
Abstract
To strengthen the burden estimates for chronic sequelae of foodborne illness, we conducted a scoping review of the current literature for common foodborne pathogens and their associated sequelae. We aim to describe the current literature and gaps in knowledge of chronic sequelae associated with common foodborne illnesses. A comprehensive search was conducted in PubMed, EMBASE, and Web of Science for peer-reviewed articles published January 1, 2000 to April 1, 2018. Articles available in English, of any epidemiological study design, for 10 common foodborne pathogens (Campylobacter, Salmonella, Escherichia coli, Listeria, Shigella, Cryptosporidium, Cyclospora, Giardia, Yersinia, and norovirus) and their associated gastrointestinal (GI)- and joint-related sequelae were included. Of the 6348 titles screened for inclusion, 380 articles underwent full-text review; of those 380, 129 were included for data extraction. Of the bacterial pathogens included in the search terms, the most commonly reported were Salmonella (n = 104) and Campylobacter (n = 99); E. coli (n = 55), Shigella (n = 49), Yersinia (n = 49), and Listeria (n = 15) all had fewer results. Norovirus was the only virus included in our search, with 28 article that reported mostly GI-related sequelae and reactive arthritis (ReA) reported once. For parasitic diseases, Giardia (n = 26) and Cryptosporidium (n = 18) had the most articles, and no results were found for Cyclospora. The most commonly reported GI outcomes were irritable bowel syndrome (IBS; n = 119) and inflammatory bowel disease (n = 29), and ReA (n = 122) or “joint pain” (n = 19) for joint-related sequelae. Salmonella and Campylobacter were most often associated with a variety of outcomes, with ReA (n = 34 and n = 27) and IBS (n = 17 and n = 20) reported most often. This scoping review shows there are still a relatively small number of studies being conducted to understand specific pathogen/outcome relationships. It also shows where important gaps in the impact of chronic sequelae from common foodborne illnesses still exist and where more focused research would best be implemented.
Introduction
Foodborne diseases (FBDs) substantially impact public health, the economy, and society. In the United States, foodborne infections result in an estimated 48 million cases of illness every year with over 100,000 hospitalizations and 3000 deaths (Scallan et al., 2011). The burden of FBDs goes beyond acute illness, however. Infections with foodborne pathogens can result in long-term postinfectious sequelae (PIS) that may not manifest for weeks, months, or even years after initial infection. Many of these sequelae involve chronic bowel and gastrointestinal (GI) dysfunction, such as irritable bowel syndrome (IBS) and inflammatory bowel disease (IBD). Others, such as reactive arthritis (ReA), impact the immune system or other organ systems. It is critical that the considerable health consequences of PIS be included in estimates of disease burden to provide a more complete understanding of the impacts of foodborne illness, as these estimates inform decisions of regulatory and public health agencies, industry, and the public.
While chronic sequelae are not included in estimates of FBD incidence due to current public health surveillance strategies, they are increasingly included in disease burden studies that utilize integrated measures, such as disability-adjusted life years (DALYs), quality-adjusted life years (QALYs), or economic costs of illness. While DALYs and QALYs consider life-years lost due to premature death and a 0-to-1 scale to measure the severity of a given disease state, cost of illness studies combine direct and indirect health care costs, productivity losses, and monetized welfare losses due to both morbidity and mortality (Mangen et al., 2010, 2013). Annually, the cost of foodborne illness in the United States has been estimated to range from $14 billion for 14 highest disease pathogens (Hoffmann et al., 2012) to $36 to $78 billion for all foodborne illnesses (Scharff, 2012; Minor et al., 2015). In addition, seven priority pathogens have been estimated to cause 112,000 DALYs (Scallan et al., 2015). A number of chronic sequelae are included in one or more of these studies: Guillain/Barré Syndrome (GBS) (Campylobacter), hemolytic uremic syndrome (HUS) and related long-term kidney disease (Escherichia Coli O157:H7), IBS (Campylobacter), newborn complications due to congenital infection (Listeria, Toxoplasma), developmental delays (Cronobacter), and ReA (Campylobacter, Salmonella, Shigella, and Yersinia). Nevertheless, a number of potential PIS are excluded from these studies.
Incorporating sequelae into disease burden estimates is challenging. This work requires establishing foodborne exposures as the cause of the sequelae, quantifying the likelihood of sequelae, and characterizing the duration and severity of potential health outcomes. Analytical models must then combine the information with other data to properly estimate DALYs or dollars. Establishing causality and quantifying outcome likelihood are often difficult because of the nature of disease surveillance and the use of retrospective study designs. Epidemiological challenges in the causal chain include missing data related to the latency between infection and sequelae, underlying host cofactors (e.g., genetics, prior exposures, clinical/subclinical comorbidities, microbiome, etc.), as well as pathogen and exposure characteristics (e.g., strain, virulence factor expression, dose of exposure, severity of acute illness, management of acute illness, etc). Often, the sequelae themselves are difficult to diagnose and, absent active surveillance with consistent case definitions, incidence estimates may be inaccurate. Moreover, pooling estimates for a given pathogen/sequelae combination is impractical or improper given differences in study type, study design, risk factors assessed, and underlying target populations. Finally, because these diseases may not manifest immediately following infection, they are not part of routine public health monitoring. In addition, because they lie at the intersection of infectious and chronic diseases, there is often limited funding from granting agencies that are often focused on one area or the other.
