
Abstract
Aeromonas dhakensis is an important ubiquitous Gram-negative and freshwater bacterium detected in different reservoirs. It can cause invasive diseases in humans. Herein, we report the first case in Mainland China of a fulminant death of a 29-year-old man as a result of a new, unexpected association between septicemic A. dhakensis and hepatitis B viral infection (HBV). Herein, the patient died from multiple organ failure 5 d postadmission after the ingestion of Snakehead Fish meal. The isolated bacterium was initially misidentified as Aeromonas hydrophila using VITEK-2, while whole-genome sequencing (WGS) revealed that the isolate is A. dhakensis. WGS revealed the occurrence of three antimicrobial genes of resistance: imiH, cphA2, and bla OXA-12; besides, major virulence factors were detected. In silico, multilocus sequence typing (MLST) showed that our A. dhakensis 17FW001 belonged to a novel sequence type (ST557). A comparative genomic analysis of our isolate with nine selected Aeromonas species was done, which elucidated the pathogenicity of our A. dhakensis. In conclusion, we reported for the first time the association between A. dhakensis and HBV in Mainland China. We revealed that septicemic A. dhakensis could result in severe adverse clinical outcomes that end up with unexpected fulminant death especially when it is accompanied with HBV and sheds light on the virulence of A. dhakensis and the high rate of its misdiagnosis that requires to urgently consider screening of all cases of A. dhakensis for HBV in the future. Besides, caution should be taken while dealing with snakeheads which act as a vector for A. dhakensis.
Introduction
The Gram-negative Aeromonas dhakensis is detected in different reservoirs, mainly in aquatic environments, including rivers and lakes, besides domestic sewage and drinking water, as well as various kinds of food and birds (Figueras et al., 2009; Aravena-Roman et al., 2011; Chen et al., 2014).
A. dhakensis was isolated for the first time from the feces of children suffering from diarrhea in Dhaka, Bangladesh (Huys et al., 2002). Later, it has been isolated from human feces, clinical sources, and diseased fish or environmental water (Carriero et al., 2016). It has been reported that A. dhakensis can cause invasive diseases in humans, ranging from mild gastroenteritis to fatal bloodstream infections; the prevalence of clinical infections caused by A. dhakensis is underestimated because it is frequently misidentified as Aeromonas hydrophila by the current phenotype-based identification system (Chen et al., 2016; Chang et al., 2018; Kitagawa et al., 2020).
Snakeheads (Channidae) represent a group of highly predatory freshwater fishes. They are vulnerable to bacterial infections leading to high mortality and economic loss (Samayanpaulraj et al., 2019).
Hepatitis B viral infection (HBV), as a significant public health threat, was found to be endemic in China and capable of causing liver cirrhosis (Tada et al., 2018). Among the 350 million individuals worldwide infected with HBV, it was found that one-third of them were residing in China (Custer et al., 2004) that requires precise monitoring, especially in patients infected with septicemic A. dhakensis. In the present study, we revealed that septicemic A. dhakensis could result in a progressive multiple organ failure that ends up with fulminant death, especially when HBV accompanies it. Besides, caution should be taken while dealing with snakeheads, which act as a vector for A. dhakensis.
Materials and Methods
Bacterial isolation and identification
This case study was conducted on an A. dhakensis strain isolated from the venous blood of a 29-year-old male who was admitted to the Fifth affiliated hospital, Sun Yat-sen University, Guangdong Province, China. The isolate was initially identified using VITEK 2 GN (bioMérieux Vitek, Inc.) identification card and biochemical tests. Then the taxonomic affiliation was determined using the whole-genome sequence analysis (Richter et al., 2016). All the clinical details of the patient were collected from the hospital medical records.
Ethics statement
The experimental procedures were approved by the Medical Ethics Committee of the Fifth Affiliated Hospital of Sun Yat-sen University, Guangzhou, China; besides, informed consent was obtained from patients' relatives when data were collected.
Minimum inhibitory concentrations
In vitro antimicrobial susceptibility of our A. dhakensis was initially determined by VITEK2 automated system using AST-16 Gram-negative susceptibility card. Minimum inhibitory concentrations (MICs) were then detected by the broth microdilution method and interpreted according to the breakpoints of the Clinical and Laboratory Standards Institute (CLSI 2017) guidelines for 16 different antimicrobial agents (Table 1). For Tigecycline, MIC was evaluated according to the European Committee on Susceptibility Testing guidelines (version 1.3, 2010; Basel, Switzerland).
