
Abstract
In Canada, enteric infections cause significant health and economic burden. We evaluated the individual characteristics of laboratory-confirmed cases of Campylobacter spp. (n = 28,728), non-typhoidal Salmonella spp. (n = 22,640), Yersinia spp. (n = 1674), Verotoxin-producing Escherichia coli (VTEC; n = 1340), and Listeria monocytogenes (n = 471), reported between 2010 and 2017 inclusive, in Ontario, Canada (population ∼13,500,000). We calculated overall and pathogen-specific annual and mean incidence rates (IRs) for Ontario. We used multivariable Poisson and negative binomial regression models to estimate incidence rate ratios (IRRs) for years, seasons, age groups, and sexes, and we included two-way age and sex interaction terms in the models. Campylobacter and Salmonella infections had the highest IRs whereas Listeria infections had the lowest IRs. None of the infections showed long-term trends over the 8-year study period; however, rates of all five infections were elevated in the summer. More Salmonella, VTEC, and Listeria infections were linked to disease outbreaks than were Campylobacter and Yersinia infections. Overall, mean IRs of Campylobacter, Salmonella, Yersinia, and VTEC infections were highest in children 0–4 years old, whereas Listeria IRs peaked in adults 60 years and older. Higher mean IRs of Campylobacter were observed in males. No other differences by sex were statistically significant. The same mean rate was observed in both sexes for Listeria. Adjusting for all other factors, significant age- and sex-specific differences in IRs were observed in Campylobacter, Salmonella, and VTEC infection rates. No significant interactions of age and sex were found for Yersinia and Listeria infections. Future research should focus on the pathogen-specific socioeconomic, environmental, or agricultural risk factors that might be responsible for these infections.
Introduction
In Canada, enteric infections cause significant health (Thomas et al., 2017; Drudge et al., 2019) and economic (Majowicz et al., 2006, 2011; Thomas et al., 2015b) burden. Among the leading causes are Campylobacter spp., non-typhoidal Salmonella spp., Yersinia spp., Verotoxin-producing Escherichia coli (VTEC), and Listeria monocytogenes, with L. monocytogenes causing the highest mortality rate (Thomas et al., 2013, 2015a; Drudge et al., 2019).
Canadian studies examining enteric disease distributions, and related sociodemographic factors, in Manitoba (Green et al., 2006), Northwest Territories (Pardhan-Ali et al., 2012), Alberta (Pearl et al., 2006), New Brunswick (Valcour et al., 2016), and Ontario (Michel et al., 1999; Varga et al., 2013a, 2013b, 2020, 2021; Paphitis et al., 2020), showed temporal, seasonal, and demographic variations in rates of Salmonella and VTEC infections, with higher rates observed mostly in children 0–4 years old and in summer.
However, research studies on the incidence rate (IR) distributions and risk factors for other infections (e.g., Listeria, Yersinia infections) have not been conducted. Given that enteric disease patterns are pathogen-specific (Drudge et al., 2019), and vary due to individual- and area-level factors such as sociodemographic, environmental, and neighborhood characteristics (White et al., 2011; Arsenault et al., 2012; Daoud et al., 2017), our objectives were to: (1) examine and compare overall and pathogen-specific crude IRs by year, season, age, and sex, and (2) examine pathogen-specific yearly and monthly trends, of Campylobacter, Salmonella, Yersinia, VTEC, and Listeria infections in Ontario, Canada, reported from January 1, 2010, to December 31, 2017, inclusive.
Methods
Study area and population
Ontario is Canada's most populous province (13,448,494 inhabitants; ∼40% of the Canadian population) (Statistics Canada, 2017) with the third-largest land area (917,741 km2) (Statistics Canada, 2020). Ontario has two primary regions: Northern Ontario contains about 6% of Ontario's population across 88% of the total land area, whereas southern Ontario is more densely populated (94% of Ontario's population) (Statistics Canada, 2017, 2020).