In 2016, the authors formed the Foodborne Illness Chronic Sequelae Working Group under the leadership of the U.S. Food and Drug Administration's Center for Food Safety and Applied Nutrition (FDA-CFSAN). With representatives from the U.S. Naval Medical Research Center and The University of Arizona, this group brought together experts in food science, epidemiology, economics, and clinical medicine to address what is known in the current literature regarding the causal links between foodborne illness and specific PIS, as well as the public health burden of these outcomes. The goal of this initial work was to better understand the breadth of the current literature and usefulness of secondary analysis of the findings within this literature. Additionally, the group aimed to identify gaps in the research related to these outcomes. This article is the result of this ongoing collaboration and describes a scoping review conducted to determine the extent of the peer-reviewed scientific literature pertaining to 10 common FBDs and the 2 most commonly reported PIS, GI, and joint-related rheumatological disorders.
Materials and Methods
Selection of pathogens and outcomes
Specific GI and joint outcomes were chosen based on expert opinion of the most common sequelae under review for the last 10 years that had a likely link to foodborne illness. The 10 pathogens selected were based on their incidence and costs of illness in the United States (Hoffmann et al., 2012; Scallan et al., 2015), as well as due to previously identified associations with the sequelae of interest (Batz et al., 2013). Because our group's primary goal is to improve burden estimates of FBDs in the United States, other outcomes that may be considered GI, such as malabsorption in children of lower and middle-income countries, which is well documented (Rogawski et al., 2017), were not included.
Identifying relevant studies
Whereas a systematic review focuses on a specific research question and may be limited to select study designs, a scoping review that addresses a broader range of questions, is not limited to a specific study methodology (Arksey and O'Malley, 2005), and can help contextualize various estimates and measures coming out of the studies. The steps taken for this scoping study were first described by Arksey and O'Malley (2005) and refined by Levac et al. (2010). The stages in this review largely follow this described methodology. In addition, our group extracted other data for development in future review articles.
To comprehensively search the literature, we used a multi-tiered approach, including searching multiple electronic databases, hand searching based on reference lists of captured articles, and reviewing publications by key authors in this area. The first step in this process was to develop the inclusion and exclusion criteria (Table 1). As with other scoping reviews, this process was iterative, based on what was found in the literature and what the team deemed relevant to the research questions.
Inclusion and Exclusion Criteria
See Appendix 1 for full search terms.
DALY, disability-adjusted life year; EQ-5D, EuroQoL 5-Dimension; GERD, gastroesophageal reflux disease; IBD, inflammatory bowel disease; IBS, irritable bowel syndrome; QALY, quality-adjusted life year.
Search terms were originally created in PubMed; then they were modified to search in Embase and Web of Science with the help of a medical librarian (J.M.). Due to the complexity of the search, each pathogen was divided among team members and searched individually in PubMed for the pathogen “AND” the first condition “OR” second condition “OR,” and so on (Appendix Table A1). We tracked the results of each iteration by pathogen in an Excel spreadsheet to identify necessary changes, deletions, or edits to the search terms. For the pathogens, we included any species or serotype within the genera, (Table 1), known to be the etiologic agent of foodborne illness in humans. Exceptionally, only data pertaining to nontyphoidal serovars of Salmonella enterica were included in the final data extraction. For brevity, etiologic agents are referred to throughout the text at the genus level, with the exception of E. coli, which is identified as “E. coli,” its commonly recognized name.
The search was then expanded by utilizing the MeSH Terms database to identify the MeSH headings and subheadings that map to each pathogen (or infection with pathogen) and condition. After each team member performed individual searches, a list of all search terms and MeSH Headings was compiled. Next, a search for all systematic reviews for each pathogen and condition was conducted. Key words and MeSH headings were extracted from these articles and added to the spreadsheet. The list was reviewed to find terms that were too broad (e.g., “consequences” returned far too erroneous searches, whereas “long-term consequences” returned more specific results), duplicates (e.g., “Crohn's” and “Crohn's disease” returned very similar results), and phrases that were missing due to differences in terminology (e.g., “bacillary dysentery” is often used to describe “bloody diarrhea”). Excel was used to map general search terms to MeSH headings, to the corresponding search term in Embase, and to the EMTree term (similar to MeSH term). A parallel search was completed through Embase in the EMTree search engine entering the general search term used in PubMed and then retrieving the preferred term. A similar process was applied to create the search for Web of Science. Multiple search iterations were shared between reviewers and experts at the FDA to provide additional feedback. The final searches combined all pathogens with all conditions because of the nature of the literature—many authors wrote about multiple pathogens for one condition or vice versa, leading to many search results for each database (Appendix Table A1).
Study selection
Covidence (2019) was used for study selection. This online tool allows for quick screening of references simultaneously by various team members. Two reviewers voted “Yes,” “No,” or “Maybe” for inclusion. When discrepancies occurred, Covidence automatically moved discordant results to a separate review area, and a third reviewer determined final inclusion. If inclusion could not be determined, the full team reviewed the article for inclusion. Hand searches were also conducted from references of articles marked for inclusion.
Searches among three databases (PubMed, Embase, and Web of Science) occurred between mid-August and mid-November 2017. All included articles were published from January 1, 2000 to November 1, 2017; a second search conducted in April 2018 yielded no additional articles. Data extraction was completed in May 2018.
Charting the data
While Covidence was very useful for organizing and reviewing articles based on inclusion and exclusion criteria, the embedded data extraction tool was designed for randomized control trials and did not fit the needs of this scoping review. We developed a data extraction form in Qualtrics (2013, Provo, UT) to allow multiple, simultaneous users and to establish range and logic checks.