Antibiotic Susceptibility Test and Minimum Inhibitory Concentrations for Aeromonas dhakensis 17FW001
MIC, minimum inhibitory concentration.
Bioinformatics analysis
The whole genome of the strain was sequenced, and the resulting draft genomes were described. The genome DNA of our A. dhakensis was extracted using Qiagen Blood & Tissue Kit (Qiagen, Hilden, Germany), and DNA libraries were constructed with 350-bp paired-end fragments. A total of 5,329,626 paired-end 150 bp reads were produced by Illumina HiSeq2000 platform. Reads were assembled using SOAPdenovo. The genome annotation was performed using Rapid Annotations Subsystems Technology (Overbeek et al., 2014).
The taxonomic affiliation was determined using the average nucleotide identity (ANI) based on BLAST+ calculation (ANIb) and Tetra-nucleotide signature correlation index using JSpecies Web Server (JSpace WS) with default parameters (Richter et al., 2016).
A comparative genomic analysis was performed using the genome accessions of our A. dhakensis strain, A. dhakensis AAK1 (NZ_BAFL00000000), A. dhakensis strain CIP 107500 (NZ_CDBH00000000), A. dhakensis strain CECT 7289 (NZ_CDBP00000000), A. dhakensis strain F2S2-1 (NZ_LZFM00000000), A. dhakensis strain SSU (NZ_JDWD00000000), A. dhakensis strain Cr1 (NZ_LBDI00000000), A. dhakensis strain Cr2 (NZ_LBDJ00000000), A. hydrophila ATCC 7966, and A. dhakensis KN-Mc-6U21, where antimicrobial resistance genes were identified using the Comprehensive Antibiotic Resistance Database (CARD;
In silico MLST was performed by MLST 2.0 (
Galleria mellonella virulence assay
The virulence of our A. dhakensis strain was determined using the wax moth (Galleria mellonella) larvae model as previously described (Silver et al., 2011). Briefly, A. dhakensis 17FW001 was grown overnight at 37°C in Lysogeny broth (LB); then the bacteria from the mid-log phase were harvested by centrifugation. Ten millimolar MgSO4 were used to resuspend and standardize the bacteria to an OD600 of 0.6. Seven 10-fold serial dilutions were prepared for the assay and the inoculum determined by plating on LB agar and incubating overnight at 37°C. G. mellonella strains were provided by the Huiyude BioTechnology limited, China. G. mellonella larvae were placed in a Petri dish and kept on ice to keep worms stationary during the injection. A 10 μL Hamilton syringe (model number 701RN) was used to inject 5 μL from each dilution into the left hindmost proleg of the larvae. In between injections the Hamilton syringes were sterilized with 70% EtOH and washed with 10 mM MgSO4. Ten larvae were used per dilution. Aeromonas veronii (ATCC 35624) was used as a reference strain, and larvae inoculated with 10 mM MgSO4 were used as a control. The experiments were conducted in duplicate.
Case Report and Results
A 29-year-old man was admitted to the Fifth affiliated hospital of Sun Yat-sen University on April 17, 2017, complaining of 2 d fever (up to 39°C) with progressive diarrhea after ingestion of a meal of raw snakehead fish and being pricked by the fish fins on his left leg 2 d preadmission.
On admission, the patient was alert showing scleral icterus. Initial physical examination revealed that his pulse rate was 120 beats/min, respiratory rate 18/min, temperature 37.5°C, and blood pressure 127/55 mmHg. Mild pitting edema on both lower extremities and scrotal swelling were detected. No skin lesions were observed. Two sets of blood cultures were collected. Laboratory findings on admission showed that white blood cell count was 16.22 × 109/mL (86.70% neutrophils), C-reactive protein 41.57 mg/L, alanine aminotransferase (ALT) 103.00 U/L, aspartate aminotransferase (AST) 192.00 U/L, total bilirubin 127.80 μM, direct bilirubin 75.60 μM, and international normalized ratio (INR) 3.89 (Table 2). Examination of the lung with a computed tomographic scan revealed the absence of any abnormalities.