Ontario is divided into 35 local public health unit (PHU) areas. The PHUs are local government health agencies established by one or more municipalities to deliver health promotion and disease prevention programs (MOHLTC, 2020). Importantly, Ontario has the most farms (including fruit and cash crops as well as poultry, dairy, and beef cattle) among Canadian provinces. About 95% of the cattle in Ontario are in southern Ontario (OMAFRA, 2021), and most are concentrated in the southwestern region with some in central and eastern Ontario (Government of Ontario, 2019).
Case data
Under Ontario's Health Protection and Promotion Act (Government of Ontario, 2020), private and public health laboratories are required to report several infectious diseases, including the five pathogens being examined in this investigation, to local PHUs. Disease data are managed in Ontario's Ministry of Health and Long-term Care's (MOHLTC) integrated Public Health Information System (iPHIS) surveillance database using standard case definitions (MOHLTC, 2019).
We obtained data on all cases of Campylobacter, Salmonella, Yersinia, VTEC, and Listeria, reported in Ontario with episode dates from January 1, 2010, to December 31, 2017 inclusive, via a request to Public Health Ontario (the provincial public health organization). This study was approved by a University of Waterloo Research Ethics Committee (ORE No. 40133).
Each case included the date of disease onset, 5-year age category, sex, PHU of residence, and whether the case was domestic versus travel-acquired, and sporadic versus outbreak-associated. A case is considered travel-related if out-of-province travel occurred within the disease incubation period. In these data, the month and calendar year of occurrence were used as the disease onset date. When these were not available, the earliest of the sample collection date or the date the case was reported was used as a proxy.
Analysis
Data were compiled in Excel 2013 (Microsoft Corporation, Redmond, WA), and checked for missing observations. Data for four (year, age, PHU, and link to outbreaks) of the six variables were 100% complete, whereas both sex and travel status had missing observations (Table 1). For sex, 0.64% of the data had missing observations and these were excluded from sex-specific IR determinations. For travel status, only 58.6% of the cases had valid data and in one of the years (2010), travel was not reported. We, therefore, only included travel in our descriptive analysis.
Annual, Seasonal, and Demographic Distributions, and the Proportion Related to Travel and Outbreaks, of the 54,853 Cases of 5 Enteric Diseases Reported in Ontario, Canada (2010–2017)
Cases excluded from sex-specific IR determinations.
Indicates that travel information was not available for reporting in iPHIS (applies to cases reported in 2010).
iPHIS, integrated Public Health Information System; IR, incidence rate.
Cases were descriptively analyzed by using Stata version 14.2 (StataCorp, LLC, College Station, TX) and Excel 2013. We used seven age categories (Table 1), as guided by previous studies (Vrbova et al., 2012; Varga et al., 2013b; Barkley et al., 2016), and aggregated cases monthly and seasonally, where season was classified as winter (January, February, and March), spring (April, May, and June), summer (July, August, and September), or fall (October, November, and December).
Overall and group-specific annual and mean IRs per 100,000 person-years, and monthly IRs per 100,000 person-months were calculated (Dohoo et al., 2012). Denominators for the IR calculations were the annual inter-censal population estimates (overall, by age and sex) based on the 2016 Census (Statistics Canada, 2019). For this study, we defined a long-term trend as an increase or a decrease in IRs for 5 consecutive years or longer. For each pathogen, monthly IRs with 3-month moving averages were charted in Excel, as were the average IRs across the 8 years.
To compare annual IRs and identify significant demographic and seasonal factors, we built five separate multivariable Poisson regression models for each pathogen. The dependent variable was the total number of cases. Independent variables were year, season, age group, and sex. The population estimates for each covariate pattern were used as the offset variable. Incidence rate ratios (IRRs) and their corresponding 95% confidence intervals and p-values were estimated. The IRR was the IR of the category of interest compared with the IR of the reference category (the category with the lowest IR).