Throughout the review, other unanticipated pathogens, outcomes, or pathogen/outcome combinations were often reported alongside the original search terms set out in the article. This information was recorded in the process of collecting data from the original search. Initially, the form was designed to capture these under “Other.” However, the form was quickly modified to include more common findings, specifically “infectious gastroenteritis,” “traveler's diarrhea,” “Guillan Barré Syndrome,” “acute gastroenteritis,” and “joint pain,” and data entry checks were conducted to ensure proper accounting. For “traveler's diarrhea” specifically, we conducted a follow-up search, including the illness name and excluding any pathogen names. From this process, we found an additional four articles. These articles were included as part of the hand search results.
A shared Google document was developed to track each article assignment in real-time, as well as to show completed reviews and document any articles excluded at the data extraction step. For example, review articles (n = 49) that did not present any original data were excluded once all the original, pertinent articles were included. During the review process, we excluded duplicate representation when multiple articles addressed findings from the same event (Walkerton outbreak follow-up study) (Garg et al., 2005; Richards, 2005; Marshall et al., 2006; Marshall, 2009; Thabane et al., 2009; Chloé Villani et al., 2010; Ford et al., 2010; Thakur et al., 2010), which used the same data on the incidence of outcomes, but addressed different research questions. Of the eight articles describing different aspects of the Walkerton outbreak, seven studies were excluded, while one all-encompassing article was included for data extraction (Thabane et al., 2010).
Following data extraction and data entry, a two-step quality control data cleaning process was conducted. To ensure consistency among reviewers, each member on the 4-person team was assigned 20 articles another team member had reviewed, 10 that were excluded, and 10 that were included (nonblinded). For excluded articles, the secondary reviewer read the article and recorded whether they concurred or disagreed with the exclusion criteria. For included articles, data entry was repeated and compared with the original data extraction form to ensure consistency. Any inconsistencies were discussed among the entire team with any minor discrepancies fixed and any systematic differences addressed in the data cleaning process.
Results
Collating, summarizing, and reporting
A total of 8880 references from the 3 databases was initially imported into Covidence. After autoremoval of duplicates (n = 2532), 6348 titles were screened for inclusion (K.P.-B., E.A., A.A.). If the title did not provide enough information, the abstract was reviewed to determine inclusion. Following initial screening, 541 studies were assessed for full-text eligibility through abstract review (K.P.-B., E.A., A.A.). An additional 41 studies were selected for full-text review from references cited by included articles (K.S.). Full-text review of 380 articles (K.S., E.A., K.P.-B., A.A.) was completed; of these, 251 studies were excluded. The final 129 unique articles were included in the scoping review for data extraction. The full Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) diagram is shown in Figure 1 (Tricco et al., 2018).
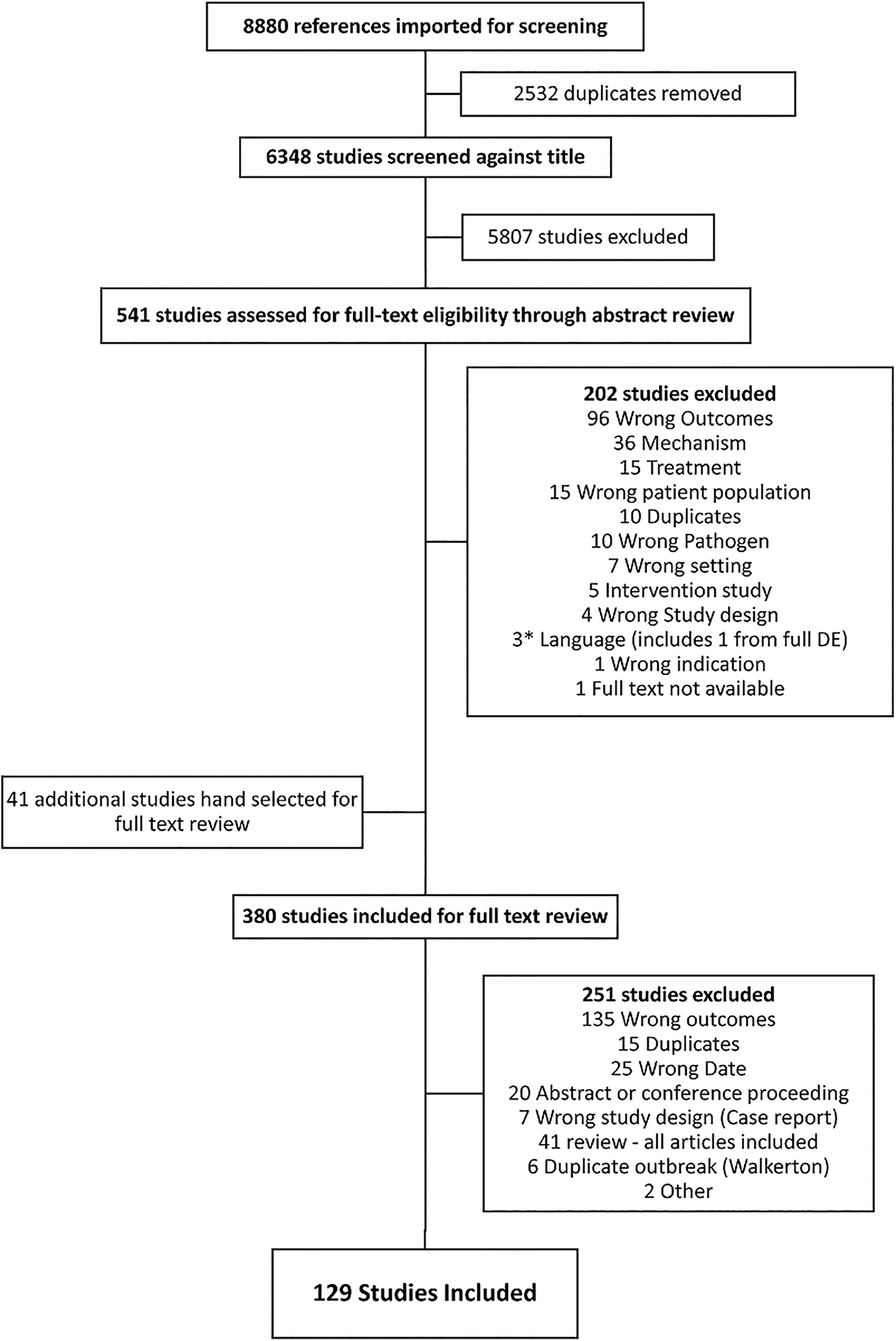
PRISMA diagram of scoping review.