The Patient's Arterial Blood Gas Analysis and Laboratory Findings on Admission
Intravenous ceftriaxone (2.0 g qd) as an empirical antimicrobial therapy was immediately administered. Three hours after admission, the patient suddenly developed septic shock. Repeat laboratory investigations revealed the following: Blood pressure was 78/37 mmHg, INR 3.89, procalcitonin 47.62 ng/mL, albumin 24.90 g/L, prothrombin time 42.80 s, and activated partial thromboplastin time 67.50 s (Table 2). To promptly control the patient's deteriorated condition, the original antibiotic regime was changed to intravenous meropenem (1.0 g q8h) besides other supportive treatments for his refractory septic shock, such as infusion of plasma, liver protection, vasopressor agent, methylprednisolone (40 mg qd), and high-flow oxygen therapy, however; the septic shock was not improved.
On the second day of admission, the patient was transferred to the intensive care unit (ICU) for hemodialysis and hemodynamic monitoring and was administered methylprednisolone (500 mg qd). Few hours following his admission to ICU a progressive multiple organ failure, including liver, heart, lung, and incurable acidosis successively, was developed beside the appearance of scattered ecchymosis on his left leg (Fig. 1). X-ray examination revealed that lungs were rough and blurry, their permeability was reduced, the density was increased, and there were many patches in the lungs, with blurred edges (Fig. 2). An initial culture from the venous blood sample revealed Gram-negative bacilli.
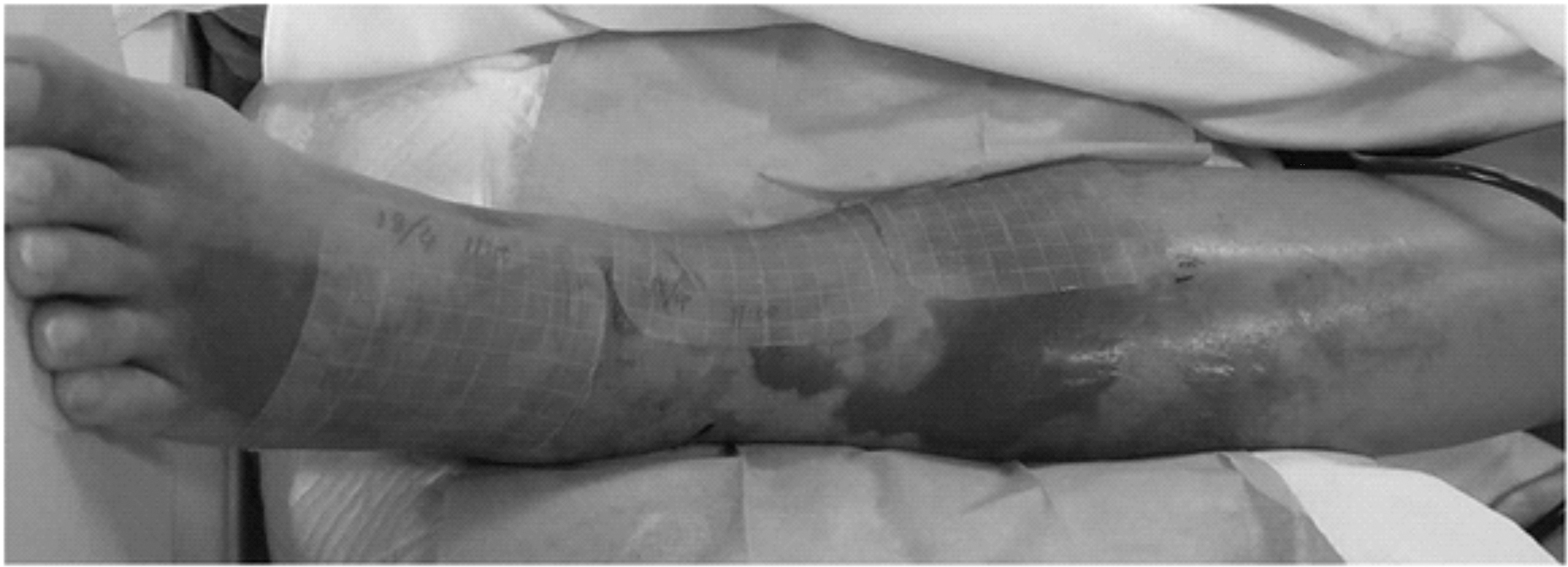
The swelling and scattered ecchymosis on the right extremity appeared on the second day of admission.