To determine whether the effect of age group on infection rates varied between males and females, two-way interaction terms were introduced in the models. However, no significant interactions of age and sex were found for Yersinia and Listeria; therefore, the interactions were excluded from these models. The overall fit of each model was assessed for over-dispersion by using the deviance and Pearson χ2 goodness-of-fit tests (Dohoo et al., 2012).
The Poisson models for all the pathogens, except Listeria, indicated a significant lack of fit (over-dispersion), since χ2 was significant at p < 0.05. Negative binomial models were, therefore, estimated for Campylobacter, Salmonella, Yersinia, and VTEC. We also compared the models by using Akaike's Information Criteria (AIC) and the Bayesian Information Criteria (BIC). The model with the lower index indicated a better fit for analysis.
Results
From 2010 to 2017, 54,853 laboratory-confirmed cases of Campylobacter (28,728; 52.4%), Salmonella (22,640; 41.3%), Yersinia (1674; 3.1%), VTEC (1340; 2.4%), and Listeria (471; 0.9%) were reported.
Of the five Campylobacter spp. identified and reported, Campylobacter jejuni (14,387/28,728; 57.2%), C. jejuni/coli (10,275/28,728; 40.8%), and Campylobacter coli (495/28,728; 2.0%) predominated. Of the 63 Salmonella serotypes reported, Salmonella Enteriditis (7946/22,640; 57.6%), Salmonella Typhimurium (2544/22,640; 18.4%), Salmonella Heidelberg (2228/22,640; 16.1%), and Salmonella Thompson (1088/22,640; 7.9%) predominated. The majority (1490/1674; 89%) of Yersinia spp. reported were Yersinia enterocolitica. All reported E. coli strains were VTEC (with no differentiation between O157 and non-O157 serotypes), and all reported Listeria spp. were L. monocytogenes.
The distribution of cases by pathogen, year, season, age, sex, travel, and outbreak status is given in Table 1. Campylobacter and Salmonella infections comprised 94% of all cases. Cases of Yersinia, VTEC, and Listeria were considerably lower, with Listeria cases constituting only 0.9% of all cases. No long-term annual trends in cases over time were observed, except for Listeria cases that peaked in 2016 (96; 20.4%). However, all infections peaked in July/August (Fig. 1). Overall, people 40–49 and ≥60 years made up 45% of all cases. There were more reported infections in males (52.1%) than in females (47.9%). Salmonella (25.2%) and Yersinia (21.4%) had the most travel-related cases, whereas VTEC (15.8%) and Listeria (11.3%) had the most outbreak cases (Table 1).

Monthly raw and smoothed
The patterns of mean IRs overtime were similar to the patterns of cases (Fig. 2). Overall, mean IRs for Campylobacter, Salmonella, Yersinia, and VTEC infections were highest in children 0–4 years old, whereas the mean IRs of Listeria infections were highest in older adults ≥60 years old (Fig. 3). Higher mean rates of Campylobacter were observed in males versus females (29.7 vs. 23.4 per 100,000 person-years, respectively); no other differences by sex were statistically significant (Table 2 and Fig. 4).
