
Abstract
Many enteric pathogens disproportionately infect children. Hospital discharge data can provide information on severe infections, including cost. However, the diagnosis must be recorded on the discharge record and coded accurately. We estimated the rate of underascertainment in hospital discharge data among children with culture-confirmed Campylobacter, Salmonella, and Escherichia coli O157 infections using linked laboratory and hospital discharge data from an integrated health care organization. We reviewed the International Classification of Diseases, 9th and 10th Revisions, Clinical Modification (ICD-9/10-CM) diagnosis codes on each patient's discharge record. We determined the percentage of patients who had a pathogen-specific diagnosis code (for Campylobacter, Salmonella, or E. coli O157) or nonspecific gastroenteritis code. We included the first admission or positive test and calculated the number of days between specimen submission (outpatient ≤7 days before admission or inpatient) and hospital discharge. Of 65 hospitalized children with culture-confirmed Campylobacter (n = 30), Salmonella (n = 24), or E. coli O157 (n = 11) infections, 55% had that pathogen-specific diagnosis code listed on the discharge record (79% Salmonella, 54% E. coli O157, 37% Campylobacter). The discharge records of the 35 children with a specimen submitted for culture ≥3 days before discharge were 16 times more likely to have a pathogen-specific diagnosis than the records of the 30 children with a specimen submitted <3 days before discharge (83% vs. 23%; odds ratio 15.9, 95% confidence interval: 4.7–53.8). Overall, 34% of records of children with culture-confirmed infection had ≥1 nonspecific gastroenteritis code (Campylobacter 43%, Salmonella 29%, E. coli O157 18%), including 59% of those for children without a pathogen-specific diagnosis (Campylobacter 63%; Salmonella 60%; E. coli O157 40%). This study showed that hospital discharge data under-ascertain enteric illnesses in children even when the infections are culture confirmed, especially for infections that usually have a short length of stay.
Many enteric pathogens disproportionately infect children (Scallan et al., 2013). Hospital discharge data can provide information on severe infections, including cost (Hoffmann et al., 2012). However, for an illness caused by a pathogen to be counted, not only must the physician consider the diagnosis and order appropriate diagnostic tests, but the diagnosis must be recorded on the discharge record and coded accurately. Our aim was to estimate the rate of under-ascertainment in hospital discharge data among children with culture-confirmed Campylobacter, Salmonella, and Escherichia coli O157 infections using data from the Marshfield Clinic Health System (MCHS), Wisconsin (Kieke et al., 2015).
Materials and Methods
Laboratory data (inpatient and outpatient) from Marshfield Clinic Labs was linked to hospital discharge data for children <18 years admitted to Marshfield Medical Center from 2004 to 2016 (2004–2013 for E. coli O157) using unique identification numbers. We reviewed patient discharge records to determine the percentage with an International Classification of Diseases, 9th and 10th Revisions, Clinical Modification (ICD-9/10-CM) diagnosis codes for typhoid or paratyphoid fever (ICD-9-CM: 002.0–002.9; ICD-10-CM: A01.00–A01.09, A01.1–A01.4) or other Salmonella infection (ICD-9-CM: 003.0–003.9; ICD-10-CM: A02.0–A02.9); Campylobacter (ICD-9-CM: 008.43; ICD-10-CM: A04.5); enterohemorrhagic or other/unspecified E. coli (ICD-9-CM: 008.00, 008.04, 008.09; ICD-10-CM: A04.3–4); HUS (ICD-9-CM: 283.11; ICD-10-CM: D59.3) or nonspecific gastroenteritis (ICD-9-CM: 008.8, intestinal infection due to other organism, not elsewhere classified; 009, ill-defined infectious gastroenteritis; 558.9, other and unspecified noninfectious gastroenteritis and colitis; 787.91, diarrhea; ICD-10-CM: A08.8, other specified intestinal infections; A09, infectious gastroenteritis and colitis, unspecified; K52.89, other specified noninfective gastroenteritis and colitis; K52.9, noninfective gastroenteritis and colitis, unspecified; R19.7 diarrhea, unspecified) (World Health Organization, 2019). We included the first admission or positive test and calculated the number of days between specimen submission (≤7 days before admission or inpatient) and hospital discharge. In a separate analysis, we queried electronic medical records from 2004 to 2016 to determine how frequently hospitalized children with a known intestinal infectious disease (ICD-9-CM: 001–008.6; ICD-10-CM: A00–A08.4) or nonspecific gastroenteritis submitted a stool sample for bacterial culture. We used SAS version 9.3 (SAS Institute, Cary, NC). We used the chi-square test to test statistical significance between categorical variables. We calculated odds ratios and 95% confidence intervals (CI) to quantify the relationship between having a pathogen-specific diagnosis and the number of days from specimen submission to discharge. MCHS's Institutional Review Board approved the study.
