
Abstract
In the field of the detection of pathogens responsible for infectious diarrhea, multiplex nucleic acids detection technology has attracted attention due to its ability to simultaneously screen a wide range of pathogens, its simplicity to operate and a faster turnaround time. We conducted a three-center evaluation that compared the BioFire FilmArray gastrointestinal panel (FA GI) and real-time polymerase chain reaction (PCR) assays for the detection of pathogens from 462 clinical diarrhea specimens, and characterized the distribution of various pathogens that were analyzed. The sensitivity of FA GI was 100% for 13 pathogens and 93.8–98.3% for 4 pathogens, but low for Salmonella (60.5%) and adenovirus (88.9%). The sensitivity per pathogen of real-time PCR assays was lower than that observed with FA GI. The specificity of FA GI and real-time PCR assays per pathogen was greater than 94.5% and 99%, respectively. FA GI and real-time PCR assays detected ≥1 pathogen in 339 (73.4%) and 297 (64.3%) samples, respectively, and 324 (70.1%) samples were considered as positive according to the reference standard. Multiple pathogens were detected in 37.2% and 24.9% of samples by FA GI and real-time PCR assays, respectively. Norovirus GI/GII and Campylobacter were less associated with coinfections. The positive rates of some pathogens varied among the three regions of China. Molecular methods can help squickly identify the cause of diarrhea and provide valuable information for early diagnosis and optimal patient therapy.
Introduction
Globally, diarrheal disease is a leading cause of childhood morbidity and mortality and is one of the main causes of malnutrition in children younger than 5 years of age. Bacteria, viruses, or parasites can all cause infectious diarrhea (Hatchette and Farina, 2011). The actual cause of infectious diarrhea often cannot be distinguished by symptoms alone. Therefore, rapid and accurate identification of diarrhea pathogens is of great significance for timely treatment and to initiate prompt measures to control the spread of infection.
Traditional detection methods such as bacterial or viral culture, microscopy, or immunological methods are time-consuming, labor-intensive, and require experienced laboratory staff. Laboratories performing traditional testing generally target only a few common pathogens. Today, highly multiplexed molecular assays to detect gastrointestinal (GI) pathogens are available with some assays having the advantages of simple operation, a rapid turnaround time, and a wide range of pathogen coverage. One of these methods, the BioFire FilmArray GI panel (FA GI; BioFire Diagnostics, a bioMérieux Company, Salt Lake City, UT) simultaneously tests for 22 pathogens from stool specimens, greatly simplifies the detection process and expands the detection range over traditional laboratory methods. In the present study, we conducted a three-center evaluation that compared the FA GI, singleplex real-time polymerase chain reaction (PCR) assays, and culture methods for the detection of GI pathogens from clinical specimens.
Materials and Methods
Clinical stool specimens
From January to September 2016, 462 fecal specimens were collected at Wuxi City in Jiangsu Province, Changning District in Shanghai Municipality, Longshan County and Xinhuang County in Hunan Province. For the patients with diarrhea who visited the sentinel hospitals, the stool specimens were collected by the clinical laboratories and sent to the laboratories in local Centers for Disease Control and Prevention (CDC) for testing. In Hunan, all diarrhea specimens collected from both sentinel hospitals were included; in Wuxi and Changning, the specimens used for the tests were collected from the first 15–20 diarrhea patients going to the sentinel hospitals each month. Demographic and clinical data, including each patient's age, gender, and symptoms, were collected.
Sample processing
Approximately 1 g of stool specimen was added to 10 mL of Cary-Blair transport medium and stored at 4°C for <48 h before delivery to the CDC laboratories. Upon specimen receipt, the laboratory performed culture for Salmonella and Vibrio. In the majority of cases, the FA GI and Nucleic Acid (NA) test could not be completed on the day of sample receipt, in which specimens were frozen at −80°C until subsequent testing by the FA GI and NA extraction.
A total of 24 retrospective specimens stored at −80°C (without transport medium or other liquids) were included in the study. After the specimens were thawed at room temperature, 10 mL of 0.9% NaCl was added to 1 g or 1 mL of the specimen, which was mixed thoroughly and processed for both FA GI and NA extraction for singleplex PCR.