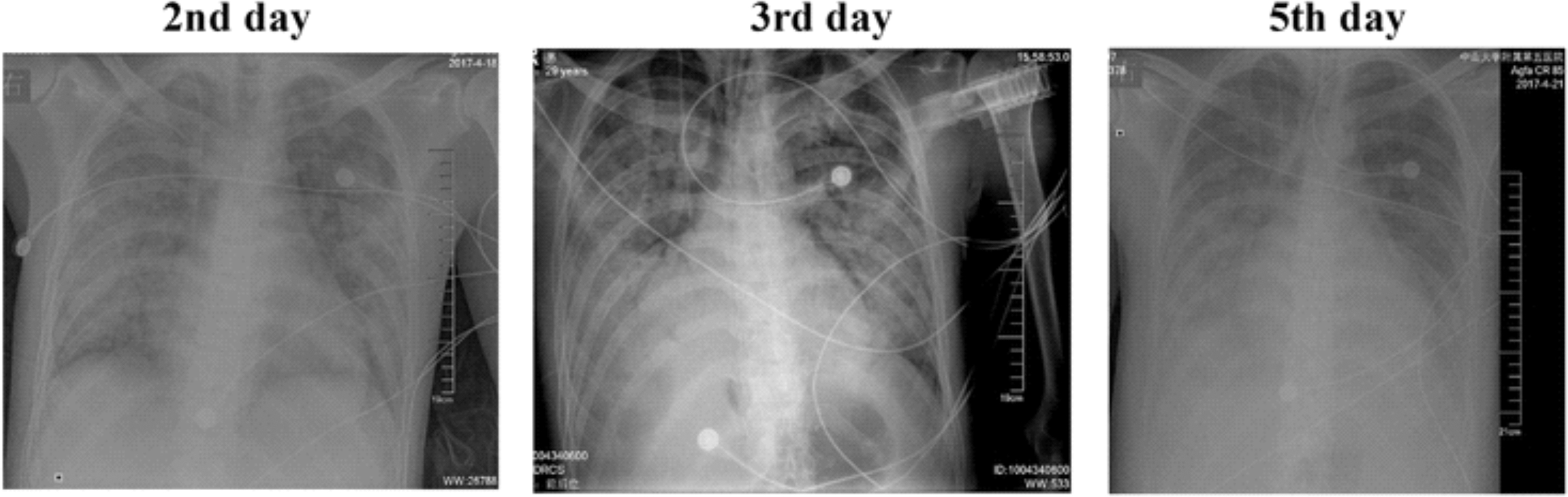
The field texture of lungs was rough and blurry, the permeability was reduced, the density was increased, and there were many patches in the lungs, and the edges were blurred.
Diagnosis of HBV was established on the serological evidence, showing positive results for HBsAg, HBeAg, and IgG anti-HBc. On the third day of admission, the quantity of HBV DNA level was estimated to be 1.54978 × 105 IU/mL using quantitative reverse transcription polymerase chain reaction (Roche COBAS Amplicon) indicating active viral replication that requires the administration of an antiviral agent such as tenofovir or entecavir. However, our patient did not receive antiviral agent since the patient was in somnolence while being diagnosed as an HBV-infected patient on the second day of admission. Generally, in our hospital, anti-HBV medicine is usually administered orally and is slow-working medicine. Therefore, the antiviral therapy was postponed in our case until septic shock was reversed, and the patient becomes conscious.
On the fourth day of admission, the isolated bacterium was misidentified as A. hydrophila using biochemical tests and GN card of VITEK-2 (bioMerieux Vitek, Inc.). The taxonomic affiliation using the whole-genome sequencing (WGS) analysis revealed that our isolate has 97.1% ANI and 0.9999 ANI Z-score resemblance to A. dhakensis F2S2-1 and was named as A. dhakensis 17FW001 (Supplementary Table S1). The genome size was 4,668,072 bp, and GC content was 61.9%. This Whole-Genome Shotgun project has been deposited at DDBJ/ENA/GenBank under the accession QUOJ00000000 with BioSample identification SAMN09770288.
Antimicrobial susceptibility results by the VITEK-2 system showed that our A. dhakensis 17FW001 was susceptible for all tested antibiotics except cefazolin, ampicillin, and ampicillin/sulbactam (Table 1). MIC determination revealed that our A. dhakensis 17FW001 was sensitive to all tested antibiotics except ampicillin, colistin, and polymyxin B (Table 1).
The patient's case still deteriorated; therefore, more resuscitative measures, including red cell transfusion, mechanical ventilation, and a large dose of methylprednisolone for pulse therapy, were taken. Despite all intensive supportive efforts, the patient died 5 d postadmission.
Antimicrobial resistance genes were identified using the CARD database, where three antibiotic resistance genes imiH, cphA2, and bla OXA-12 were detected.