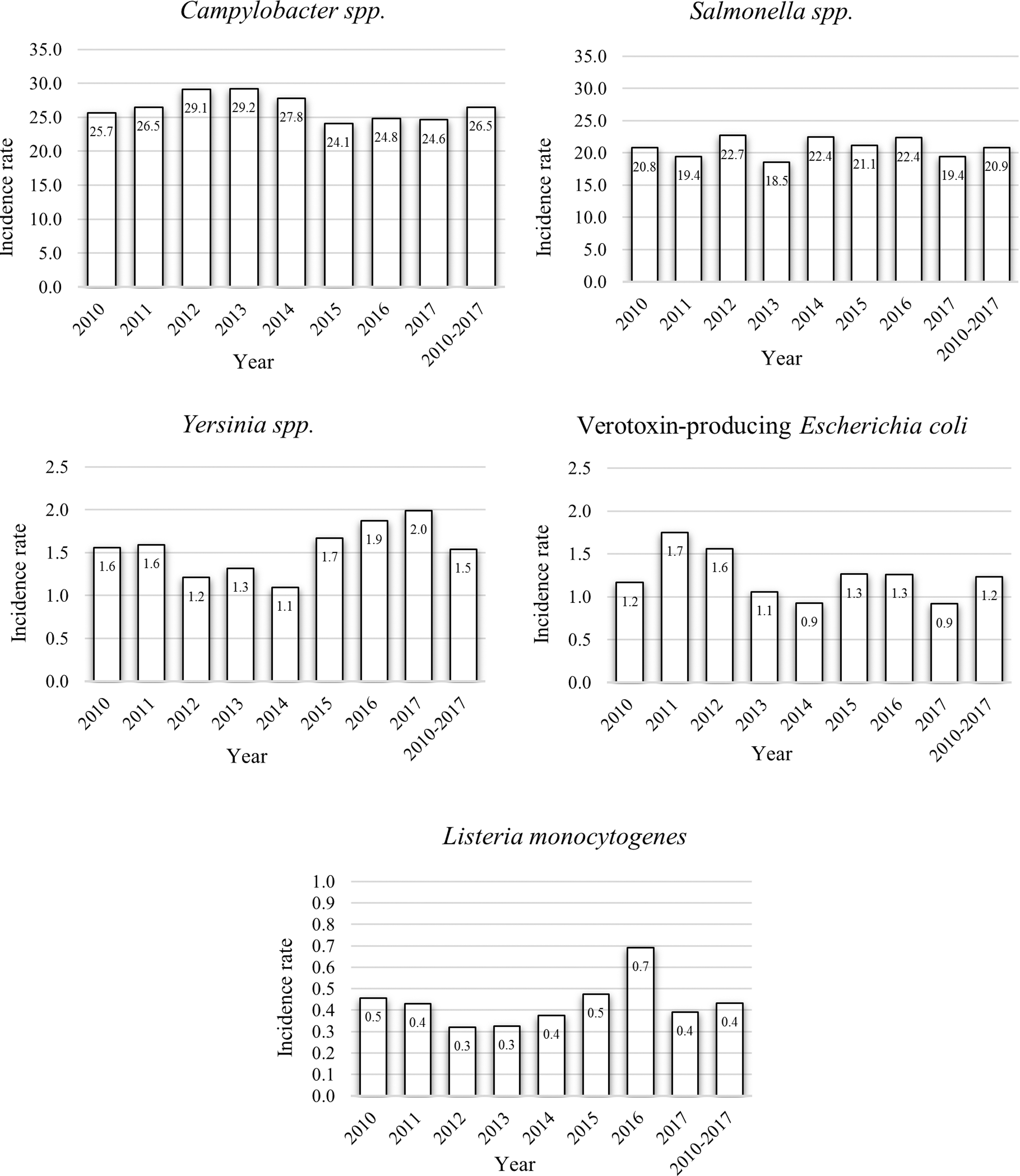
Annual and mean incidence rates, in 100,000 cases per person-year, of major enteric diseases in Ontario, Canada (2010–2017).