The number of freeze–thaw cycles for all samples was <3. The remaining specimens and the purified NAs were stored at −80°C. NAs were delivered on dry ice to the China CDC laboratory where they were tested with singleplex PCR assays within 2 months.
FA GI testing
Pathogens detected by FA GI are listed in Table 1. A 200 μL aliquot of specimen suspension in Cary-Blair medium (for prospective specimens) or saline (for retrospective specimens) was tested by FA GI according to the manufacturer's instructions. FA GI testing and NA extraction of specimens were always performed on the same day.
Pathogens Detected and Genes Targeted by Comparator Real-Time Polymerase Chain Reaction and the Polymerase Chain Reaction Used for Discordance Resolution
Luminex xTAG Gastrointestinal Pathogen Panel (xTAG GPP).
EAEC, enteroaggregative E. coli; EPEC, enteropathogenic E. coli; ETEC, enterotoxigenic E. coli; GI, gastrointestinal; STEC, Shiga toxin-producing E. col.
Comparator methods
At Wuxi CDC, NAs were extracted from 200 μL of the Cary-Blair supernatant using the MagNA Pure LC Total Nucleic Acid Isolation Kit on the MagNA Pure LC 2.0 instrument (Roche, Indianapolis, IN) and eluted with 50 μL of elution buffer. At Changning CDC, NAs were extracted from 300 μL of the Cary-Blair supernatant using a cador Pathogen 96 QIAcube HT Kit on the QIAcube HT instrument (Qiagen, Hilden, Germany) and eluted with 150 μL of elution buffer. In Hunan CDC, NAs were extracted from 200 μL of the Cary-Blair supernatant using a EX-DNA/RNA virus extraction kit using the automatic purification system NP968 (Tianlong, Xi'an, China) and eluted in a final volume of 100 μL. The extracted NAs were tested by real-time PCR or real-time reverse transcriptional PCR (RT-PCR). The pathogens detected are listed in Table 1.
For viral pathogens, singleplex real-time RT-PCR assays were performed with a PrimerScript One Step RT-PCR Kit (perfect Real Time; TaKaRa, Dalian, China). Vibrio cholerae, Vibrio parahaemolyticus, and Salmonella were detected by TaqMan real-time PCR assays with Premix Ex Taq (Probe qPCR [quantitative PCR]; TaKaRa). Other targets were detected by SYBR real-time PCR assays with SYBR Premix Ex Taq (TaKaRa). All detections were performed in 20 μL reaction mixtures, including 1 μL of extracted NAs, 0.4 μL of forward primer (10 μM) and reverse primer (10 μM), and 0.4 μL of probe (10 μM) if applicable. The cycling conditions were as follows: (1) real-time RT-PCR: 42°C for 5 min, 95°C for 10 s; 95°C for 5 s, 60°C for 40 s, for 40 cycles. (2) real-time PCR: 95°C for 30 s; 95°C for 5 s, 60°C for 40 s, for 40 cycles; melt curves were analyzed in SYBR real-time PCR. Real-time PCR was performed in a LightCycler 96 system (Roche).
Traditional culture was performed for Salmonella and Vibrio with the following media: Selenite Brilliant Green (SBG) Broth (Luqiao, Beijing, China), Salmonella Chromogenic Medium (Kemajia, Shanghai, China), Alkaline Peptone Water (APW; Luqiao), and thiosulfate-citrate-bile-sucrose (TCBS; Oxoid, Basingstoke, England, United Kingdom) agar. Suspicious colonies were selected and identified using serum agglutination tests and systematic biochemical reactions with VITEK 2 Gram-negative identification cards (bioMérieux France).
Discordant analysis
To investigate any discordance between FA GI and real-time PCR results, a third method was used as shown in Table 1. Samples showing discordant results for norovirus GI/GII and rotavirus A were tested with a Luminex xTAG (Luminex, Austin, TX) gastrointestinal pathogen panel according to the manufacturer's instructions.
Reference standard
A reference standard positive sample was defined as a sample with (1) an organism identified by culture when applicable or (2) a “consensus positive,” in which an organism was detected by both FA GI and real-time PCR or (3) an organism detected by two or three of the molecular assays after discordant analysis.