Among the 129 included articles, most utilized a prospective cohort (n = 41; 31.8%), retrospective cohort (n = 34; 26.4%), or case/control (n = 17; 13.2%) study design. Only 11 (8.5%) systematic reviews and/or meta-analysis articles were found; of these, 6 reviewed IBS, 3 included IBD, and 2 reviewed ReA (data not shown). The majority of case populations were patients detected through routine surveillance data (n = 48; 37.2%) or through outbreaks (n = 39; 30.2%). Studies were conducted from 1960 to 2016 with an average study length of 19.1 months (range 1–60 months) after excluding studies longer than 5 years (n = 9) for the range calculation. Studies most commonly recruited patients from Europe (n = 65), the United States (n = 26), and other countries (n = 24). On average, 46.4% of cases (range: 5–99.4%) in the studies reporting demographics (n = 83; 64.3%) were male (Table 2).
Study Characteristics for 129 Included Studies
Counts for cases and controls were collected but missing for 38 (number of cases) and 81 (age range); this information was excluded from this table due to missingness.
Other countries included: Canada (n = 7), South Korea (n = 4), India (n = 2), Mexico (n = 2), Chile (n = 1), China (n = 1), Israel (n = 1), and multiple (n = 6).
Pathogens and chronic outcomes search terms
The original search included 10 common foodborne pathogens and 9 possible outcomes (Table 1). The final evaluated 129 articles reported 544 pathogen/outcome combinations (Fig. 2). For example, an article reviewing IBS may report incidence rates for four different pathogens. Each pathogen/outcome combination was accounted for, with many articles reporting multiple results for each (incidence rates, hospitalizations, prevalence, etc.). The most commonly reported GI outcomes were IBS (n = 119) and IBD (n = 29) (Fig. 2 for counts and Table 3 for references). Counts for IBS included all forms of IBS (IBS with constipation [IBS-C], IBS with diarrhea [IBS-D], and IBS with mixed symptoms [IBS-M]), although many studies did not make the distinction by type. Other GI-related outcomes included ulcerative colitis (n = 22), Crohn's disease (n = 25), dyspepsia (n = 29), functional diarrhea (n = 14), and functional constipation (n = 13). Four articles reported celiac disease. For joint outcomes, the most commonly reported outcome was ReA (n = 122), followed by articles that used “joint pain” as an outcome (n = 19). Articles with results classified as “Other” included diverse outcomes, such as abdominal pain or “functional bowel disease” for GI (n = 26), septic arthritis or rheumatologic symptoms for joint (n = 19), and chronic fatigue syndrome and depression for a general other category (n = 78).