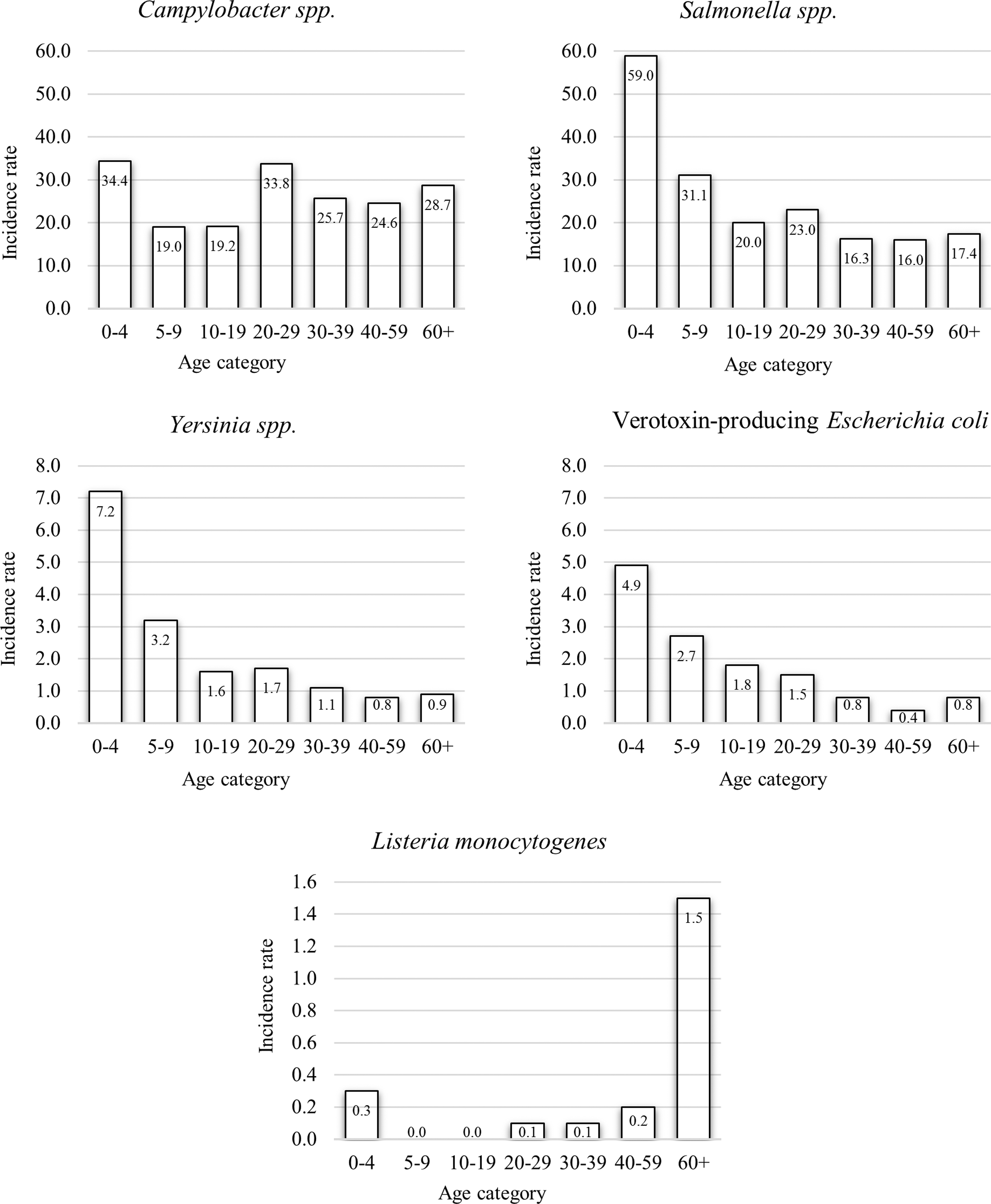
Age-specific mean incidence rates, in 100,000 cases per person-year, of major enteric diseases in Ontario, Canada (2010–2017).

Sex-specific annual and mean incidence rates, in 100,000 cases per person-year, of major enteric diseases in Ontario, Canada (2010–2017), with 95% confidence interval error bars.
Incidence Rate Ratios from the Multivariable Models with 95% Confidence Intervals, by Factor, for Five Enteric Diseases in Ontario, Canada, 2010–2017 (N = 54,853 Cases)
Significant values are shown in bold.
Negative binomial model.
Poisson model.
—, Reference group; n/a, not applicable; interaction terms excluded from models.
CI, confidence interval; IRR, incidence rate ratio.