A reference standard negative sample was defined as a sample with (1) a “consensus negative,” in which an organism was not detected by FA GI, real-time PCR or culture, when applicable or (2) an organism was not detected by two or three of the molecular assays, and the culture result was also negative.
Escherichia coli O157 and Cyclospora cayetanensis were not tested by real-time PCR assays, and the results of FA GI were considered true positive (TP) or true negative (TN).
Calculations and statistical analysis
Based on the reference standard described, the sensitivities and specificities per pathogen were calculated for each method. Sensitivity = (TP/[TP + FN, False Negative]) and specificity = (TN/[TN + FP]). The exact binomial two-sided 95% confidence interval (95% CI) was calculated according to the method of Wilson/Brown using GraphPad Prism 7. FA GI and real-time PCR were compared by percent positive agreement (PPA) and percent negative agreement (PNA). The positivity rate of each pathogen was compared among three sites using the chi-squared test or Fisher exact test at α = 0.05. Statistical analyses were performed using SPSS (ver. 23; IBM Analytics, Armonk, NY).
Results
Specimen basic information
Stool specimens were collected from January 2016 to September 2016; 160 from Changing District, 152 from Wuxi, and 126 from Hunan. In addition, 24 specimens collected before December 2015 in Hunan were tested in the study. In total 462 specimens were analyzed during this evaluation. The patients included 234 males and 228 females, of which 92 (19.9%) were <1 year-old and 70 (15.1%) were 1–5 years old.
Performance of FA GI and real-time PCR
The specimens of Hunan included 24 retrospective specimens. The positive rate of retrospective specimens in the FA GI test was 83.3%. The positive rate of most major pathogens was close to that of nonpreserved specimens in Hunan, such as norovirus (29.2% vs. 21.4%) and enteropathogenic E. coli (EPEC; 33.3% vs. 31.0%). Therefore, all Hunan specimens were analyzed together.
The concordance between FA GI and real-time PCR by pathogen is shown in Table 2. When compared to real-time PCR, FA GI showed a high level of PPA and PNA for each pathogen (>95%), with the exception of adenovirus (PPA = 80.0%), Salmonella spp. (PPA = 90.0%), enteroaggregative E. coli (EAEC; PNA = 93.6%), and EPEC (PNA = 93.7%). The overall concordance between these two methods was >95% except for EAEC (93.9%) and EPEC (94.2%).
Performance of FilmArray Gastrointestinal Panel and Real-Time Polymerase Chain Reaction Results
Including 10 positive and 8 negative in culture of Salmonella.
The specimens were positive by culture methods.
Including two positive and one negative in culture of V. cholera.
Including nine positive and four negative in culture of V. parahaemolyticus.
95% CI, 95% confidence interval; EAEC, enteroaggregative Escherichia coli; EIEC, enteroinvasive E. coli; EPEC, enteropathogenic E. coli; ETEC, enterotoxigenic E. coli; FA GI, FilmArray gastrointestinal panel; PCR, polymerase chain reaction; PNA, percent negative agreement; PPA, percent positive agreement; Sen, sensitivity; Spe, specificity; STEC, Shiga toxin-producing E. coli; /: not applicable.
The overall sensitivity and specificity of the FA GI were 95.6% (95% CI: 93.5–97.1) compared to 88.4% (95% CI: 85.4–90.9) for real-time PCR and 98.4% (95% CI: 98.1–98.7) compared to 99.9% (95% CI: 99.8–99.9) for real-time PCR, respectively.
FA GI demonstrated a sensitivity of 100% for 13 pathogens (Table 2). The sensitivity was 93.8–98.3% for norovirus GI/GII, rotavirus A, EPEC, and Campylobacter, and lower for Salmonella spp. (60.5%) and adenovirus (88.9%). The specificity of FA GI per pathogen was >94.5% for all the targeted pathogens.
The sensitivity per pathogen of the real-time PCR was lower than FA GI for most of the targets: 47.4% (18/38) for Salmonella spp.; 60–70% for astrovirus, sapovirus, EAEC, and V. cholerae; 80–90% for Shiga toxin-producing E. coli (STEC), Campylobacter spp., and V. parahaemolyticus; 90–99% for norovirus GI/GII and EPEC; and 100% for the other nine pathogens. The specificity per pathogen of the real-time PCR was >99%.