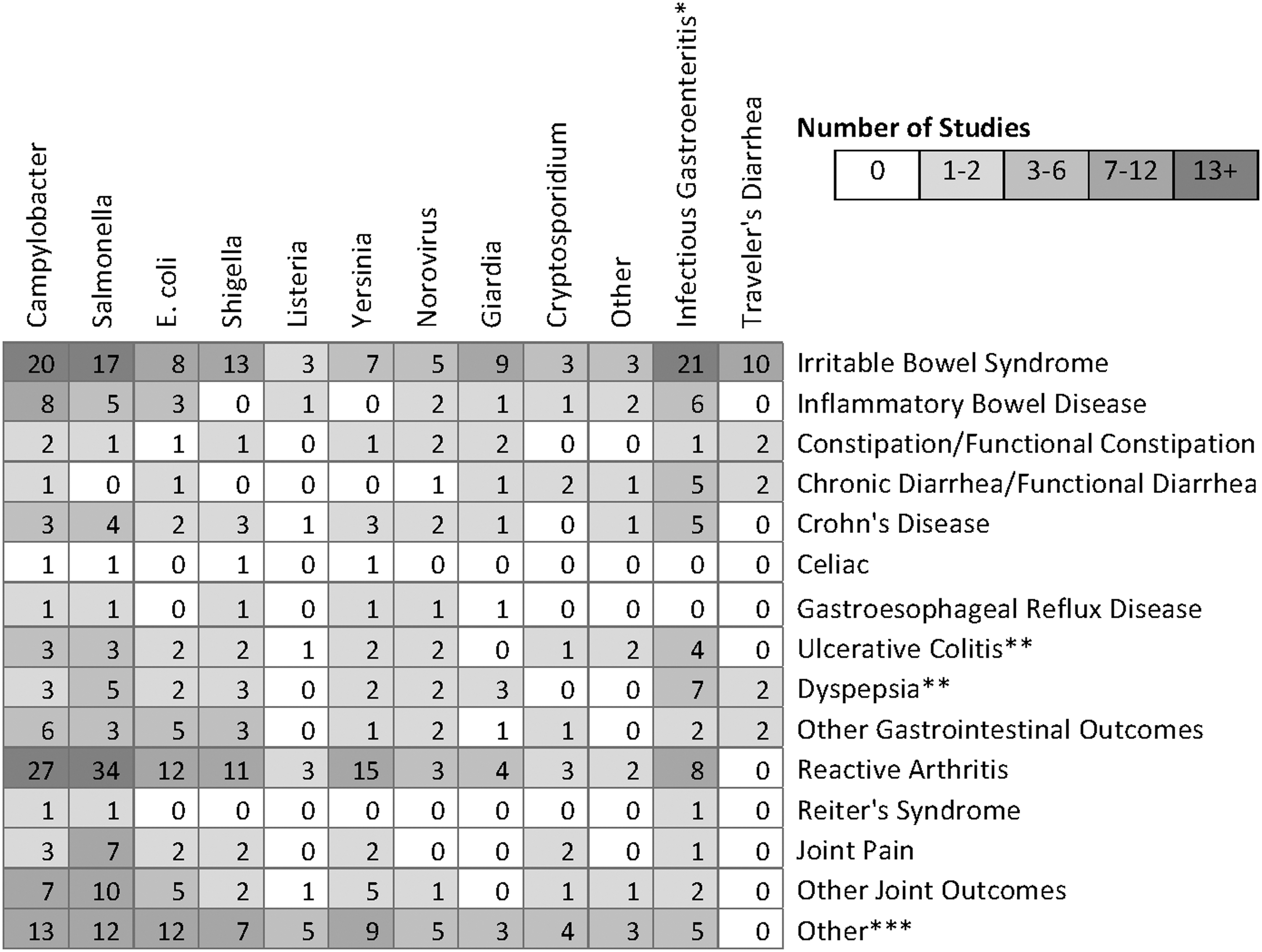
Heat map of articles for each pathogen and outcome. *IGE includes infectious gastroenteritis and those articles which shared combined results, not individual pathogen results. **Not included in original search. ***Other includes Guillain/Barré Syndrome.
References for Articles by Pathogen and Chronic Sequelae a
See Appendix 2 for description of “other”.
Review articles. **Systematic review and meta-analyses.
IBD, inflammatory bowel disease; IBS, irritable bowel syndrome.
Of the pathogens searched, those most commonly associated with chronic outcomes were Salmonella (n = 104) and Campylobacter (n = 99). For the bacterial diseases, E. coli (n = 55), Shigella (n = 49), and Yersinia (n495) had the next highest results, with Listeria (n = 15) having the fewest published articles related to these outcomes. Among the studies with E. coli subtype information available, 18 focused on Shiga toxin–producing E. coli and Enterohemorrhagic E. coli (STEC/EHEC; 4 STEC generally; 10 on O157:H7; and 4 on a non-O157 serovar), 4 on non-STEC cases, and 1 on mixed pathotypes.
Norovirus was the only viral pathogen included, and 28 reports of mostly GI-related outcomes, with ReA reported three times. For parasitic diseases, Giardia and Cryptosporidium were found in 26 and 18 articles, respectively, while articles reporting “infectious gastroenteritis” and “traveler's diarrhea” were found often (68 and 18 publications, respectively). No results were found for Cyclospora for any of these chronic outcomes. Finally, “Other” (n = 15) included a wide variety of other less common foodborne pathogens (Toxoplasma, Hepatitis A, Clostridium parvum, etc). Appendix 2 lists all “Other” outcomes and pathogens.
The two most studied pathogens, Salmonella and Campylobacter, were most often associated with a variety of ReA (n = 34 and n = 27, respectively) and IBS (n = 17 and n = 20, respectively) outcomes. Across all pathogens, IBS and ReA had the most data. Several studies (n = 21) that did not differentiate by pathogen reported associations between infectious gastroenteritis and IBS as well.
Table 3 provides references to all articles included in the scoping review by pathogen and chronic sequelae, with those reporting data for multiple pathogens and/or multiple outcomes referenced for each pair accordingly.
In addition to pathogens and health outcomes, the search terms included those related to disease burden (Table 1). Of the 129 articles considered in the scoping review, 17 (13%) included a disease burden assessment for the chronic sequelae considered. Nine (53%) of these studies were conducted in Europe, five (29%) in North America, two (12%) in Oceania, and one (6%) worldwide. Thirteen (76%) reported a single measure of disease burden. Nine (53%) included a cost of illness analysis, while two (12%) reported general or available cost. Nine (53%) included a nonmonetary assessment of disease burden using the DALY; two (12%) provided years lost to disability (YLD); and one (6%) used the QALY. Disease burdens were most frequently reported for Campylobacter and Salmonella, followed distantly by Shigella, Yersinia, and E. coli. Table 4 shows the number of studies reporting disease burden for each pathogen/sequelae combination. Within disease burden measures, DALY and YLD were frequently reported to assess IBD, IBS, and ReA caused by Campylobacter and Salmonella. Reports of cost of illness were found for the three sequelae most frequently reported for ReA. No studies reported DALYs for E. coli, Shigella, or Yersinia.