Results
We identified 65 hospitalized children with culture-confirmed Campylobacter (n = 30), Salmonella (n = 24), or E. coli O157 (n = 11) infections. Of these, 55% had that pathogen-specific diagnosis code on the discharge record (79% Salmonella, 54% E. coli O157, 37% Campylobacter), including 31% as the primary diagnosis (Salmonella 46%, Campylobacter 23%, E. coli O157 18%). The discharge records of the 35 children with a specimen submitted for culture ≥3 days before discharge were 16 times more likely to have a pathogen-specific diagnosis than the records of the 30 children with a specimen submitted <3 days before discharge (83% vs. 23%; odds ratio 15.9, 95% CI: 4.7–53.8) (Fig. 1).
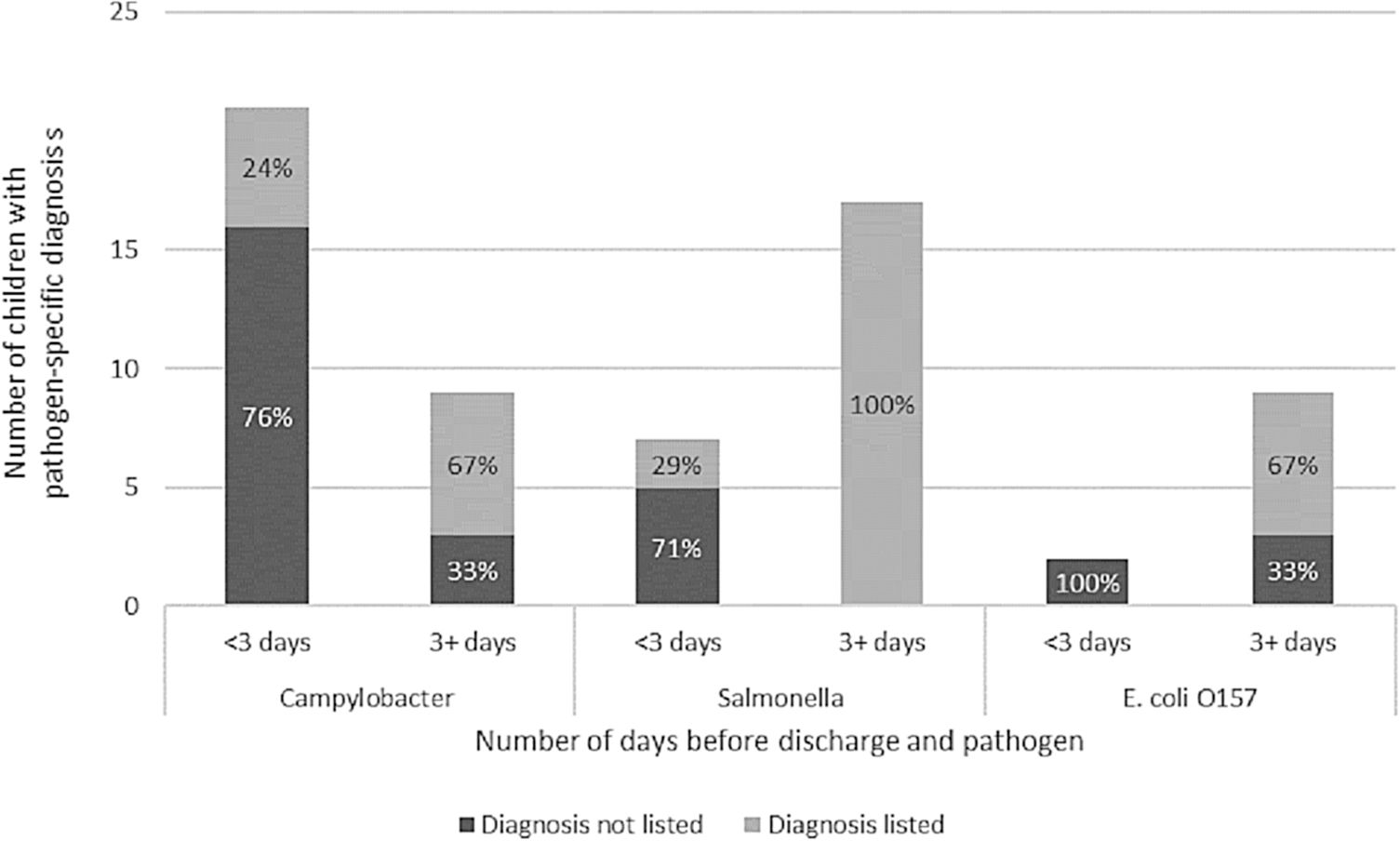
Number and percentage of hospitalized children (patients <18 years) with culture-confirmed Campylobacter, Salmonella, or Escherichia coli O157 infection who submitted a specimen for bacterial culture <3 days and ≥3 days before discharge* from hospital and the percentage of these children who had the culture-confirmed pathogen-specific diagnosis listed as an ICD-9-CM diagnosis code on the hospital discharge record, Marshfield Medical Center, Marshfield, Wisconsin, January 1, 2004–December 31, 2014 (January 1, 2004–December 31, 2013 for E. coli O157). *We chose this number because it takes on average 3–4 days for a positive result to be obtained in this hospital system (Personal communication, Thomas Fritsche, Marshfield Labs). The average number of days between specimen submission and hospital discharge was 6.7 for the 36 children who had the pathogen-specific diagnosis listed on the discharge record compared with 2.1 days for the 29 children without that pathogen-specific diagnosis listed (p < 0.05). ICD-9-CM, International Classification of Diseases, 9th Revisions, Clinical Modification.
