 2019).
Conclusions
As expected, the epidemiological analysis of the available data in Mexico (2000–2017) confirmed that S. enterica is a foodborne pathogen of major concern. There is a possible relationship between less favorable socioeconomic states of Mexico (Chiapas and Tabasco) and the highest IR of NTS. The lack of clinical diagnostics precludes the establishment of a trustable tendency among age groups.
Although there is a scarcity of information, analysis of the available studies of the prevalence of S. enterica in food showed that fresh meat (pork, chicken, and beef) and meat products (chorizo and longaniza) are the food items of major concern due to the high prevalence of the pathogen and the presence of isolates with MDR profiles. Salmonella Typhimurium is the serotype most frequently isolated from human and food items, showing the highest percentages of MDR profiles. Information presented in this review highlights the need to implement effective surveillance and control strategies to improve food safety that could eventually impact the number of illnesses caused by S. enterica in Mexico.
Finally, in 2017, the calculated estimations for illnesses caused by NTS (4,508,537), Salmonella Typhi (1,041,440), and Salmonella Paratyphi A (286,534) linked to the consumption of contaminated food provide evidence for the impact of S. enterica on the public health of Mexico.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
No funding was received for this article.