Number of Studies Reporting Disease Burden of Sequelae from Included Pathogens
DALY, disability-adjusted life year; IBD, inflammatory bowel disease; IBS, irritable bowel syndrome; ReA, reactive arthritis; YLD, years lost to disability.
Discussion
This scoping review identified 129 studies mapped to 15 chronic sequelae related specifically to GI and joint function and to 10 pathogens. Given the heterogeneity of existing studies, the review synthesizes available evidence into a usable list of references (Table 3), identifies gaps where additional research is needed, and provides a database of extracted information our team will use for future studies.
Overall, substantial research is published on two PIS, IBS, and ReA. For both of these sequelae, links have been made with the nonspecific exposures of “infectious gastroenteritis” and “traveler's diarrhea,” and with specific pathogens, most commonly Campylobacter and non-Typhoidal Salmonella. However, key research gaps in incidence rates among varying populations, duration of sequelae, and health care utilization complicate estimates of overall disease burden. Less commonly implicated pathogens, such as Shigella, Yersinia, and Listeria, have been studied far less (Scallan et al., 2011); E. coli was also not well represented in these results, despite an established relationship between E. coli O157:H7 and a serious PIS, HUS. While HUS was not part of our search criteria, it became evident that GI and joint outcomes are either less commonly studied or less commonly reported in relation to E. coli O157:H7. Also, we found that very little research assessing the relationship between Cyclospora infection and any chronic sequelae. Given the increasing emergence of this pathogen and the size of recent outbreaks caused by it (Casillas et al., 2018), further study of the possible sequelae related to infection is warranted. Current research in similar parasitic pathogens may help guide this research. Regarding the study populations, almost 65% of those studied were men highlighting a need to reduce the disparity in these studies, particularly because several studies found women to be at higher risk of developing certain outcomes such as IBS.
In addition to reviewing the literature on the epidemiology of these outcomes, this study aimed to determine the breadth and depth of articles related to the burden of PIS. Our review shows that disease burden estimates for sequelae are limited, with only 13% of identified studies reporting at least one burden measure. Campylobacter and Salmonella are the pathogens for which disease burdens of IBS, IBD, and ReA were most commonly reported. This pattern is consistent with the proportionally large representation of these pathogens in our sampled studies. The lack of studies with disease burden measures, particularly DALYs, for chronic sequelae of other major pathogens, such as E. coli, Shigella, and Yersinia, suggests avenues for more focused research. Newly available data, especially on chronic sequelae such as ReA, GBS, and IBS, will help decision makers generate more accurate burden estimates.
This review provides a comprehensive list of the available data on ten select foodborne pathogens of concern and some of their selected sequelae. Detailed characterization of sequelae are critical for their incorporation into economic cost of illness estimates, and other disease burden studies using DALYs or QALYs (Scallan et al., 2011; Hoffmann et al., 2012; Mangen et al., 2013; Batz et al., 2014). Many studies in this review not only identified the relationship between FBDs and specific chronic sequelae, but also gave estimates of their incidence, duration, and severity. Future estimates of U.S. FBD burden, such as those by FDA, can incorporate these data (Minor et al., 2015).
In addition to informing regulatory policy and improving estimates of the burden of disease, these findings have implications for clinical care. IBS is prevalent globally and represents a high proportion of gastroenterology-associated diagnoses in Western countries. Acute enteric infection has been linked epidemiologically in multiple reviews of IBS (Keithlin et al., 2014b, 2015; Porter et al., 2016) (Table 3), and the Rome Foundation, in its release of the Rome IV criteria (used to diagnose IBS), has defined postinfectious IBS (PI-IBS); however, even these criteria highlight some of the ambiguity in the exposure and the timing of postexposure symptom onset (Barbara et al., 2018). While there are no specific treatments for PI-IBS, consensus recommendations include dietary and lifestyle modification, education about disease risk and prognosis, and potential pharmacological intervention. Clinically, PI-IBS has recently gained recognition among gastroenterologists and others as a significant portion of the overall IBS picture, as noted in a report and accompanying editorial published after this review concluded (Barbara et al., 2018; Spiller, 2018). Given that PI-IBS may account for a large proportion of IBS (Shah et al., 2012), large randomized, double-blind, placebo-controlled trials are needed to further guide and refine PI-IBS clinical management (Spiller, 2018).
Strengths
Our group was comprised primarily of epidemiologists, economists, and clinicians from both academia and government agencies, allowing for a wide variety of input and priorities to be addressed. This collaborative and iterative process represents the largest scoping review on this topic to be conducted to date. While other review articles (Appendix 2) have addressed specific pathogen/outcome combinations, this is the first comprehensive review of the literature in this area with the goal of determining where current strengths and gaps lie concerning our specific target pathogens and outcomes. By focusing not only on the incidence of these outcomes following infection but also the burden, we were able to collect data on duration and cost. For epidemiologists, this information can help guide the type of study design that should be put into place to further assess the relationships. For regulatory agencies that must make decisions based on all available data, this new information on sequelae can lead to the development of new and updated burden estimates. Additionally, it helps identify data gaps. The dataset compiled in this project will be used to examine each pathogen/outcome more closely and develop additional resources for researchers in multiple disciplines. Finally, we were able to take advantage of multiple resources from a medical librarian, whose perspective was pivotal to the development of the search strategies using fairly new online resources (Covidence and Qualtrics) to efficiently conduct this review in a timely manner (9 months).