The performance of the FA GI and the real-time PCR for the detection of Yersinia enterocolitica, E. coli O157, and C. cayetanensis were not evaluated, as E. coli O157 and C. cayetanensis were not detected by comparator methods, and Y. enterocolitica was not detected by both assays.
Spectrum of pathogens detected
For all pathogens, FA GI showed higher or equal detection rates than real-time PCR. FA GI detected one or more pathogens in 339 (73.4%) samples, real-time PCR detected pathogens in 297 (64.3%) samples, and 324 (70.1%) samples were verified as positive for one or more pathogens, according to the reference standard (Table 3). EPEC was the pathogen most frequently detected (20.8%), followed by norovirus GI/GII (15.8%), rotavirus A (13.0%), EAEC (8.9%), enterotoxigenic E. coli (8.9%), Clostridium difficile (8.7%), Campylobacter spp. (7.8%), and Salmonella spp. (8.2%).
The Positive Detection Rates of Samples and Percentage of Co-Infections
The detection results verified according to the reference standard.
EAEC, enteroaggregative E. coli; EPEC, enteropathogenic E. coli; ETEC, enterotoxigenic E. coli; FA GI, FilmArray gastrointestinal panel; PCR, polymerase chain reaction; STEC, Shiga toxin-producing E. col.
For all verified results (E. coli O157 was not counted as a separate pathogen), coinfections were observed in 28.8% of the total samples, 21.0% (n = 97) with two pathogens, 5.6% (n = 26) with three, and 2.2% (n = 10) with four or more pathogens. Except for C. cayetanensis, all pathogens detected were also observed as part of coinfections (Table 3). The proportion of detections relating to coinfections was not included in the assessment for these pathogens the positive specimens of which were ≤5, such as Cryptosporidium and C. cayetanensis.
EPEC and EAEC were the most common pathogens in coinfections. If EPEC and EAEC were deducted from analysis, the coinfection rates fell by half (19.4% of the positives and 13.6% of the total), with a significant decrease of coinfection-related detections for other pathogens. The majority of C. difficile (55.0%), astrovirus (66.7%), sapovirus (66.7%), Plesiomonas shigelloides (73.3%), and STEC (100.0%) detections were associated with coinfections. Norovirus GI/GII (23.3%) and Campylobacter (25.0%) were less associated with coinfections.
Temporal and spatial distribution of positive specimens
The 462 specimens analyzed in the present study were collected from 3 regions of China between January and September 2016. The temporal and spatial distribution of the positive specimens was analyzed.
The positive rates of norovirus GI/GII, V. parahaemolyticus, EPEC, and C. difficile varied greatly among the three regions (Table 4). In both the <5 years old group and the >5 years old group, the positive rates of EPEC were higher in Hunan (34.9% vs. 29.9%) than in Changning (18.2% vs. 15.4%) and Wuxi (12.0% vs. 15.7%). In both <2 years old groups and the >2 years old group, the positive rates of C. difficile were higher in Hunan (19.2% vs. 12.6%) than in Changning (14.3% vs. 4.8%) and Wuxi (11.1% vs. 2.2%).
Comparison of Positive Rates of Pathogens in Three Regions of China
The difference in positive rate between the two regions marked with the same letter was statistically significant.
The difference in positive rates of the three regions was statistically significant.
EAEC, enteroaggregative E. coli; EPEC, enteropathogenic E. coli; ETEC, enterotoxigenic E. coli; STEC, Shiga toxin-producing E. coli.
Different peaks of the positive rates of pathogens were observed (Fig. 1), especially for noroviruses, rotaviruses, some types of diarrheagenic E. coli, Salmonella, and C. difficile. The prevalence of pathogens was clearly seasonal, with viral infections more common in the winter and bacterial infections more common in the summer.