Overall, 34% of the records of children with culture-confirmed infection had ≥1 nonspecific gastroenteritis code (Campylobacter 43%, Salmonella 29%, E. coli O157 18%), including 59% of those for children without a pathogen-specific diagnosis (Campylobacter 63%; Salmonella 60%; E. coli O157 40%). Records of seven children with E. coli O157 infection had HUS listed; five as the primary diagnosis. Among 12 records of children with culture-confirmed infections who had neither a pathogen-specific nor a nonspecific gastroenteritis code, the primary code was HUS (n = 3), intussusception (n = 3), another infectious intestinal disease (cryptosporidiosis, Clostridium difficile) (n = 2), disorders of fluid electrolyte and acid–base balance (n = 1), regional enteritis (n = 1), or an illness feature (n = 2; fever, nausea/vomiting).
Overall, 40% (351/882) of hospitalized children with a discharge code for infectious intestinal disease, nonspecific gastroenteritis, or both had a stool sample submitted for bacterial culture.
Discussion
This analysis indicates that hospital discharge data can under-ascertain bacterial enteric infections in children even when they are culture confirmed. Moreover, many children with an infectious intestinal disease or nonspecific gastroenteritis diagnosis code may not have a stool culture.
Just more than half of children with culture-confirmed Salmonella, Campylobacter, or E. coli O157 infections had that pathogen-specific diagnosis listed on the hospital discharge record. This percentage was higher than among adults (55% vs. 46%) (Scallan et al., 2018). Compared with adults, children with Salmonella and E. coli O157 infections were more likely, and children with Campylobacter were less likely, to have that that pathogen-specific diagnosis listed. Among children, a Salmonella code was 2.3 times more likely than a Campylobacter code to be listed on the discharge record; it was only 1.3 times more likely among adults.
The strong association between having the pathogen-specific diagnosis and a longer time between specimen submission and hospital discharge likely accounts for much of the difference in reporting rates between Salmonella and Campylobacter because Campylobacter patients had the shortest median length of stay. This might reflect the fact that the laboratory testing was not completed at the time discharge billing codes were assigned or that the laboratory report was not yet included in the patient record. However, almost one-fifth of records of children who submitted a specimen ≥3 days before discharge also did not have the pathogen-specific diagnosis, indicating that there are likely other reasons.
MCHS provides care to a largely rural population that may not be representative of the U.S. population. It is not known how coding or laboratory practices of the clinic compare with others. Our analysis was limited to three pathogens. Underdiagnosis may be more common than assessed, particularly among vulnerable persons in whom dehydration or electrolyte imbalance may exacerbate a chronic illness, resulting in hospitalization after resolution of the gastrointestinal illness.
Conclusions
The findings of this study can be used to improve estimates of the burden of foodborne and enteric illnesses. Hospital discharge data are likely to underestimate hospitalizations caused by enteric pathogens, particularly for infections that usually have a short length of stay. This has implications for studies that use hospital stay to estimate costs: the use of only pathogen-specific codes might result in overestimation of costs, because longer stays are more likely to receive a pathogen-specific code.
Disclaimer
The contents of the article are solely the responsibility of the authors and do not necessarily represent the official views of CDC or the Department of Health and Human Services.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This article was 100% funded with federal funds from a federal program of $131,270. This article was supported by Cooperative Agreement No. 5NU60OE000103 funded by the Centers for Disease Control and Prevention.