Limitations
Our team chose to focus only on GI and joint outcomes for this review because they were the most commonly reported. We acknowledge that other outcomes not included in our search, such as HUS and GBS, have both public health and economic impacts. For efficiency and future use, we collected data on reported outcomes that were not part of the original search. However, these results do not fully reflect the scope of literature on each of the outcomes our search did not include. GBS, which is included in the “Other” category, for instance, has a much larger set of literature related to many of these pathogens, particularly Campylobacter. These results simply capture articles that include both GBS and other GI or joint outcomes. For our inclusion and exclusion criteria, as noted above, we chose to include only articles published after January 1, 2000. We acknowledge that other important articles were published before this date; however, the goal was to determine the current level of information, and many of the newer articles utilized information from or expanded upon findings of older articles.
Studying chronic outcomes is challenging in epidemiological studies due to the cost and time needed for extensive follow-up of relatively rare events. Because many of the sequelae of interest have nonspecific symptoms, it is difficult to attribute specific etiologies to them. Attributing these outcomes to prior infections may also be difficult as patients may not have seen the same physician for follow-up if they develop sequelae later in life. Medical record keeping in the United States is also not uniform and has changed. For these reasons, we considered reviewing the breadth of literature to be very important.
Future research
Moving forward, we hope to further synthesize the results that we have found in this review. This synthesis will include improving the incidence, duration, and severity estimates currently used to derive the burden of foodborne infectious diseases. We also plan to further analyze specific pathogen/sequelae relationships by utilizing the database of extracted data on incidence rates, duration, and economic outcomes. These data will allow for a more in-depth analysis of heterogeneity between studies and a more nuanced understanding of the research gaps in this field.
Conclusions
This scoping review is a major step in furthering understanding of the relationships between foodborne pathogens and PIS. For researchers working in specific areas, we hope this work will serve as a comprehensive resource to determine the current status of studies in each relationship and catalog the gaps that still exist in specific pathogen/sequelae pairs.
Footnotes
Acknowledgments
The authors would like to acknowledge Beverly Wolpert and André Markon from the FDA Center for Food Safety and Applied Nutrition as well as Angela Lasher and Andrew Estrin from the FDA Office of Planning for their guidance, leadership, and input throughout this project.
Disclaimer
The views expressed in the submitted article are the authors' own and not an official position of the institution or funder. The findings and conclusions in this study are those of the authors and do not necessarily represent the official position of the United States Food and Drug Administration.
The views expressed in this article are those of the authors and do not necessarily reflect the official policy of the U.S. Department of Health and Human Services, the U.S. Food and Drug Administration, or the U.S. Government.
Disclosure Statement
The authors declare no conflicts of interest.
Funding Information
Sources of support: FDA Grant Number HHSF22320171-0181P.
Appendix Table A1
Search Strategy Used for PubMed, EMBASE, and Web of Science
| PubMed | EMBASE | Web of Science |
|---|---|---|
| (((“cyclospora”[MeSH Terms] OR “cyclospora”[All Fields] OR “giardia”[MeSH Terms] OR “giardia”[All Fields] OR “cryptosporidium”[MeSH Terms] OR “cryptosporidium”[All Fields] OR “norovirus”[MeSH Terms] OR “norovirus”[All Fields] OR “listeria”[MeSH Terms] OR “listeria”[All Fields] OR “yersinia”[MeSH Terms] OR “yersinia”[All Fields] OR “shigella”[MeSH Terms] OR “shigella”[All Fields] OR “Escherichia coli”[MeSH Terms] OR “Escherichia coli”[All Fields] OR “salmonella”[MeSH Terms] OR “salmonella”[All Fields] OR “campylobacter”[MeSH Terms] OR “campylobacter”[All Fields])) AND (“functional gastrointestinal disorder”[All Fields] OR (“chronic”[All Fields] AND gastrointestinal[All Fields]) OR “chronic bowel”[All Fields] OR “functional gastrointestinal”[All Fields] OR “functional bowel”[All Fields] OR (functional[All Fields] AND (“colon”[MeSH Terms] OR “colon”[All Fields] OR “colonic”[All Fields])) OR “functional GI”[All Fields] OR (inflammatory[All Fields] AND gastrointestinal[All Fields]) OR “functional dyspepsia”[All Fields] OR “celiac”[All Fields] OR “Crohn's”[All Fields] OR “ulcerative colitis”[All Fields] OR “irritable bowel syndrome”[All Fields] OR “inflammatory bowel disease”[All Fields] OR “reactive arthritis”[All Fields] OR “Reiter's Syndrome”[All Fields] OR “IBS”[All Fields] OR “IBD”[All Fields] OR “post-infectious sequelae”[All Fields] OR “sequelae”[All Fields] OR “long-term”[All Fields] OR “long term”[All Fields] OR “long-term”[All Fields] OR “consequences”[All Fields] OR “conditions”[All Fields] OR “outcomes”[All Fields])) AND (“DALY”[All Fields] OR “QALY”[All Fields] OR “duration”[All Fields] OR “burden of disease”[All Fields] OR “disease burden”[All Fields] OR “burden”[All Fields] OR “YLL”[All Fields] OR “YLD”[All Fields] OR “EQ-5D”[All Fields] OR “treatment cost”[All Fields] OR “healthcare utilization”[All Fields] OR “cost”[All Fields] OR “hospitalization”[All Fields] OR “hospitalized”[All Fields] OR “morbidity”[All Fields] OR “mortality”[All Fields] OR “severity”[All Fields] OR “outpatient”[All Fields] OR “disability”[All Fields] OR “monetary”[All Fields] OR “medical care”[All Fields]) Filters: Publication date from 2000/01/01; Humans; English | (“campylobacter”:ti,ab,kw OR “cyclospora”:ti,ab,kw OR “giardia”:ti,ab,kw OR “salmonella”:ti,ab,kw OR “listeria”:ti,ab,kw OR “cryptosporidium”:ti,ab,kw OR “norovirus”:ti,ab,kw OR “yersinia”:ti,ab,kw OR “shigella”:ti,ab,kw OR “escherichia coli”:ti,ab,kw) AND (“functional gastrointestinal disorder”:ti,ab,kw OR (“chronic”:ti,ab,kw AND “gastrointestinal”:ti,ab,kw) OR “chronic bowel”:ti,ab,kw OR “functional gastrointestinal”:ti,ab,kw OR “functional bowel”:ti,ab,kw OR (“functional”:ti,ab,kw AND (“colon”:ti,ab,kw OR “colonic”:ti,ab,kw)) OR “functional gi”:ti,ab,kw OR (“inflammatory”:ti,ab,kw AND “gastrointestinal”:ti,ab,kw) OR “functional dyspepsia”:ti,ab,kw OR “celiac”:ti,ab,kw OR “ulcerative colitis”:ti,ab,kw OR “irritable bowel syndrome”:ti,ab,kw OR “inflammatory bowel disease”:ti,ab,kw OR “reactive arthritis”:ti,ab,kw OR “ibs”:ti,ab,kw OR “ibd”:ti,ab,kw OR “post-infectious sequelae”:ti,ab,kw OR “sequelae”:ti,ab,kw OR “long-term”:ti,ab,kw OR “long term”:ti,ab,kw OR “consequences”:ti,ab,kw OR “conditions”:ti,ab,kw OR “outcomes”:ti,ab,kw OR “reiter syndrome” OR “chronic inflammatory bowel disease”) AND (“daly”:ti,ab,kw OR “qaly”:ti,ab,kw OR “duration”:ti,ab,kw OR “burden of disease”:ti,ab,kw OR “disease burden”:ti,ab,kw OR “burden”:ti,ab,kw OR “yll”:ti,ab,kw OR “yld”:ti,ab,kw OR “eq-5d”:ti,ab,kw OR “treatment cost”:ti,ab,kw OR “healthcare utilization”:ti,ab,kw OR “cost”:ti,ab,kw OR “hospitalization”:ti,ab,kw OR “hospitalized”:ti,ab,kw OR “morbidity”:ti,ab,kw OR “mortality”:ti,ab,kw OR “severity”:ti,ab,kw OR “outpatient”:ti,ab,kw OR “disability”:ti,ab,kw OR “monetary”:ti,ab,kw OR “medical care”:ti,ab,kw) AND [english]/lim AND [humans]/lim AND [2000–2017]/py NOT ([embryo]/lim OR [fetus]/lim OR [infant]/lim OR [newborn]/lim OR “bloodstream infection”/de OR “hospital infection”/de OR “pneumonia”/de OR “sepsis”/de OR “urinary tract infection”/de) | TOPIC:(Cyclospora OR Giardia OR Salmonella OR Listeria OR Norovirus OR Yersinia OR Shigella OR Cryptosporidium OR “Escherichia coli” OR “E coli” OR “e. coli” OR Campylobacter) AND TOPIC:(gastrointestinal OR “chronic bowel” OR “functional gastrointestinal” OR “functional bowel” OR “functional gi” OR “functional colonic” OR (“inflammatory” AND “gastrointestinal”) OR “functional dyspepsia” OR “celiac” OR “ulcerative colitis” OR “irritable bowel syndrome” OR “inflammatory bowel” OR “reactive arthritis” OR “ibs” OR “ibd” OR “post-infectious sequelae” OR “sequelae” OR “long-term” OR “long term” OR “consequences” OR “conditions” OR “outcomes” OR “reiter syndrome” OR “chronic inflammatory bowel disease” crohn OR crohns OR dyspepsia OR celiac) AND TOPIC: (“daly“OR “qaly“OR “duration” OR “burden of disease” OR “disease burden“OR “burden“OR “yll“OR “yld“OR “eq-5d“OR “treatment cost” OR “healthcare utilization” OR “cost“OR “hospitalization“OR “hospitalized“OR “morbidity“OR “mortality“OR “severity“OR “outpatient“OR “disability“OR “monetary “OR “medical care”) NOT TOPIC: (embryo OR fetus OR infant OR newborn OR “bloodstream infection” OR “hospital infection” OR pneumonia OR sepsis OR “urinary tract infection”) AND LANGUAGE:(English) |
| Refined by: [excluding] DOCUMENT TYPES: (BOOK CHAPTER OR LETTER OR RETRACTED PUBLICATION OR EDITORIAL MATERIAL OR MEETING ABSTRACT) | ||
| Timespan: 2000–2017. Indexes: SCI-EXPANDED, SSCI, A&HCI, CPCI-S, CPCI-SSH, BKCI-S, BKCI-SSH, ESCI, CCR-EXPANDED, IC. |