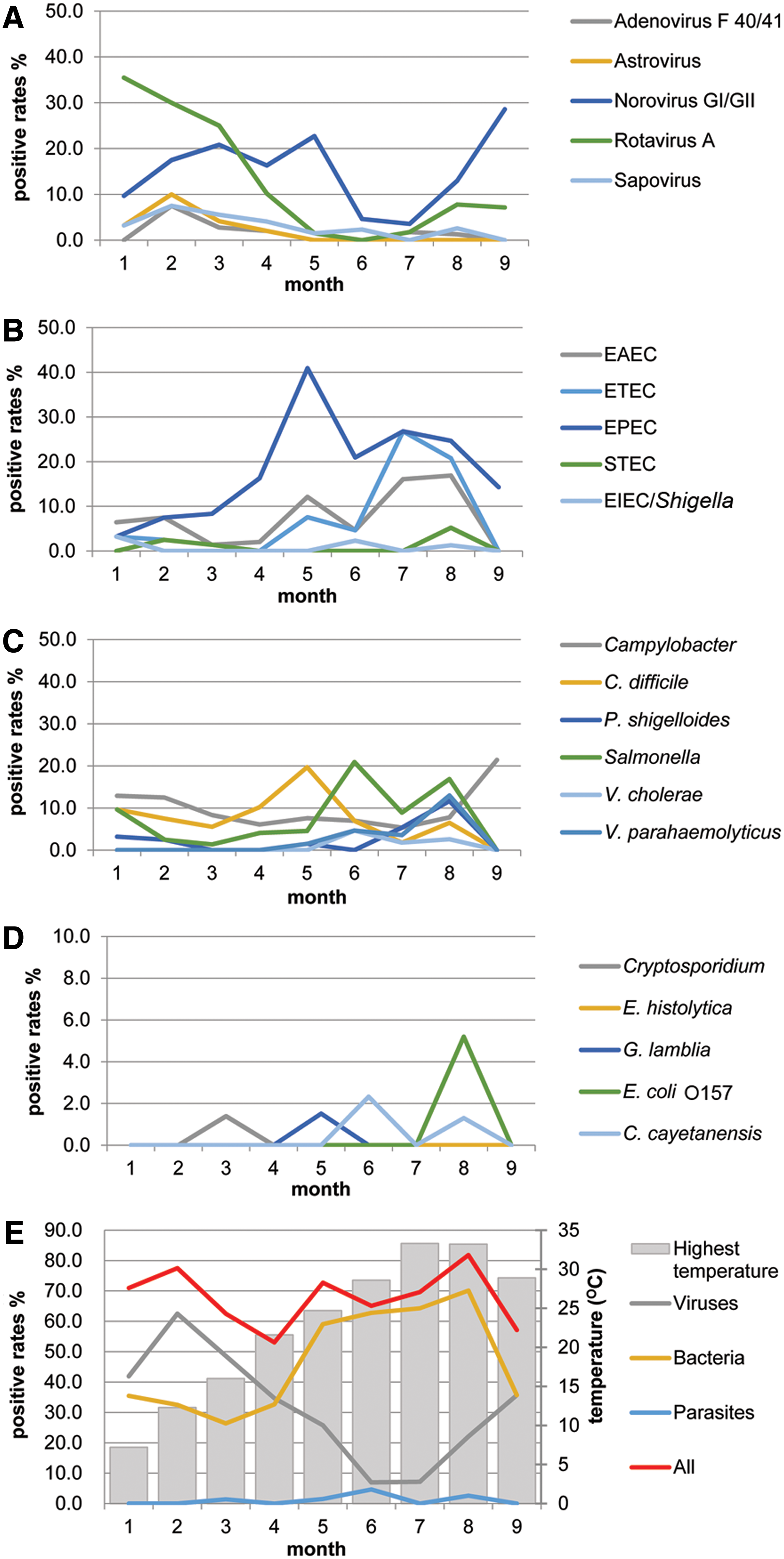
The variation of positive rates of different pathogens among different months.
Discussion
In this three-center molecular diagnosis evaluation, FA GI, real-time PCR, and culture methods were used for the detection of GI pathogens in clinical samples from patients with diarrhea. The performances of the FA GI and real-time PCR assays were evaluated, and the temporal and spatial characteristics of the distribution of various pathogens were analyzed.
The FA GI performed similarly in several studies. In general, the specificity was >96% and the sensitivity was >90% (Khare et al., 2014; Buss et al., 2015). Sensitivity varies in different studies, partly due to the low positive rate of certain pathogens. In our study, FA GI demonstrated high sensitivity per pathogen (≥94.5%) except for Salmonella (60.5%) and adenovirus (88.9%). Except for Salmonella, false negatives of other targets were ≤2.