Virulence factors were screened using VFDB, where different virulence factors related to the pathogenicity of A. dhakensis were detected, including the toxin factors, aerA/act, ahh1, hlyA beside the T6SS secretion system, and many other adherence factors such as flaA and flaB (Supplementary Table S2), which may play a role in the rapid deterioration of the case.
The comparative genomic analysis of our A. dhakensis 17FW001 elucidated the pathogenicity of our strain by identifying different virulence factors that may play a vital role in the bacterial pathogenicity (Supplementary Table S2).
MLST analysis of A. dhakensis 17FW001 revealed that it belonged to a novel sequence type (ST557) and was deposited in the PubMLST database (
To correlate the bacterial virulence with the rapid deterioration of the patient's condition, a virulence evaluation was conducted using the G. mellonella as a model. In the virulence assays, the survival of G. mellonella infected by A. dhakensis 17FW001 and A. veronii (ATCC 35624) was observed for 24 h. The survival rates of the groups injected by A. dhakensis within the 24 h showed a similar survival rate with that of A. veronii (ATCC35624), where the survival rate was 80% in the two groups injected by A. dhakensis and A. veronii at 107 colony forming unit (CFU) (Table 3). Indeed, the A. dhakensis 17FW001 strain did not reveal more virulence compared to the reference strain A. veronii (ATCC35624).
Twenty-Four Hour Survivals of Galleria mellonella Infected with Aeromonas Stains
Discussion
Although the genus Aeromonas includes a large number of species, only a few of them represent the pathogens of fish and warm-blooded animals, including humans (Piotrowska and Popowska, 2015). In our study, the initial identification was performed using the VITEK-2 automated identification system, which identified the strain successfully to the genus level. However, the VITEK-2 system misidentified the species of the isolate, which was identified falsely as A. hydrophila. In this context, it has been reported that the genus Aeromonas includes strains that are difficult to be differentiated from one another by the phenotypic methods (Carriero et al., 2016). Besides, Kitagawa et al. (2020) have reported that A. dhakensis is often misidentified as A. hydrophila, A. veronii, or Aeromonas caviae by commercial phenotypic tests. Thus, herein, we further identified our isolate by WGS analysis using the ANI by JSpecies, which confirmed that our strain was A. dhakensis, revealing that the VITEK-2 identification system was incapable of differentiating between A. hydrophila and A. dhakensis. This emphasizes the findings of other studies, where the usage of VITEK for the identification of Aeromonas spp. was unreliable, where it identified most of Aeromonas spp. as belonging to the species A. hydrophila resulting in an underestimation of the occurrence of A. dhakensis (Abbott et al., 2003; Chen et al., 2016; Chang et al., 2018).
The antimicrobial susceptibility profile of our A. dhakensis 17FW001 strain was obtained by performing both of the broth microdilution method and VITEK-2 system, which revealed the susceptibility of A. dhakensis 17FW001 to all tested antibiotics except cefazolin, ampicillin, ampicillin/sulbactam, colistin, and polymyxin B. The resistance to ampicillin and ampicillin/sulbactam was predictable, as most species of this genus are already known to be resistant to aminopenicillins (Abbott et al., 2003).
It has been reported that antimicrobial resistance of A. dhakensis to broad-spectrum cephalosporins or carbapenems is not widespread although it intrinsically harbors class-B Metallo-β-lactamases, CphA, and class-D-beta-lactamases (oxacillinases). The conventional susceptibility test does not easily detect CphA carbapenemase unless large inoculum is used (Chen et al., 2016). In our study, meropenem susceptibility was determined with both standard and large inocula of 104 and 108 CFU per spot according to the breakpoints of the CLSI, 2017, which adopted the same interpretative results of susceptibility for meropenem.
HBV inducing chronic liver inflammation and liver cell damage have been reported in several studies (Custer et al., 2004; Tada et al., 2018). Besides, it was reported that T cell inhibition is more profound within the liver than in the circulation, and its severity was found to be increased in the presence of high HBV levels (Fisicaro et al., 2012). In this context, a previous study reported that immunocompromised conditions could serve as essential factors of Aeromonas septicemia and hepatobiliary infections (Morinaga et al., 2011). Besides, it has been reported that A. dhakensis is the principal species causing septicemia and more lethal than other Aeromonas species, especially among cirrhotic liver patients (Chen et al., 2016; Kitagawa et al., 2020). Herein, the patient did not know about his HBV until his admission and performing the serological examinations and other liver function tests. We have postulated that the impairment of his liver function tests may be attributed to HBV and that the septicemic infection with A. dhakensis 17FW001 accelerated the rate of his liver deterioration. Therefore, we concluded that it is urgent to consider the probability of liver damage in patients with A. dhakensis septicemia.