Adjusting for season, age, sex, and the interaction between age and sex, the highest IR occurred in 2012 and 2013 for Campylobacter, 2012 for Salmonella, 2017 for Yersinia, 2011 for VTEC, and 2016 for Listeria infections. Infections caused by these five pathogens had the highest IRs in summer, with the highest IRR (4.07) observed in VTEC. The lowest IRs were observed in winter for Campylobacter, VTEC, and Listeria, and in fall for Salmonella and Yersinia.
Children 0–4 years old had the highest IRs for Campylobacter, Salmonella, Yersinia, and VTEC, and adults ≥60 years had the highest IR for Listeria (4.4 times the rate compared with children 0–4 years old). Overall, the IR was 0.7 times lower in females than males for Campylobacter; no other sex differences were significant. However, we found significant interactions between certain age groups and sex for Campylobacter, Salmonella, and VTEC infections. For example, among those 10–19 years old, the IRs of Campylobacter and Salmonella infections were significantly higher in males than females. The IRs of VTEC infection were significantly higher in females 30–39 and 40–59 years old compared with males in the same age groups. No significant interaction was observed for Yersinia and Listeria infections (Table 2).
Discussion
The study describes and compares the incidence, seasonality, and demographic factors, of five major causes of enteric infections in Ontario. The distribution varied by pathogen, with Campylobacter and Salmonella infections making up the majority of cases, similar to other studies from Ontario (Vrbova et al., 2012; Drudge et al., 2019), other parts of Canada (Thomas et al., 2013; Valcour et al., 2016), and other countries (Scallan et al., 2011; OzFoodNet Working Group, 2018).
Although there were no annual trends in cases over time, there were observed differences in annual infection rates, which can be explained by climatic variations and fluctuations in regional temperature and precipitation (Arsenault et al., 2012; Lal et al., 2013), different demographics (Chang et al., 2009; Arsenault et al., 2012; Varga et al., 2013b), immigration and travel (Kendall et al., 2012; Tighe et al., 2012), or disease outbreaks (Hanson et al., 2019; Self et al., 2019).
All five infections in our study were elevated in summer, consistent with other studies (Vrbova et al., 2012; Varga et al., 2013b; Valcour et al., 2016). This may be due to the increased outdoor activities, such as travel (Kendall et al., 2012; Tighe et al., 2012), and the higher proliferation of pathogens in food products and farm environments in warm weather, which can result in disease outbreaks (Kozak et al., 2014; Stein and Katz, 2017). Our results showed that some cases were linked to outbreak events for all the infections, with Salmonella, VTEC, and Listeria having the highest proportions of outbreak-related cases, in line with a previous study in Ontario (Vrbova et al., 2012).
We observed higher rates of enteric infections in children 0–4 years old and adults ≥60 years old, consistent with other studies from Ontario (Majowicz et al., 2007; Vrbova et al., 2012; Varga et al., 2013b), the United States (Chang et al., 2009; Barkley et al., 2016), and the United Kingdom (Gillespie et al., 2008). This was expected given that these age groups are more susceptible to infections due to their inherent vulnerabilities resulting from developing or weakened immune systems (Barkley et al., 2016). Poor hygiene practices (e.g., lack of hand-washing before eating or after visiting the toilet) are also important factors for the higher rates of enteric infections in children 0–4 years old (Karambu et al., 2013).
Our analysis showed age-dependent sex differences in infection rates for Campylobacter, Salmonella, and VTEC, but not for Yersinia or Listeria. There were higher rates of Campylobacter and Salmonella infections in young males (10–19 years) than in young females and higher rates in women (≥20 years) than in men. Similar to our findings, Sodha et al. (2015) determined that VTEC infection rates were higher in women aged 20–29 years and older in the United States. Researchers in England and Wales (Gillespie et al., 2008) also reported higher Campylobacter infection rates in women between 20 and 36 years old.