One false negative of adenovirus occurred in the detection by FA GI. The comparator method and the method used for discordance analysis can detect 51 serotypes of human adenoviruses (species A–F). FA GI only detects species F serotype 40 (AdV40) and AdV41. Therefore, this false negative might be due to infection with other human adenoviruses other than AdV40/41.
In the testing of EAEC, only the aggR gene was targeted by real-time PCR, while the FA GI targets both aggR and aatA genes. False negatives by real-time PCR may not be due to the aggR gene, but most likely the PCR design.
With regard to the detection of Salmonella spp., the concordance between FA GI and real-time PCR was relatively high. FA GI detected more positive samples in both culture-positive and culture-negative specimens than the comparator method. However, FA GI only detected Salmonella spp. in about 50% of the culture-positive specimens, and real-time PCR detected fewer specimens. Both molecular methods had high false negative rates, similar to the findings in our previous study (Guan et al., 2016). Low bacteria load in specimens may be the major cause of false negative results observed with the two molecular assays.
EPEC can cause acute or persistent diarrhea in young children, but they can also be detected in healthy children and adults (Ochoa and Contreras, 2011). The positive rate of EPEC in Hunan (32.0%) was twice that of Changning (15.6%) and Wuxi (15.1%). The specimens of Hunan came from underdeveloped rural areas where the economy is relatively backwards, and the results were consistent with the finding that EPEC is more prevalent in developing regions (Trabulsi et al., 2002).
C. difficile is one of the most common organisms detected in diarrheal stool specimens (Gorbach, 1999; Sammons et al., 2013; Khare et al., 2014). However, about 60–70% of healthy newborns and infants have their intestines colonized by C. difficile, but do not show signs of disease, and between 12 and 24 months, C. difficile is gradually eliminated (Jangi and Lamont, 2010). In both <2 years old groups and the >2 years old group, the positive rates of C. difficile were higher in Hunan (19.2% vs. 12.6%) than in Changning (14.3% vs. 4.8%) and Wuxi (11.1% vs. 2.2%). Whether this difference is regionally specific will require continuous monitoring.
The positive rates of norovirus and V. parahaemolyticus in the three regions were also significantly different. These differences may reflect the regional characteristics of the pathogens' prevalence, but may also be related to the outbreaks in the area at the time of the study or bias caused by sampling.
Coinfections detected by FA GI far higher than those reported in the literatures (Khare et al., 2014; Buss et al., 2015; Spina et al., 2015). The positive rates of EPEC and EAEC were high and coinfection-related detections accounted for a large proportion, 75.0% for EPEC and 85.4% for EAEC, respectively. Norovirus GI/GII and Campylobacter were less associated with coinfections, while C. difficile, astrovirus, sapovirus, P. shigelloides, and STEC were more associated with coinfections. The correlation between pathogens and coinfections varied in different studies and may be affected by the sampling area and study population (Buss et al., 2015; Alejo-Cancho et al., 2017; Piralla et al., 2017).
FA GI has a high overall sensitivity and can detect more positive specimens and coinfections. A number of real-time PCR methods can be used in combination to screening for pathogens in stool samples. On account of the detection data, we observed the seasonal changes of the infections for different pathogens. Different positive rates of some pathogens were also found in these three regions, and continuous surveillance is needed to estimate whether actual regional differences exist, especially for V. parahaemolyticus and C. difficile infections. In this study, the inconsistency of NA extraction methods at different monitoring sites may affect the regional differences in pathogen positive rates, which is the limitation of this study.
Footnotes
Acknowledgments
This study was supported by the Ministry of Science and Technology of the People's Republic of China (2018ZX10712001-014), Pathogen Monitoring Capacity Building Project (Grant 131031102000150003), Shanghai Changning Specialty Medicine of Health and Family Planning—Pathogenic Microorganisms Test (20163004), and Wuxi Medical Innovation Platform [laboratory; CXPT(SYS)002]. We thank BioFire for providing the kits and instruments used in this study. We thank Dr. Shuyu Wu (CDC, United States, at the US Embassy, Beijing, China) for her suggestions in the analysis.
Disclosure Statement
No competing financial interests exist.