Moreover, several studies reported that A. dhakensis exhibits higher pathogenicity than A. hydrophila and that it had the highest mortality rate and was an independent risk factor for mortality where deaths occurred within 14 d from septicemia (Wu et al., 2015; Sinclair et al., 2016). In the present study, the patient died from multiple organ failure 5 d postadmission despite all intensive supportive efforts.
In addition, several studies reported the presence of different virulence genes, which contribute to developing various infectious diseases. Besides, the virulence of A. dhakensis has been reported as the most potent among members of the genus Aeromonas resulting in the most cytotoxicity to human blood cell lines (Figueras et al., 2009; Chen et al., 2016). In our study, virulence factors were screened using Virulence Factors Database, where different virulence factors related to the pathogenicity of A. dhakensis were detected, including the toxin factors, aerA/act, ahh1, hlyA besides the T6SS secretion system, and many other adherence factors such as flaA and flaB (Supplementary Table S2), which may play a role in the rapid deterioration of the case. Besides, a virulence evaluation was conducted using the G. mellonella as a model to correlate the bacterial virulence with the rapid deterioration of the patient's condition. However, the A. dhakensis 17FW001 strain did not show more virulence compared to the reference strain A. veronii (ATCC35624) that probably confirms our postulation that the association between A. dhakensis 17FW001 and HBV in our patient was perhaps the cause of the multiple organ failure that ended up with the unexpected fulminant death.
Snakehead fishes are related to two known genera, namely the African Parachanna and the Asian Channa, with 27 different extant species (Musikasinthorn and Taki, 2001). Herein, the patient died from a progressive multiple organ failure 5 d postadmission after the ingestion of Snakehead Fish meal. In this context, it has been reported that Aeromonas spp. is widely distributed in Northern snakehead intestine (Channa argus) in China and have considerable virulence potential (Zhang et al., 2019).
Eventually, the failure of the administered antibiotics to save the patient's life has directed us to try to find out the reasonable cause behind the death of the patient. According to our worm virulence experiments, we found that our A. dhakensis 17FW001 strain did not show more virulence compared to the reference strain A. veronii (ATCC35624); besides, previous reports revealed that Aeromonas spp. is more likely to cause adverse clinical outcomes in patients with liver fibrosis and impaired liver function (Custer et al., 2004; Tada et al., 2018). Thus, we concluded that the HBV and the elevations of AST and ALT levels with the septicemic A. dhakensis 17FW001 were the culprits. Regrettably, since the patient has died in a short period, it was impossible to judge whether the defect of immune function or the immune hyperstimulation caused the final adverse outcome, which might require medicines regulating the immune function besides the antimicrobial agents.
Conclusions
We reported for the first time in Mainland China a fatal case of septicemic A. dhakensis with HBV and shed light on the urgent need for reevaluating the role of A. dhakensis as a serious pathogen after the changing taxonomy. In addition, septicemic Aeromonas infected patients should be promptly checked whether they are known-infected patients with HBV or not, to prescribe the proper therapy from the beginning to minimize the rapid liver deterioration, which leads to the progress of the case into multiple organ failure. Besides, caution should be taken while dealing with snakeheads, which serve as a vector for A. dhakensis. We aim that our study may serve as an alarm to clinicians to pay special care for patients with Aeromonas infections with impaired liver function and to take early intervention measures to reduce the probability of adverse outcomes.
Authors' Contributions
All authors contributed to the study conception and design. Collection and clinical analysis of the sample were performed by M.H., H.C., C.L., and C.G. Material preparation, performing experiments, and assistance in whole-genome sequence analysis were performed by Y.L. and M.A.E.-G.E.-S.A. The first draft of the article was written by M.H., Y.L., and M.A.E.-G.E.-S.A. The final article was written by M.A.E.-G.E.-S.A., and all authors commented on previous versions of the article. The whole-genome sequence analysis and the susceptibility testing were performed by
All authors read and approved the final article.
Footnotes
Disclosure Statement
No competing financial interests exist.
Funding Information
This work was supported by grants from the National Key R&D Program of China (No. 31010304-2016035).
Supplementary Material
Supplementary Table S1
Supplementary Table S2
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.