The higher rates of these infections in women (compared with men) may be due to greater person-to-person contact with young children in the household. Women are also more likely to be exposed to these pathogens during food preparation given that these pathogens are mostly foodborne (Thomas et al., 2013), and women are generally more engaged in food preparation activities than men in Canada (Moyser and Burlock, 2018). Different sources of infections and different transmission routes (Butler et al., 2015), age (Gillespie et al., 2008), existing health conditions (Barkley et al., 2016), and medical care-seeking behaviors (Blackwell et al., 2009) have also been proposed as explanations for these sex-related health disparities, and we hypothesized that these factors influenced the results observed in our study.
In contrast to our findings, a meta-analysis of population data on reported cases of Campylobacter infections obtained from seven countries, including Canada, determined that infection rates were higher in males than females of all ages (Green et al., 2020). Several factors could be responsible for the contrast in this finding and our results. The effects of under-reporting and variations in laboratory test methods on infection rates across different regions are well known (Majowicz et al., 2005; Amaku et al., 2017). Exposure sources, behavioral, cultural, and socioeconomic factors (Gillespie et al., 2008; Butler et al., 2015; Shaw et al., 2016), as well as biological factors (van Lunzen and Altfeld, 2014) are all important determinants of age- and sex-specific infection rates.
Although other researchers in Canada and the United States observed no significant sex differences for Salmonella infections (Younus et al., 2006; Vrbova et al., 2012; Varga et al., 2013b), it was interesting to observe in our study that only infants and young children (<10 years old) have the same rate of Salmonella and Campylobacter infections regardless of sex, suggesting that factors apart from biological or genetic ones might play a role in the manifestations of these infections.
Strengths and limitations
We detected demographic and seasonal variations among the major enteric infections in Ontario. There are several individual-level factors such as personal hygiene, food-handling practices, and high-risk food consumption behaviors that might explain the higher rates in specific groups of individuals, and during specific periods such as in summer. Knowing the demographic factors and seasonal patterns of infections caused by the five major pathogens in Ontario might inform community-focused policy-making initiatives. Our study will also aid public health authorities in the evaluation and implementation of disease prevention and control measures to mitigate the health burden of enteric infections in Ontario.
Findings from our study should be interpreted in light of the limitations inherent to the use of passive surveillance data that do not represent the true burden of diseases in the general population due to factors such as under-reporting and under-diagnosis in different populations, different regions, and across times. These can be due to differences in health care-seeking behavior, accessibility to health care, failure to obtain stool samples by physicians, inadequate or lack of diagnostic tools, inaccurate diagnosis, or rate of reporting along the administrative chain (Majowicz et al., 2005; Amaku et al., 2017), which could result in an underestimation of the number of cases in our study.
Despite the limitations, our study provides a retrospective depiction of the epidemiology of the major enteric infections in Ontario, especially Yersinia and Listeria infections that had not been previously studied in Ontario or Canada.
Conclusion
This study investigated the incidence, seasonality, and demographic factors of Campylobacter, Salmonella, Yersinia, VTEC, and Listeria infections, in Ontario, Canada. Overall, we identified higher infection rates in young children and older adults known for their vulnerabilities to many infectious diseases. We noticed significant age- and sex-specific differences in infection rates for Campylobacter, Salmonella (higher in young and older women compared with men in the same age groups), and VTEC (higher in young women than in young men), and none for Yersinia or Listeria.
To our knowledge, the age- and sex-specific differences (or lack thereof) in IRs of Salmonella, Yersinia, and Listeria infections observed in our study have not been previously identified in Ontario. Infections from these five major pathogens peaked in the summer months, which may have been driven by disease outbreaks during this period. Further research is required to determine the local environmental and socioeconomic factors that may be responsible for the pathogen-specific disease distributions we observed in our study. Public health interventions should focus on these factors to significantly reduce infection risks.
Footnotes
Acknowledgment
The authors wish to acknowledge Public Health Ontario for providing the surveillance case data used for our study.
Disclosure Statement
No competing interests exist.
Funding Information
No funding was received.